Article Text

Abstract
Background Treatment of spinal metastatic lesions by radiofrequency ablation (RFA) before cementation can potentially help in local tumor control and pain relief. This is often limited by access and tumor location. This study reports multicenter clinical and imaging outcomes following targeted RFA (t-RFA) and cement augmentation in neoplastic lesions of the spine.
Material and methods A retrospective multicenter study of 49 patients with 72 painful vertebral lesions, evaluated for clinical and imaging outcomes following RFA and cement augmentation of spinal metastatic lesions, was undertaken. Visual Analogue Pain score (VAS) and Oswestry Disability Index (ODI) were obtained before and 2–4 weeks after treatment. Pre- and post-procedure imaging examinations including MRI and positron emission tomography (PET) were also evaluated.
Results Mean ablation time was 3.7±2.5 min (range 0.92–15). Mean VAS scores decreased from 7.9±2.5 pre-procedure to 3.5±2.6 post-procedure (p<0.0001). Mean ODI scores improved from 34.9±18.3 to 21.6±13.8 post-procedure (p<0.0001). Post-contrast MRI resulted in a predictable pattern of decreased tumor volume and an enhancing rim. Metabolically active lesions in pre-procedure PET scans (n=10 levels) showed decreased fluorodeoxyglucose activity after ablation.
Conclusions t-RFA followed by vertebral augmentation in malignant vertebral lesions resulted in significant pain reduction and functional status improvement, with no major complications. t-RFA permitted access to vertebral lesions and real-time accurate monitoring of the ablation zone temperature. Post-procedure MRI and PET examinations correlated with a favorable tumor response and helped to monitor tumor growth and the timing of adjuvant therapy.
- Spine
- Malignant
- Metastatic
Statistics from Altmetric.com
Introduction
Bone metastases are common in patients with primary malignancy. Osseous metastatic lesions have been reported in up to 80% of patients with cancer at the time of death.1 Neoplasms most frequently metastasize to the axial skeleton due to the high hematopoietic activity and vascularization of the spine.2 Traditionally, these vertebral metastases are managed through a combination of radiation therapy, chemotherapy, and analgesics. Surgical decompression and stabilization is an option for patients with neurologic deficits, instability, or a longer life expectancy.3
Radiofrequency ablation (RFA) is a known treatment option for metastases in the liver and kidney.4 ,5 Recently, RFA has been emerging as another treatment modality for the management of osseous metastatic lesions. Conventionally, spinal RFA treatment has been limited to lesions within the anterior column of the vertebral body as this location is more accessible and further away from the spinal cord and nerve roots.6 In particular, a previously reported method of spinal tumor ablation is plasma-mediated RFA. This procedure uses radiofrequency energy to excite electrolytes and create a plasma field that disrupts molecular bonds at relatively low temperatures (between 40°C and 70°C).7 ,8 As seen with this procedure, there has not been a standard method to monitor the resultant thermal profile and ablation zone during RFA procedures, imposing a potential risk of thermal injury to the spinal cord and/or nerve roots.
Vertebral augmentation has been shown to help relieve pain in patients with painful vertebral metastases by providing stabilization of the compromised vertebral body.9 ,10 RFA alone has also been used to treat solitary metastatic lesions in the spine and in long bones.11 ,12 Documented tumor extravasation and migration into adjacent vertebrae following cement augmentation for pathologic vertebral compressions fractures in patients with metastatic spine disease has raised interest in the use of tumor ablative procedures prior to augmentation in order to reduce the potential for increased pressurization that results in the mechanical displacement of viable tumor cells.13 ,14 An initial clinical study in the treatment of metastatic spinal lesions with a steerable bipolar radiofrequency device showed that it could be used in combination with vertebral augmentation to treat osseous lesions of the spine.3
This multicenter retrospective study was performed to determine the safety and clinical efficacy in terms of clinical outcomes and imaging findings after targeted RFA (t-RFA) of various metastatic lesions of the vertebral column using a steerable and articulating tumor ablation system. The articulating nature of the ablation system enables any part of the vertebral body to be reached for direct tumor debulking and, in most cases, this can be performed using a unipedicular access.
Material and methods
Demographics
After obtaining the appropriate IRB approval, a retrospective analysis involving seven centers (four USA and three European) was conducted for patients who received t-RFA as a treatment for vertebral metastases between October 2012 and July 2014. All patients received concurrent vertebral augmentation using radiofrequency-activated high viscosity polymethylmethacrylate cement. The number of patients and treated lesions were recorded, as well as the tumor type.
