Article Text

Abstract
Background Stroke due to the release of embolic debris during the placement of a stent to correct carotid artery stenosis is a constant procedural and peri-procedural threat. The new all metal Casper stent has been created with two layers of nitinol, the inner layer of which has pores diminutive enough to prevent embolic release.
Objective To evaluate the safety, effectiveness, and utility of the double layer nitinol Casper carotid artery stent in the treatment of patients with severe carotid artery stenosis.
Methods 19 patients with severe internal carotid artery stenosis, 14 symptomatic and 5 asymptomatic, were treated with the Casper stent. After stent placement, angiographic and cone beam CT images were recorded in all patients.
Results The unique low profile delivery system allowed for easy stent placement, re-sheathing, and repositioning of the stent. The large cell external layer produced excellent apposition to the artery wall. The inner layer prevented prolapse of atherosclerotic debris through the device. Plaque coverage was achieved; residual stenosis ranged from 0% to 20%. Long term angiographic follow-up in 5 patients showed wall apposition of the device covering the lesion and no restenosis. There were no procedure related complications. Two patients experienced a delayed ischemic stroke, likely related to inconsistent medical management.
Conclusions The Casper has been an excellent stent for the treatment of internal carotid artery stenosis and its internal micromesh layer has been effective in preventing plaque prolapse. It provides the flexibility of large cell stents and the inner layer provides maximum protection against plaque prolapse.
- Stent
- Stenosis
- Plaque
- Angiography
- Device
Statistics from Altmetric.com
Introduction
With the 2008 and 2010 publication of the results of clinical trials1 ,2 comparing the effectiveness and outcomes of surgical carotid artery endarterectomy (CEA) and transcatheter endovascular carotid artery stenting (CAS) that showed no significant difference in outcomes, there has been a sustained effort at research and development by several medical device manufacturers to create the most effective and safest stenting device. Selecting the best combination of materials for flexibility, mechanical properties, and cell size for manufacture has produced a variety of stent devices with different features. The Casper stent (Microvention, Terumo, Tustin, California, USA) is a unique dual layer micromesh small cell all nitinol stent that has the added feature of being resheathable (with up to 50% deployment) for repositioning, if desired by the operating physician.
Methods
The Casper stent
The dual layer carotid artery stent is a unique all metal nitinol device. Designed for sustained embolic protection, the inner layer has fine pores measuring 375 µm (0.375 mm). The pores are so fine that the term ‘micromesh’ has been applied. The inner layer acts like a covered stent but the micromesh is inside the stent. This construction is aimed at trapping any potentially embolic material against the arterial wall. It comes in a 143 cm 5.2 F catheter with a 0.014 inch guidewire. The stents are tapered and come in diameters of 5–10 mm and lengths of 16–40 mm. The stent can be repositioned in the catheter until up to 50% has been extruded for improved positioning, as determined by the operator. Favorable results have been reported from Europe where the Casper stent is called the Roadsaver stent.3 ,4 (The Casper stent is undergoing clinical trials with the US Food and Drug Administration as the Roadsaver Stent. The protocol includes the use of an embolic protection device (EPD) and is not commercially available in the USA.)
Patients
This was a case series of 19 patients with symptomatic or asymptomatic carotid artery occlusive disease who were treated with the Casper device between March 2015 and October 2016.
Patients with a high surgical risk because of comorbid medical conditions underwent CAS with the Casper device only, and those with a low surgical risk were allowed to choose between CEA and CAS.
For each patient, information on demographics, risk factors, and clinical presentation were collected. There were 16 men and 3 women. Median age was 66 years. Hemiparesis was present in 10 patients, and amaurosis fugax, syncope, dysarthria, and vertigo were recorded in the other 4 symptomatic patients. Hypertension was present in 17 of the 19 patients.
Symptomatic patients were treated in the first 60 days after symptom presentation. Indications in the asymptomatic group included occlusion of the contralateral carotid artery and restenosis in the target vessel after CEA (see table 1). Symptomatic patients were directed to angiography, and two underwent duplex ultrasound and three cone beam CT. Therefore, there was no echolucency classification. Post-procedural MRI was reserved for symptomatic patients.
Patient characteristics
The study was conducted in accordance with our local institutional review board regulations. Written informed consent was obtained from all patients. Post-deployment angiography and cone beam CTs were obtained in all cases.
