Article Text

Abstract
Background and purpose Higher admission serum glucose levels have been associated with poor outcomes in patients with acute ischemic stroke (AIS) treated with IV thrombolysis. We sought to evaluate the association of admission serum glucose with early outcomes of patients with emergent large vessel occlusion (ELVO) treated with mechanical thrombectomy (MT).
Methods Consecutive AIS patients due to ELVO treated with MT in three tertiary stroke centers were evaluated. The following outcomes were documented using standard definitions: symptomatic intracranial hemorrhage (sICH), complete reperfusion, mortality, functional independence (modified Rankin Scale (mRS) score of 0–2), and functional improvement (shift in mRS score) at 3 months. The association of admission serum glucose and admission hyperglycemia (>140 mg/dL) with outcomes was evaluated using univariable and multivariable binary and ordinal logistic regression models.
Results 231 AIS patients with ELVO (mean age 62±14 years, 51% men, median admission National Institute of Health Stroke Scale score 16 points (IQR 12–21), median admission serum glucose 125 mg/dL (IQR 104–162)) were treated with MT. Admission hyperglycemia was associated with a lower likelihood of functional improvement (common OR 0.53; 95% CI 0.31 to 0.97; p=0.027) and higher odds of 3 month mortality (OR 2.76; 95% CI 1.40 to 5.44; p=0.004) in multivariable analyses adjusting for potential confounders. A 10 mg/dL increase in admission blood glucose was associated with a higher likelihood of sICH (OR 1.07; 95% CI 1.01 to 1.13; p=0.033) and 3 month mortality (OR 1.07; 95% CI 1.02 to 1.12; p=0.004) in multivariable models. There was no association between admission serum glucose or hyperglycemia and complete reperfusion.
Conclusions Higher admission serum glucose and admission hyperglycemia are independent predictors of adverse outcomes in ELVO patients treated with MT.
- Stroke
- Thrombectomy
Statistics from Altmetric.com
Introduction
Hyperglycemia is common in acute ischemic stroke (AIS), even in non-diabetic states secondary to stress mediated release of cortisol and norepinephrine.1 Admission hyperglycemia has been associated with poor outcomes in AIS patients treated with IV thrombolysis (IVT).2 ,3 Hyperglycemia has been shown to exacerbate brain injury by enhancement of intracellular acidosis in ischemic penumbra, which in turn leads to mitochondrial dysfunction and energy failure.4 In addition, hyperglycemia can also impair cerebral autoregulation, predisposing to reperfusion injury and potential hemorrhagic transformation of infarcts treated with tissue plasminogen activator (tPA).5 Moreover, hyperglycemia has been linked to exacerbation of ischemic brain injury through free radical formation and worsening of cerebral edema through matrix metalloproteinase 9 activation.6 ,7 There are contradictory findings regarding the potential interaction of early tPA induced recanalization on the association of admission hyperglycemia with detrimental outcomes in AIS.3 ,8
Mechanical thrombectomy (MT) improves functional outcomes of AIS patients with emergent large vessel occlusion (ELVO), particularly in those with good collaterals.9–12 There are limited data evaluating the relationship of admission hyperglycemia with early outcomes of patients with ELVO treated with MT.13 Interestingly, the potential unfavorable effects of hyperglycemia in relation to early reperfusion can be studied better in AIS patients treated with MT due to the higher achieved reperfusion rates in comparison with tPA.14 ,15
In view of former considerations, we sought to evaluate the association of admission hyperglycemia with early efficacy (complete reperfusion and functional improvement) and safety (symptomatic intracranial bleeding and mortality) outcomes in patients with ELVO treated with MT. In addition, we assessed the potential interaction of reperfusion on the association of admission serum glucose with early functional outcomes.