Procedure
Prior to each procedure, written informed consent was obtained from the patient after a detailed explanation of the treatment risks, benefits, and complications as well as treatment alternatives.
Pre-procedure planning was performed using cross-sectional imaging including MRI, CT, or both. Imaging was used to determine the number of lesions as well as the size and locations of the various metastatic foci. Images were carefully scrutinized for the presence of cortical disruption on CT or the presence of epidural tumor extension on MRI. All cases were performed under IV sedation and analgesia in order to enable monitoring of any neurologic symptoms. All procedures were performed under fluoroscopic guidance by operators experienced in image-guided percutaneous spine interventions. No electrophysiological monitoring was performed during the procedures in any of the centers.
RFA was performed with the STAR Tumor Ablation System (comprising the SpineSTAR electrode and the MetaSTAR Generator, Merit Medical, Salt Lake City, Utah, USA).15 The articulating, navigational and bipolar radiofrequency electrode contains a pair of active thermocouples positioned along the length of the electrode at 10 and 15 mm from the center of the ablation zone. The ellipsoid ablation volume is approximately 20×15×15 mm when the thermocouple located 10 mm from the center of the ablation zone reaches 50°C and 30×20×20 mm when the thermocouple 15 mm from the center of the ablation zone reaches 50°C. The generator displays the two thermocouple readings permitting real-time monitoring of the peripheral edge of the ablation zone.
All vertebral lesions were targeted from a transpedicular or, when necessary, with a parapedicular approach through a 10-gauge coaxial working cannula. The working cannula was advanced into the posterior aspect of the vertebral body. A biopsy of the pathologic vertebra was obtained when indicated (in particular to establish tumor type when uncertain). An articulating osteotome capable of crossing the axial midline was used to make targeted working channels within the vertebral body prior to ablation. After removal of the osteotome, a steerable bipolar electrode was advanced through the working cannula to a desired location within the vertebral body. A variable number of ablation zones, temperatures, and ablation times were used based on the size, shape, and location of the lesion. Ablation access was unipedicular in all levels but two. Cement augmentation was performed after removal of the bipolar electrode using high viscosity acrylic bone cement (StabiliT Vertebral Augmentation System, Merit Medical), which was delivered directly into the working cavity created by the ablation procedure immediately after ablation in the same treatment session. Visual Analogue Score (VAS) data to measure pain level and Oswestry Disability Index (ODI) data to measure function were obtained prior to the procedure and 2–4 weeks after the procedure. Pre-procedure CT examinations were available in 40 patients; 23 of these 40 patients had a post-procedure CT examination available for evaluation. Of the 37 patients who had a pre-procedure MRI available, 18 had a post-procedure MRI (10 with contrast enhancement using fat suppression technique). Ten patients had pre- and post 18F-fluorodeoxyglucose (FDG) positron emission tomographic (PET) scanning.
The patients' charts were reviewed with regard to other treatments performed at the index vertebra(e) before, during and after the ablation procedure and complications. Independent radiologists evaluated all images as part of the routine clinical evaluation. The images were further evaluated by the authors to collect all the data needed for the study. CT images were evaluated for the degree of compression, the nature of the tumor (lytic, sclerotic or mixed), and the presence of bony disruption, especially in the posterior cortex. Post-procedure images were evaluated for the location and degree of cement leakage.
MRI images were evaluated with regard to the signal characteristics of the lesions in different pulse sequences, size and location of the tumor mass, degree of compression, and the presence of any extravertebral extension-like epidural tissue or paravertebral extension. Post-procedure images were evaluated for the degree of enhancement, the size of the tumor bulk, the presence of an enhancing rim, and the presence of new findings that indicate progression of tumor-like new epidural extension.
Statistical evaluation
Patients' baseline assessments were used as controls. Analysis of pain and disability assessments were performed at visits between 2 and 4 weeks after RFA. Change from baseline was evaluated using a one-sample t-test and compared with no change. 95% CIs were calculated.
Results
All procedures were performed safely. There were no reported complications from the procedure. Specifically, no cases of thermal injury occurred in this patient cohort. One patient reported moderate sharp pain 50 s after the thermal ablation procedure was initiated. The ablation was stopped and the t-RFA probe was repositioned. Ablation was then continued with no pain or adverse effect. Table 1 summarizes the study population.