Procedural information and lesion characteristics assessed included the presence of visible thrombus, dense calcification, ulceration, target lesion location, lesion length, minimal lesion diameter, and preprocedural stenosis severity (North American Symptomatic Carotid Endarterectomy Trial (NASCET) %). Average stenosis of the treated arteries was 76.5%. All patients had an EPD placed, and all had pre-stent and post-stent balloon dilatation. There were no complications. In one patient, the pre-stent Rankin Scale score increased from 2 to 3. All others were unchanged.
Procedure
Antiplatelet therapy (aspirin 100 mg and clopidogrel (Plavix) 75 mg) was started 5 days before the procedure in all patients, and all underwent transfemoral cerebral angiography under general anesthesia. For patients in whom endovascular treatment was anticipated, the procedures were performed under general anesthesia, with an arterial line and Foley catheter. This permits easy control of the patient's blood pressure and movements (14 symptomatic patients could not follow commands). No patient experienced post-procedural arterial hypotension.
The diameter of the internal carotid artery proximal to, at, and distal to the lesion, as well as the length of the target lesion, were measured and recorded. Heparin (5000 units) was administered intra-arterially. A Spider (ev3) EPD was placed under fluoroscopy and advanced to a position 4–5 cm distal to the lesion. In 18 cases, the lesion was pre-dilated with a Maverick balloon catheter (Boston Scientific; sizes 2.5×12, 3×20,4×20, 5×20). In one case, a Sprinter Legend (Medtronic) 4×20 was used. The delivery system was then advanced under fluoroscopy and positioned with the radiopaque inner shaft markers (distal and proximal ends of the stent) distal and proximal to the target lesion. The Casper stent was then deployed under constant fluoroscopy by slowly withdrawing the delivery catheter and holding the delivery wire in a secure stationery position.
If positioning was less than ideal and the stent not more than 50% delivered, the stent could be slipped back into the catheter and the catheter repositioned for improved deployment. Post-deployment balloon dilatation of the stent was carried out in all cases with a Sterling balloon catheter 6×20 (Boston Scientific). The guidewire, balloon catheter, pusher, and EPD were removed. There was no debris found under direct inspection by two operators after flushing the EPD with saline. We believe the absence of debris may be a reflection of the effectiveness and control provided by the micromesh configuration of the stent. Finally, angiography in two projections was performed as well as cone beam CT imaging (figures 1, 2).