Methods
We performed a retrospective analysis of previously prospectively collected database of consecutive patients with ELVO who underwent MT at a tertiary care stroke center from January 2012 to June 2015 (217 patients).16–19 Additionally, consecutive ELVO patients who underwent MT at two other tertiary centers from January 2015 to June 2015 were added (14 patients). We included AIS patients with CT angiography (CTA) confirmed large vessel occlusions, who presented within 6 hours of symptom onset and underwent MT. For patients presenting between 6 and 12 hours from symptom onset, additional imaging selection criteria were used, such as Alberta Stroke Program Early CT Score (ASPECTS) ≥6 on CT head and/or good collaterals on CTA.16–19 CT and CTA were performed on a 64 slice scanner. CT slice thickness was 1.25 mm with acquisitions in axial, sagittal, and coronal planes with three-dimensional reformations. Blinded neuroradiologists (AC, GM) calculated ASPECTS20 and CTA collateral scores, as previously described.16 ,17 Collateral scores were reported in a dichotomized fashion (good vs poor collaterals) for anterior circulation ELVO using a methodology that has been shown to predict clinical outcome.21
Stroke severity at hospital admission was documented using the National Institute of Health Stroke Scale (NIHSS) score by certified vascular neurologists. Baseline characteristics, including demographics, vascular risk factors, admission NIHSS score, admission ASPECTS, pretreatment with IVT, admission serum glucose, admission hyperglycemia, admission systolic blood pressure, and diastolic blood pressure levels, were recorded as previously described. Hyperglycemia on hospital admission was defined as admission serum glucose >140 mg/dL, as previously described.13 ,22
Successful reperfusion at the end of the endovascular procedure was defined by Thrombolysis in Cerebral Infarction (TICI) scores of IIb or III.23 TICI scores were obtained from the reports of endovascular specialists (LE, ASA, DH). Symptomatic intracranial hemorrhage (sICH) was defined as the presence of a parenchymal hematoma type 2 (PH-2) on brain CT and/or MRI gradient recall echo sequence accounting for deterioration, with an increase in NIHSS score of ≥4 points within 36 hours from treatment.24 Functional outcome was evaluated at 3 months using the modified Rankin Scale (mRS) score. Functional improvement was assessed by the shift in the distribution of 3 month mRS score,25 while functional independence was defined as a 3 month mRS score of 0–2.19 The mRS scores were obtained either from a post hospital discharge clinic follow-up or from a hospital visit. Both endovascular specialists and NIHSS/mRS certified assessors of stroke severity and functional outcomes were unaware of the purposes of the study and performed treatments and assessments as part of their clinical duties. The study was approved by the institutional review boards of the participating centers (10-01003-XP).
Statistical analyses
Continuous variables are presented as mean±SD (normal distribution) and as median with IQR (skewed distribution). Categorical variables are presented as percentages with their corresponding 95% CIs. Statistical comparisons between two groups were performed using the χ2 test or, in the case of small expected frequencies, Fisher's exact test. Continuous variables were compared using the unpaired t test or the Mann–Whitney U test, as indicated. The distribution of the mRS score at 3 months among ELVO patients was compared between different AIS subgroups (with and without admission hyperglycemia) using both the Cochran–Mantel–Haenszel test and univariable/multivariable ordinal logistic regression (Rankin shift analysis).25 Univariable and multivariable binary logistic regression models were used to evaluate associations between admission serum glucose (evaluated as a continuous variable) or admission hyperglycemia (evaluated as a dichotomous variable) with 3 month functional independence, 3 month mortality, and sICH, before and after adjusting for all baseline characteristics. A cut-off of p<0.1 was used to select variables for multivariate analysis.
In addition, historical variables known to influence stroke outcome were included in a secondary multivariable analysis. Moreover, we also performed additional sensitivity univariable/multivariable logistic regression analyses for all outcomes of interest using collateral score as an independent prediction variable. Complete reperfusion was excluded per se from the aforementioned sensitivity analyses, due to the known correlation with collateral score26 ,27 and the possibility of multicollinearity.28 Associations are presented as ORs with corresponding 95% CIs. Statistical significance was achieved if p≤0.05 in multivariable logistic regression analyses.
Finally, we evaluated the interaction of reperfusion on the association of admission serum glucose or admission hyperglycemia with 3 month functional independence. The Statistical Package for Social Science (SPSS Inc, V.22.0 for Windows) was used for statistical analyses.