Summary of the study population and important findings
Seventy-two lesions were treated in 49 patients (34 women and 15 men). The mean age was 64.3±12.6 years. Primary tumor types included breast (n=21, 43%), lung (n=18, 37%), pancreatic, renal and prostate (n=2, 4% each), and colon, sarcoma, melanoma and urinary bladder cancer (n=1, 2% each). Levels treated ranged from T3 to L5 with T11 (14%), L1 (14%), L4 (13%), L2 (11%), and L3 (11%) the most commonly treated. The average number of vertebrae treated per patient was 1.5±0.7 (range 1–4). The average number of overlapping ablation zones per patient was 1.8±1.1 (range 1–5). The average time of ablation per vertebra was 3.7±2.5 min (range 1–15). The amount of cement injected was 2.9±1 mL (range 1–5). Nine patients underwent additional vertebral augmentation procedures at non-index vertebrae.
Nine patients had no radiation or chemotherapy to the index vertebra prior to RFA. In 11 patients the ablation treatment was performed during the course of their radiation therapy and chemotherapy. Five patients received radiation therapy without adequate pain relief prior to the ablation and augmentation procedure. Three patients underwent ablation during their chemotherapy treatment. No concomitant therapy data were available on 21 patients.
Pain score measurements
In 44 patients (90%) the VAS scores were available before and after the procedure. The mean VAS score before the procedure was 7.9±2.5 (range 2–10) and the mean VAS score after the procedure was 3.5±2.6 (range 0–10). The mean decrease in the VAS score from baseline (matched pairs) was 4.6±3.4 (95% CI 3.6 to 5.6, p<0.0001) (figure 1).
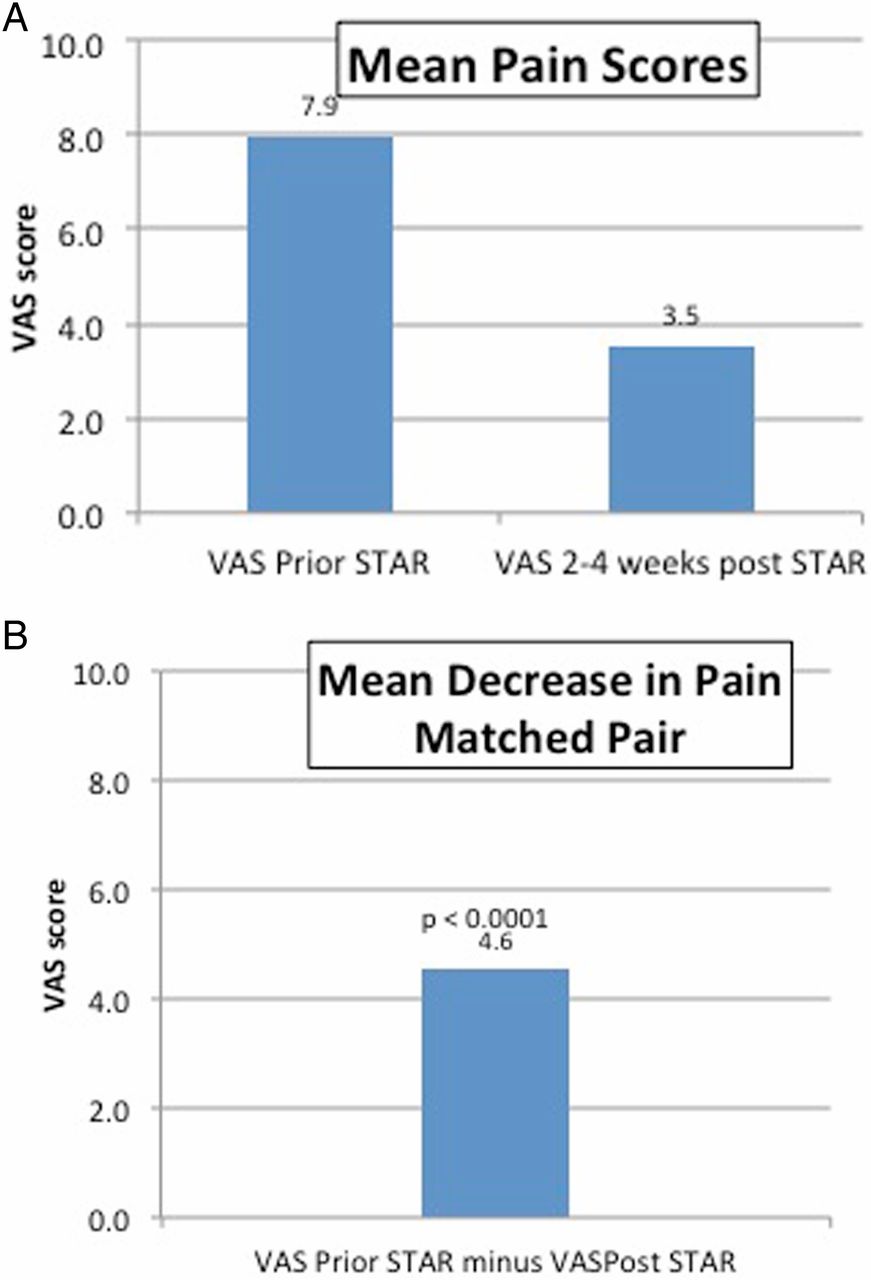
Mean decrease in Visual Analog Score (VAS) before and after STAR treatment (A) and the mean decrease in matched pairs (B).