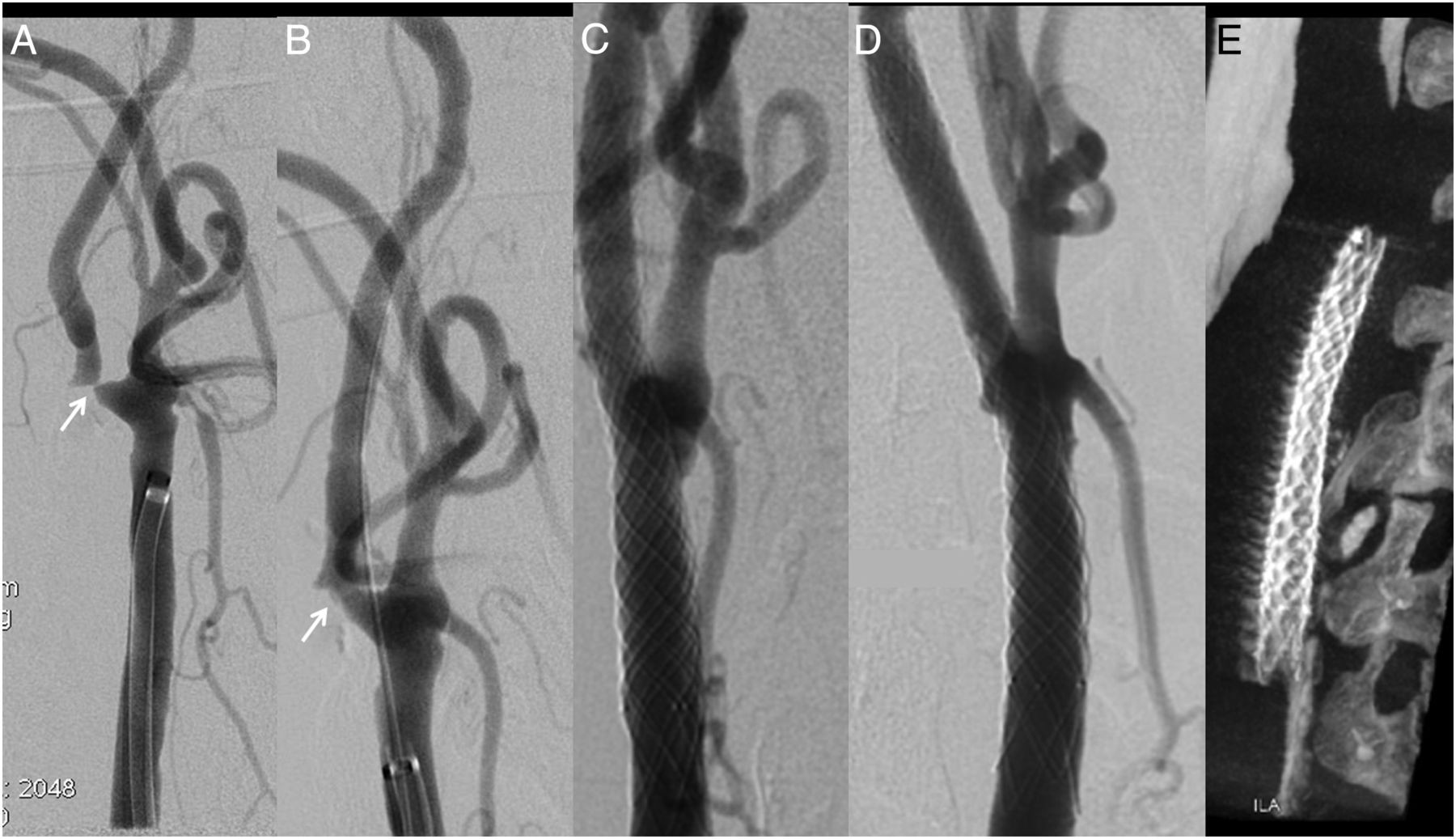
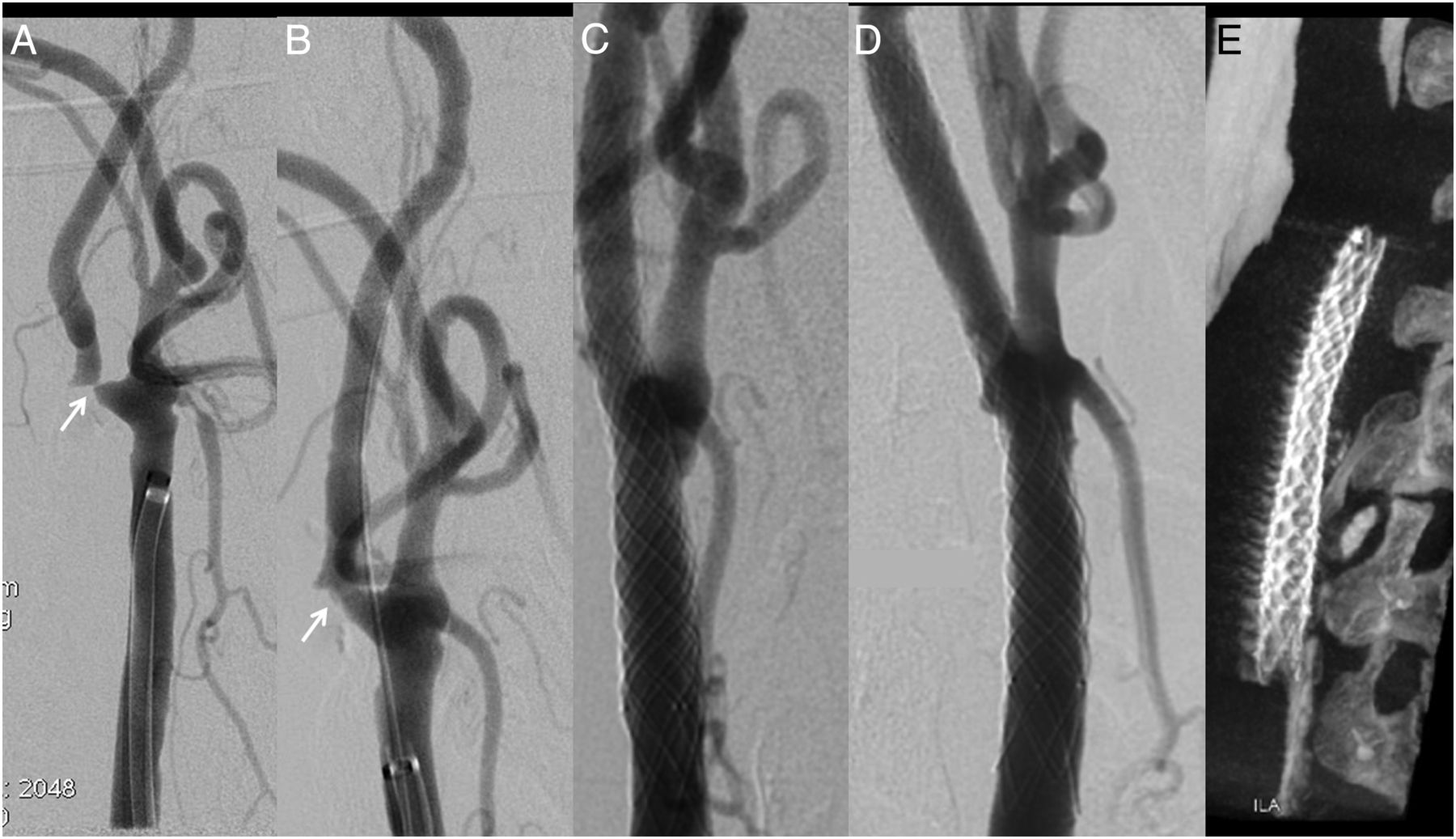
Case No 3. (A, B) Pre-stenting lateral and posteroanterior common carotid injection, showing a right internal carotid artery bulbar ulcerated atherosclerotic plaque causing near complete occlusion. The plaque extends into the distal common carotid artery (arrows). (C, D) Immediate post-Casper stent placement. Posteroanterior and lateral projections show close apposition of the stent to the wall of the artery. (E) Cone beam CT image of the expanded Casper stent dilating the stenosis and covering the plaque.

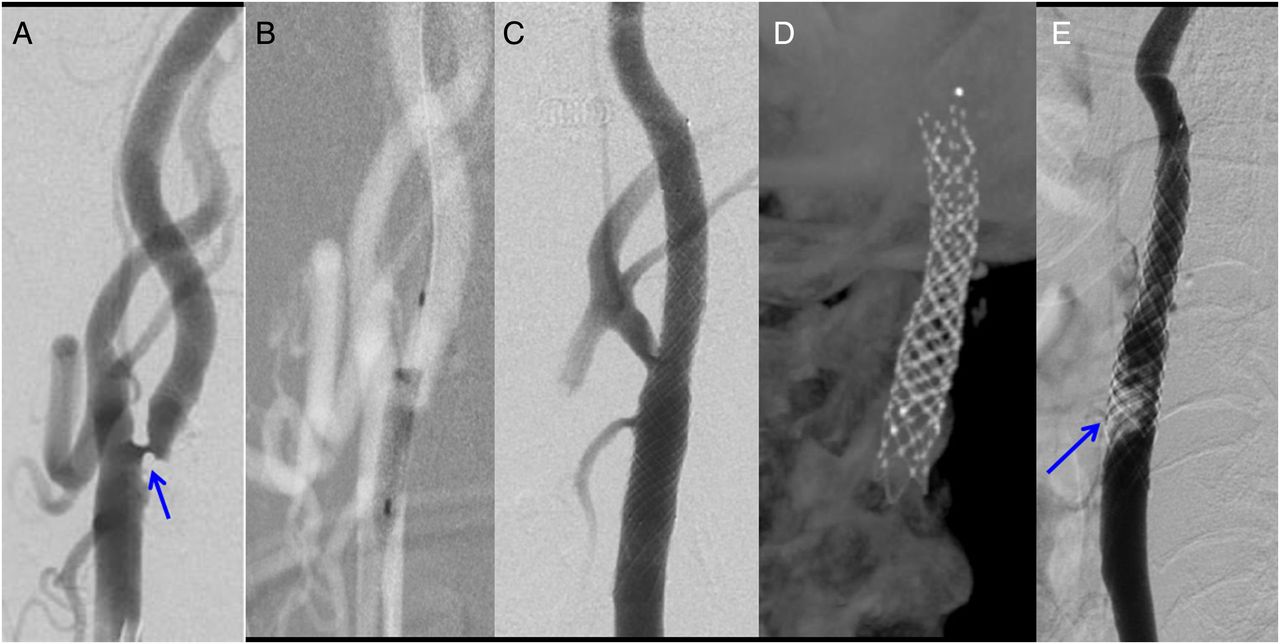
Case No 8. (A) 90% stenosis of the bulbar portion of the left internal carotid artery produced by an irregular calcific carotid plaque (arrow). (B) Balloon angioplasty prior to stenting. (C) Post-stent lateral projection with wide patency of the stented artery. (D) Cone beam CT image of the expanded Casper stent. (E) Antiplatelet therapy was stopped prior to coronary artery surgery. Hemiparesis appeared 8 days after surgery, 25 days after stent placement. In-stent thrombus (arrow) and occlusion of the external carotid artery are present on the angiogram.