Results
Our study population consisted of 231 AIS patients with ELVO (mean age 62±14, 51% men, median NIHSS score 16 points (IQR 12–21), median admission serum glucose 125 mg/dL (IQR 104–162)) who were treated with MT (median onset to groin puncture 228 min (IQR 178–288)). Baseline characteristics of the study population are presented in the online supplementary table I.
supplementary tables
A total of 71 patients (31%) had a history of diabetes mellitus while 88 patients (38%) had admission hyperglycemia (47 diabetic and 41 non-diabetic). Online supplementary table II compares baseline demographic and clinical variables of ELVO patients with or without admission hyperglycemia. Patients with admission hyperglycemia were more likely to have a history of diabetes mellitus (53% vs 18%, p<0.0001), and presented with higher admission blood glucose levels (median (IQR) 178 (156–211) vs 109 (95–121) mg/dL; p<0.001) compared with patients with no hyperglycemia at admission.
Of 231 AIS patients, 35 had internal carotid artery occlusions (15%), 111 had middle cerebral artery M1 occlusions (48%), 20 patients had M2 middle cerebral artery occlusions (9%), 24 patients had tandem occlusions (10%), and the remaining 41 patients had posterior circulation occlusions (18%—14% with basilar artery occlusions, 2% with posterior cerebral artery occlusions, and the remaining 2% with vertebral artery occlusions).
In our cohort, a combination of distal aspiration and stent-triever was used as the most common technique (also called the ‘solumbra’ technique) in 122 cases (53%). The second most commonly employed technique was A Direct Aspiration First Pass Technique (ADAPT), and this was used in 54 cases (23%). Stent-trievers without distal aspiration were used in 35 cases (15%). The remaining cases were mostly cervical or intracranial carotid occlusions in which acute angioplasty and/or stenting was employed. Systemic thrombolysis prior to MT was administered in 145 patients (63%). Successful reperfusion (TICI IIb or III) was achieved in 154 patients (67%). sICH occurred in 15 patients (7%), while the 3 month functional independence and mortality rates were 50% and 25%, respectively.
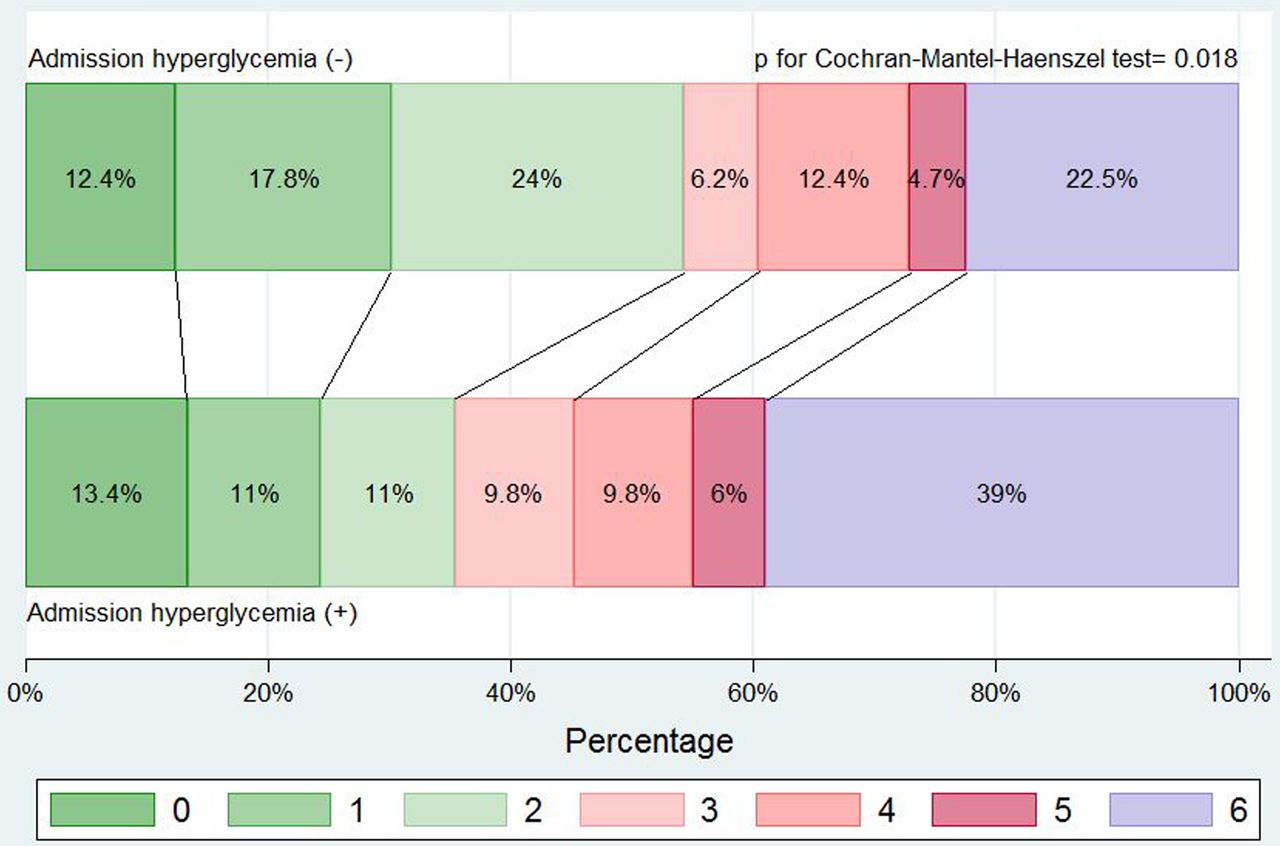
Table 1 summarizes the univariable associations of admission serum glucose or admission hyperglycemia with outcomes. Higher median admission serum glucose values were documented in patients with sICH (175 mg/dL (IQR 113–198) vs 124 mg/dL (IQR 103–157); p=0.048), without 3 month functional independence (133 mg/dL (IQR 107–183) vs 119 mg/dL (IQR 101–154); p=0.008) and who did not survive during the 3 month follow-up period (148 mg/dL (IQR 112–185) vs 119 mg/dL (IQR 103–155); p=0.004). Patients with admission hyperglycemia had higher 3 month mortality (36% vs 19%; p=0.005) and lower 3 month functional independence (40% vs 56%; p=0.005) rates. The prevalence of sICH tended to be higher in patients with admission hyperglycemia (10% vs 4%; p=0.071). Patients without admission hyperglycemia had greater functional improvement at 3 months (p=0.018 by Cochran–Mantel–Haenszel test) according to the distribution of the mRS scores (figure 1). There was no association (p>0.7) between admission serum glucose or admission hyperglycemia and complete reperfusion. Similarly, we documented no relationship (p>0.3) between admission serum glucose or admission hyperglycemia and good collateral status.
Association of serum glucose levels and hyperglycemia state (>140 mg/dL) with safety and efficacy outcomes (univariate analysis)
{kind=link}
Correlation of admission hyperglycemia and functional improvement (Cochran–Mantel–Haenszel test) according to the distribution of the modified Rankin Scale score at 3 months.
Table 2 shows the associations of admission serum glucose with sICH in univariable and multivariable binary logistic regression analyses. A 10 mg/dL increase in admission serum glucose was an independent predictor of a higher likelihood of sICH (OR 1.07; 95% CI 1.01 to 1.13; p=0.033) on multivariable logistic regression models adjusting for potential confounders. The associations of admission hyperglycemia with sICH are presented in the online supplementary table III. Admission hyperglycemia was not associated with odds of sICH in the final multivariable model (OR 2.54; 95% CI 0.77 to 8.38; p=0.125).
Univariable and multivariable logistic regression analyses depicting the associations of admission serum glucose and other baseline characteristics with symptomatic intracranial hemorrhage
Table 3 shows the associations of admission hyperglycemia with 3 month functional improvement in univariable and multivariable ordinal logistic regression analyses. Admission hyperglycemia was associated with a lower likelihood of functional improvement at 3 months (common OR 0.53; 95% CI 0.31 to 0.97; p=0.027) on multivariable ordinal logistic regression models adjusting for potential confounders. The associations of admission serum glucose with functional improvement on univariable and multivariable ordinal logistic regression analyses are presented in the online supplementary table IV. A 10 mg/dL increase in admission serum glucose tended to be associated with lower odds of functional improvement at 3 months (common OR 0.96; 95% CI 0.92 to 1.01; p=0.068) on multivariable ordinal logistic regression models adjusting for potential confounders.