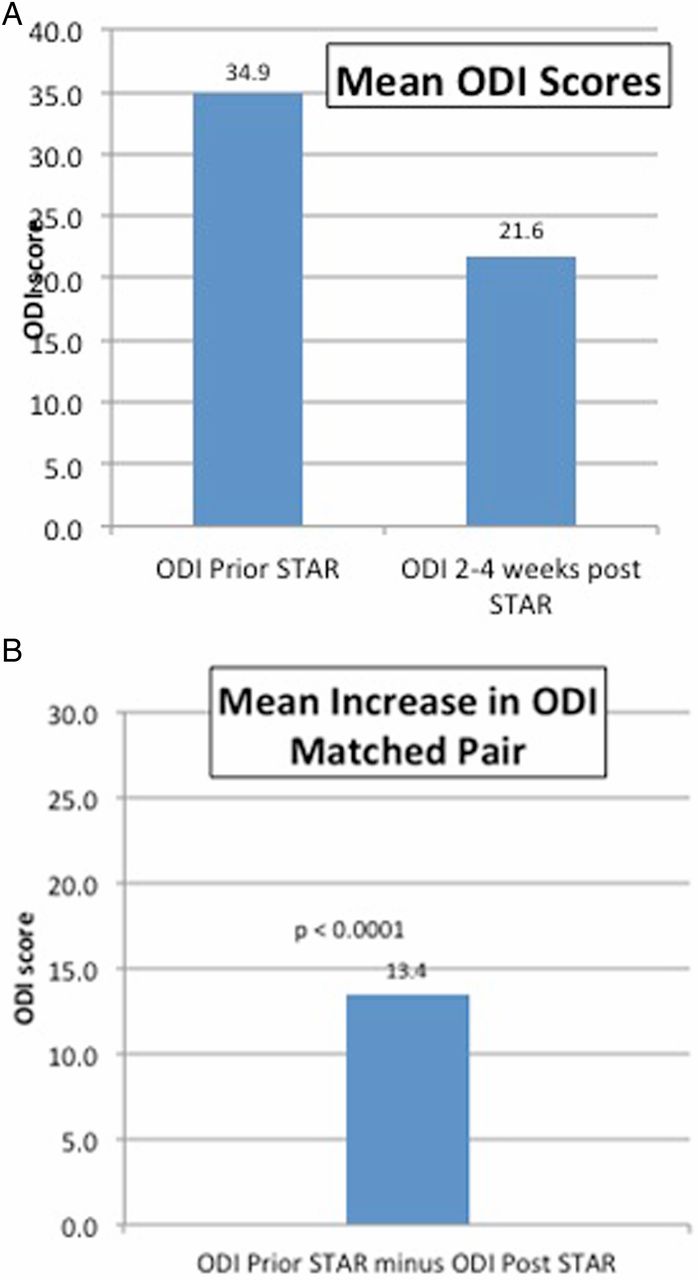
In 30 patients (63%) the ODI scores were available at pre- and post-procedure time points. The mean ODI score before the procedure was 34.9±18.3 (range 13–50) and the mean ODI score after the procedure was 21.6±13.8 (range 0–45). The mean ODI score decrease from baseline (matched pairs) was 13.4±8.1 (95% CI 10.4 to 16.4, p<0.0001) (figure 2).