Post treatment clinical follow-up was done in all cases within the first 30 days using the Rankin scale. The completeness of the use of technical tools in follow up evaluations was limited by funding. Doppler follow-up was carried out within the first 6 months in eight cases, showing no evidence of re-stenosis or occlusion of the treated vessel. Five patients underwent angiographic follow-up. Four of these patients were asymptomatic. One patient had acute hemiplegia. (figure 2). Platelet reactivity measurement (PRU-P2-Y12), was only obtained at the end of this series in five patients to monitor the response to antiplatelet therapy.
Results
Angiography and cone beam CT images obtained at the conclusion of each case showed excellent plaque coverage with residual stenosis percentages ranging between 0% and 20%. There was no kinking of any of the stents. Immediate restoration of blood flow was present in all cases on immediate post-deployment angiography. There was no distal embolization or dissection. Representative images are shown in figure 1.
There were no technical problems encountered with the device and no complications. Two patients suffered periprocedural ischemic strokes. These patients had an increased risk related to severe carotid stenosis (80% and 90%), total occlusion of the contralateral carotid artery, and multiple comorbidities. One patient developed hemiparesis after being returned to her original hospital where clopidogrel was discontinued. Fifteen days after the stenting, hemiparesis appeared. In the second patient, antiplatelet (aspirin and clopidogrel) therapy was stopped in order to perform coronary bypass surgery. Eight days later, hemiparesis developed. Carotid angiogram showed thrombus in the stent (figure 2).
Discussion
The effectiveness of CAS in the treatment of carotid occlusive disease was evident in our small series. The Casper stent was successfully deployed in every case, resulting in residual stenosis of no more than 20%. Neither restenosis nor device kinking was seen in the angiographic follow-up. Outcomes were similar to those reported in the randomized clinical trials Stenting and Angioplasty with Protection in Patients at High Risk for Endarterectomy (SAPPHIRE)1 and Carotid Revascularization Endarterectomy versus Stenting Trial (CREST),2 supporting the premise that CAS has reached ‘non-inferiority’ to carotid endarterectomy. A recent report on a randomized clinical trial (Asymptomatic Carotid Trial (ACT)) in 1453 asymptomatic patients showed that stenting with embolic protection was non-inferior to surgery at 1 year. In their analyses that included up to 5 years of follow-up, there were no significant differences between the study groups in the rates of non-procedure related stroke, all stroke, and survival.5 A recent report, the CLEAR-ROAD study, on 100 patients treated with the Roadsaver sent (aka the Casper stent) from centers in Belgium, Italy, and Germany, showed it to be “a safe and effective device for endovascular treatment of subjects at high risk for carotid endarterectomy”.6
Nevertheless, the randomized trials also demonstrated that peri-procedural (30 day) stroke was more likely after carotid stenting and myocardial infarction more likely after endarterectomy.2 The incidence of complications increases in patients with longer lesions, higher level of tortuosity, complicated plaque morphology, older age, female gender, and poor glycemic control.7 Plaque prolapse through the stent cells and intraluminal manipulation of the lesion are suggested determinants for distal embolization post-stenting. Because our patients were symptomatic and at high risk for embolization with moderate to severe stenosis and an ulcerated plaque, an EPD was used in each case. Hopf-Jensen reports on a series of seven patients successfully treated with the Casper stent without EPD and without complications.3 Although difficult to prove, the micromesh design of the Casper double layer stent provided added confidence that the risk of embolization had been minimized.
The Casper device is the first carotid stent designed with a nitinol double layer micromesh construction for sustained embolic protection. The braided nitinol construction confers the properties of shape memory and flexibility, and allows conformation to carotid anatomy while minimizing the chance of kinking. It is characterized by a closed cell design with open cell mechanical performance. The open cell external layer produces flexibility and conformability (figure 3) and the inner micromesh with its diminutive pore size allows extensive plaque coverage, minimizing the risk of plaque protrusion and embolization.