Univariable and multivariable ordinal logistic regression analyses depicting the associations of admission hyperglycemia and other baseline characteristics with improvement in 3 month functional outcome (shift in modified Rankin Scale score)
The univariable and multivariable associations of admission serum glucose and admission hyperglycemia with 3 month functional independence are displayed in the online supplementary tables V and VI, respectively. A 10 mg/dL increase in admission serum glucose tended to be associated with lower odds of 3 month functional independence (OR 0.95; 95% CI 0.90 to 1.01; p=0.097) on multivariable binary logistic regression models adjusting for potential confounders. Similarly, admission hyperglycemia tended to be associated with lower odds of 3 month functional independence (OR 0.53; 95% CI 0.28 to 1.02; p=0.059) on multivariable binary logistic regression models adjusting for potential confounders.
The univariable and multivariable associations of admission serum glucose and admission hyperglycemia with 3 month mortality are displayed in the online supplementary table VII and in table 4, respectively. A 10 mg/dL increase in admission serum glucose was independently associated with a higher odds of 3 month mortality (OR 1.07; 95% CI 1.02 to 1.12; p=0.004) on multivariable binary logistic regression models adjusting for potential confounders. Also, admission hyperglycemia was an independent predictor of a higher likelihood of 3 month mortality (OR 2.76; 95% CI 1.40 to 5.44; p=0.004) on multivariable binary logistic regression models, adjusting for potential confounders. There was no interaction of complete reperfusion on the association of admission hyperglycemia (p=0.467) or admission serum glucose (p=0.426) with 3 month functional independence.
Univariable and multivariable logistic regression analyses depicting the associations of admission hyperglycemia and other baseline characteristics with 3 month mortality
In addition to blood glucose levels and admission hyperglycemia, a 10 mm Hg increase in systolic blood pressure was an independent predictor of deterioration in functional outcomes at 3 months (p<0.001) and 3 month mortality (p=0.014) in multivariable logistic regression models (tables 2, 3). Additionally, a 1 point decrease in ASPECTS on admission CT (p=0.034) and a history of coronary artery disease were independently associated with an increased risk of sICH (p=0.004) (table 1). There was no difference in the outcomes with the secondary multivariable analysis, including historically significant stroke variables.
Similarly, no differences were detected in the multivariable logistic regression analyses after introducing collateral score as an independent predictor variable on the outcomes of interest (see the online supplementary table VIII).
Discussion
Our study demonstrated that admission hyperglycemia was associated with a higher likelihood of 3 month mortality and lower odds of 3 month functional improvement in terms of shift in mRS score in ELVO patients treated with MT. The former association was independent of demographics, vascular risk factors, baseline stroke severity and early hypodensity on brain CT, admission blood pressure levels, pretreatment with IVT, and complete reperfusion at the end of the endovascular procedure. In addition, we detected an independent association of increasing admission serum glucose levels with a higher risk of sICH and 3 month mortality. The initial univariable relationships of admission hyperglycemia and admission serum glucose with 3 month functional independence (defined as mRS scores of 0–2) did not retain their significance in the final multivariable analyses, while admission hyperglycemia or admission serum glucose was not associated with the likelihood of complete reperfusion at the end of MT.
A recent post hoc analysis of SWIFT (Solitaire flow restoration device vs the Merci Retriever in patients with AIS) trial demonstrated that admission hyperglycemia was an independent predictor of lower odds of 3 month excellent functional outcome (defined as mRS scores of 0–1) in 143 ELVO patients treated with MT.13 The negative effects of admission hyperglycemia on 3 month functional status were exacerbated in patients with incomplete reperfusion. Admission hyperglycemia or admission serum glucose levels were not associated with the odds of sICH, complete reperfusion, 3 month mortality, and 3 month good functional outcome (defined as mRS scores of 0–2). The partial discrepancies between the findings of our group and SWIFT investigations in terms of 3 month mortality, sICH, and the interaction of reperfusion on the association of admission hyperglycemia with 3 month good functional outcome could be attributed to methodological disparities between the two studies. More specifically, SWIFT was a randomized trial in contrast with our observational study. Furthermore, our sample size was larger (n=231) than the SWIFT subanalysis (n=143). Also, complete reperfusion was defined in SWIFT using Thrombolysis in Myocardial Infarction, while we used the TICI scale to define reperfusion status. We preferred to use the TICI grading system in view of a recent expert opinion paper highlighting TICI as the best defined and widely used classification scheme.29
Interestingly, our findings are in line with the results of a Swiss study that evaluated the association of admission serum glucose levels with early outcomes in ELVO patients treated with IA thrombolysis.30 Increasing admission serum glucose levels were independently associated with higher odds of sICH and poor functional outcomes (defined as mRS scores of 0–2), while no association was documented between admission serum glucose and successful recanalization.30 The findings of the recently published study from MR CLEAN pre-trial registry where admission hyperglycemia (admission glucose >7.8 mmol/L) and impaired fasting glucose (>5.5 mmol/L) in the first week of admission were associated with unfavorable short term outcomes and a higher risk of sICH after MT for AIS, further corroborate our observation.31 However, in their study, functional outcomes were assessed on discharge, while we used mRS score at 3 months to report functional outcomes. Additionally, we did not have data on fasting blood glucose levels and could not assess its impact on outcome variables after MT.
Our observations are in line with the existing literature that has demonstrated the association of admission hyperglycemia with adverse outcomes in AIS patients treated with IVT. More specifically, admission hyperglycemia has been correlated with a higher risk of sICH in different risk prediction scores32 ,33 and lower odds of tPA induced recanalization3 in patients treated with systemic thrombolysis, while increasing admission serum glucose levels have been correlated with more extensive final infarct volumes.8 ,22 Also, admission hyperglycemia has been identified as an independent predictor of poor 3 month functional outcome and early mortality in different cohorts of AIS patients treated with IVT.34 Whether the impact of hyperglycemia can be attenuated with admission treatment to <140 mg/dL remains unknown, although this is an important area for future investigation, and methods will need to be incorporated into the current time sensitive paradigm for rapid MT treatment.
Several limitations of the present report need to be acknowledged. We did not obtain serial serum glucose measurements and were therefore unable to assess the impact of peri-procedural or post-procedural hyperglycemic status on final outcomes. Moreover, we did not evaluate the association of hyperglycemia treatment with early outcomes of ELVO patients treated with MT. Also, the lack of statistical significance (p=0.059) in the association between admission hyperglycemia and lower likelihood of 3 month functional independence on the multivariable analyses may be attributed to the moderate sample (n=231) of our study population.
In addition, we did not collect hemoglobin A1c (HbA1c) levels and could not correlate levels of HbA1c with blood glucose levels at presentation. Moreover, it should be acknowledged that there are inconsistencies in the results correlating admission blood glucose or admission hyperglycemia with different outcome measures and in the associations of ASPECTS score, age, and admission NIHSS score found in the univariable and multivariable regression analyses. These inconsistencies observed in the logistic regression analyses can probably be explained by the moderate sample size of our study, resulting in substantial within-group and between-group variation, and the multiple variables tested in multivariable models.35
Finally, the observational study design did not allow us to establish a cause–effect relationship between baseline hyperglycemia and poor outcomes in ELVO patients treated with MT. However, our highly experienced multicenter investigators, and our observational methods, make our findings compelling. Our multicenter approach to MT for AIS patients with ELVO reflects the experience of everyday clinical practice.
In conclusion, our observations underline the fact that admission hyperglycemia or higher admission serum glucose levels are related to worse outcomes in ELVO patients treated with MT. This association is independent of potential confounders and is not mediated by reperfusion status following the termination of IA procedures. These findings emphasize the importance of careful management of serum glucose before, during, and after endovascular reperfusion therapies in AIS patients with proximal intracranial occlusions.
References
Footnotes
NT and GT contributed equally to this study.
A portion of this study's findings have been presented at the World Stroke Conference 2016.
Contributors NG: study concept and design, acquisition of the data, analysis and interpretation, and critical revision of the manuscript for important intellectual content. GT: analysis and interpretation, and critical revision of the manuscript for important intellectual content. AP and KD: acquisition of the data and critical revision of the manuscript for important intellectual content. AHK, GM, JJC, RZ, DH, AS, AC, AWA, AVA, and ASA: critical revision of the manuscript for important intellectual content. LE: study concept and design, acquisition of the data, and critical revision of the manuscript for important intellectual content.
Competing interests None declared.
Ethics approval The study was approved by the institutional review board of the University of Tennessee (acute stroke registry 10-01003-XP).
Provenance and peer review Not commissioned; externally peer reviewed.