{kind=link}
{kind=link}
{kind=link}
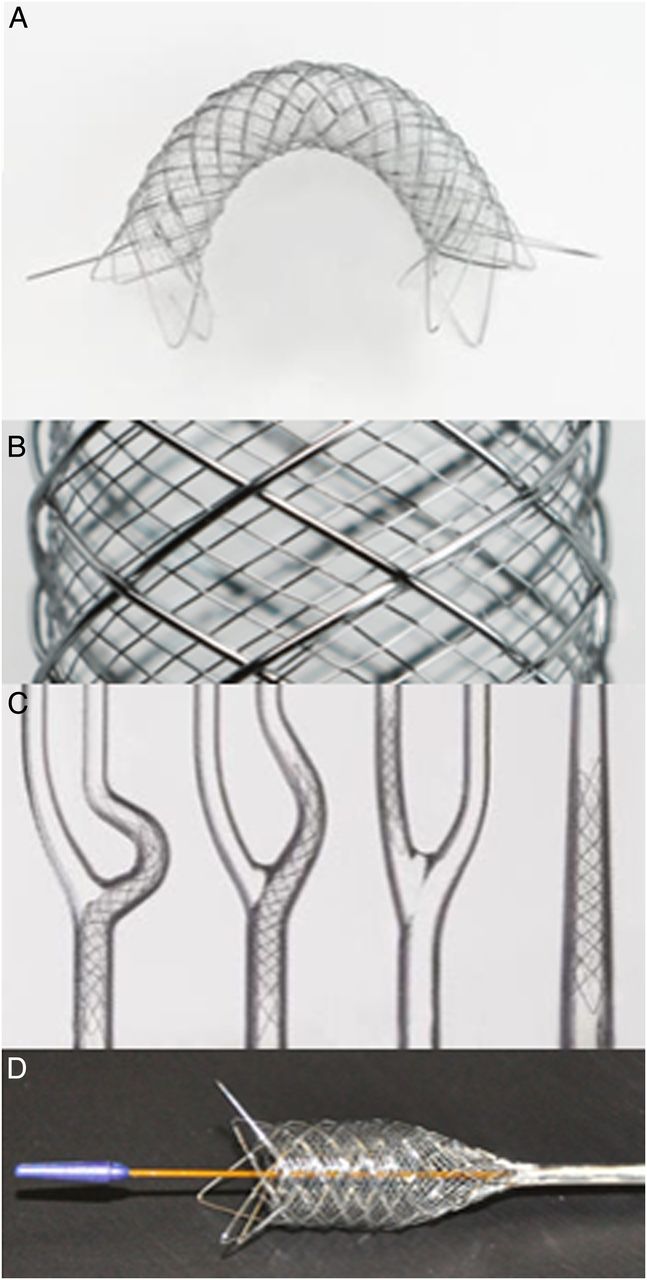
Casper device, (A) Flexibility of nitinol construction. (B) Double layer micromesh design. (C) Shape memory and conformability to carotid anatomy to minimize kinking. (D) Low profile 5.2 F rapid exchange catheter for all sizes.
This new Casper micromesh stent provides the advantage of sustained embolic protection with plaque stabilization and peri-procedural stroke prevention. These advantages are reflected in our results, with a low degree of neurologic disability and no change in the Rankin Scale score after the intervention in 90% of cases. Two clinical complications were encountered in the first 30 days in patients at very high risk. Both patients had a severe degree of stenosis, total occlusion of the contralateral carotid artery, multiple comorbidities, and did not adhere to medical management.
There were no technical complications. The low profile delivery system allowed rapid exchange for all sizes. The ability to re-sheath and reposition the stent is unique with this device and provided added comfort and confidence for the operator. Other dual layer micromesh carotid stents involved in clinical trials utilized extended polytetrafluoroethylene with nitinol (WL Gore)8 ,9 and polyethylene terephthalate with nitinol (InspireMD)9 ,10 in their dual layer construction in contrast with the all nitinol Casper stent.
Weaknesses of this paper include the small number of cases treated and the lack of long term angiographic follow-up in some cases.
Conclusion
Our clinical experience has shown excellent performance of the Casper stent for the treatment of carotid artery stenosis. The double layer micromesh stent has been designed to prevent plaque prolapse and to provide protection against emboli. Further studies with larger populations are warranted.
Footnotes
Contributors OD and AR performed all procedures and contributed to manuscript conception, design, creation, editing, and revision. JR and GL contributed to manuscript conception, design, creation, editing, and revision. GD, OF, and AR contributed to manuscript conception and design.
Competing interests None declared.
Ethics approval The study was approved by the institutional review board of Nuevo Hospital de Bocagrande, Cartagena, Colombia.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional unpublished angiographic and cone beam CT data for each case are available to readers of the journal. Please email all requests to the corresponding author.