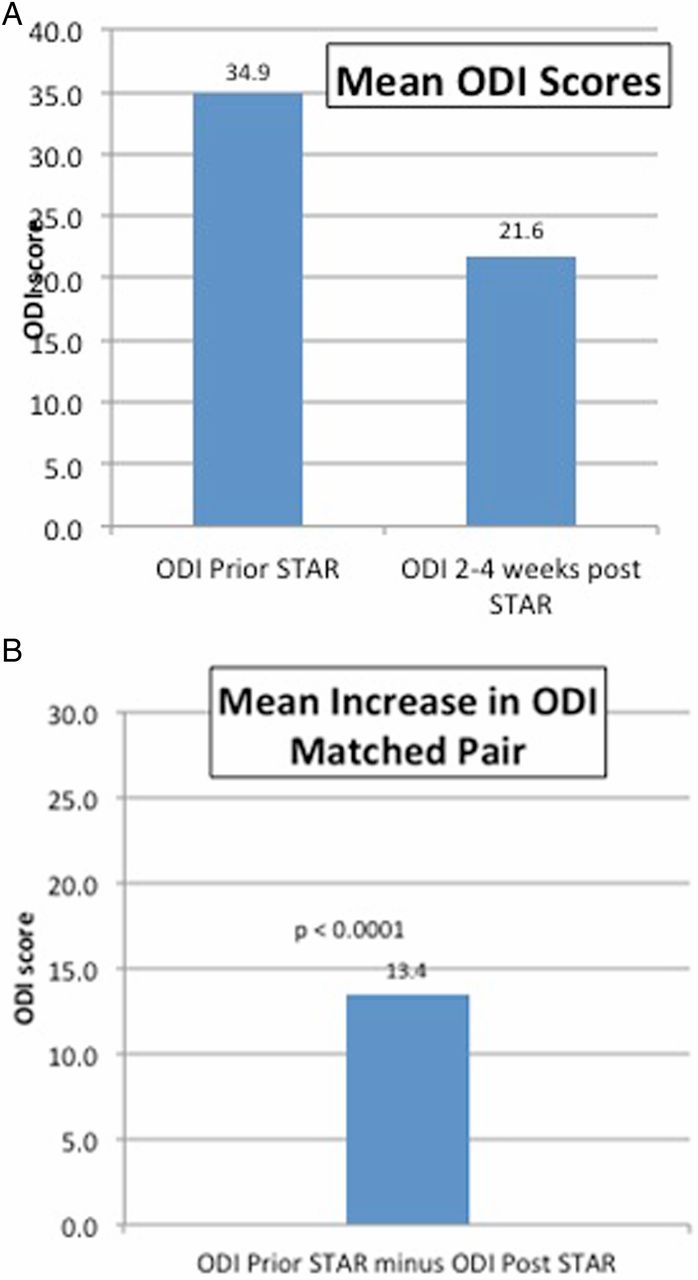
Mean decrease in Oswestry Disability Index (ODI) scores before and after STAR treatment (A) and the mean decrease in matched pairs (B).
Imaging evaluation
All but eight patients had some pre-procedure imaging. Fourteen patients had no post-procedure imaging. However, all those patients had clinical data available for VAS and/or ODI scores.
Pre-procedure CT was available in 40 (82%) patients. Evaluation of those with pre-procedure CT examinations showed 50 (69%) lytic lesions, 8 (11%) mixed lytic/sclerotic lesions, and 2 (2%) sclerotic lesions. Thirty-three of the 40 patients (83%) had lesions with posterior cortical disruption.
Twenty-four (49%) of the 49 patients had a post-procedure CT examination totaling 39 levels. Eight of these levels were documented to have posterior cortical disruption. No epidural cement leakages were seen in cases with cortical disruption. None of the patients demonstrated adverse cement-related clinical symptoms or sequelae.
Pre-procedure MRI showed variable degrees of vertebral body compression up to 80% involvement of the vertebral body. Images were evaluated by independent radiologists for T1- and T2-weighted signal characteristics, size and location of the lesion, presence of epidural or paravertebral extension, and degree of compression. The imaging pattern of a pathologic vertebra was hypointense or isointense on T1-weighted images and hyperintense on T2-weighted images. Eight levels had epidural extension and two levels had paravertebral components. Nineteen patients had compression fractures ranging from 20% to 80% based on pre-procedure MRI. Pre- and post-ablation MRI images were available in 15 patients with 21 lesions (figure 3). Post-procedure MRI showed decreased signal intensity on both T1- and T2-weighted images due to the presence of acrylic bone cement. Pre- and post-contrast fat saturated T1-weighted images were available for evaluation in 10 patients (with 16 lesions) following the ablation procedure. All of these lesions showed decreased tumor bulk on post-contrast enhanced images except in two patients. One patient with a breast cancer metastasis showed increased epidural extension after ablation. This patient showed marked unexpected progression of the disease and further biopsy confirmed development of a new malignancy (lymphoma). Another patient showed new extension of tumor into a neural foramen and associated epidural extension. All but one lesion showed a thin rim of contrast enhancement in the periphery of the tumor bed after ablation.
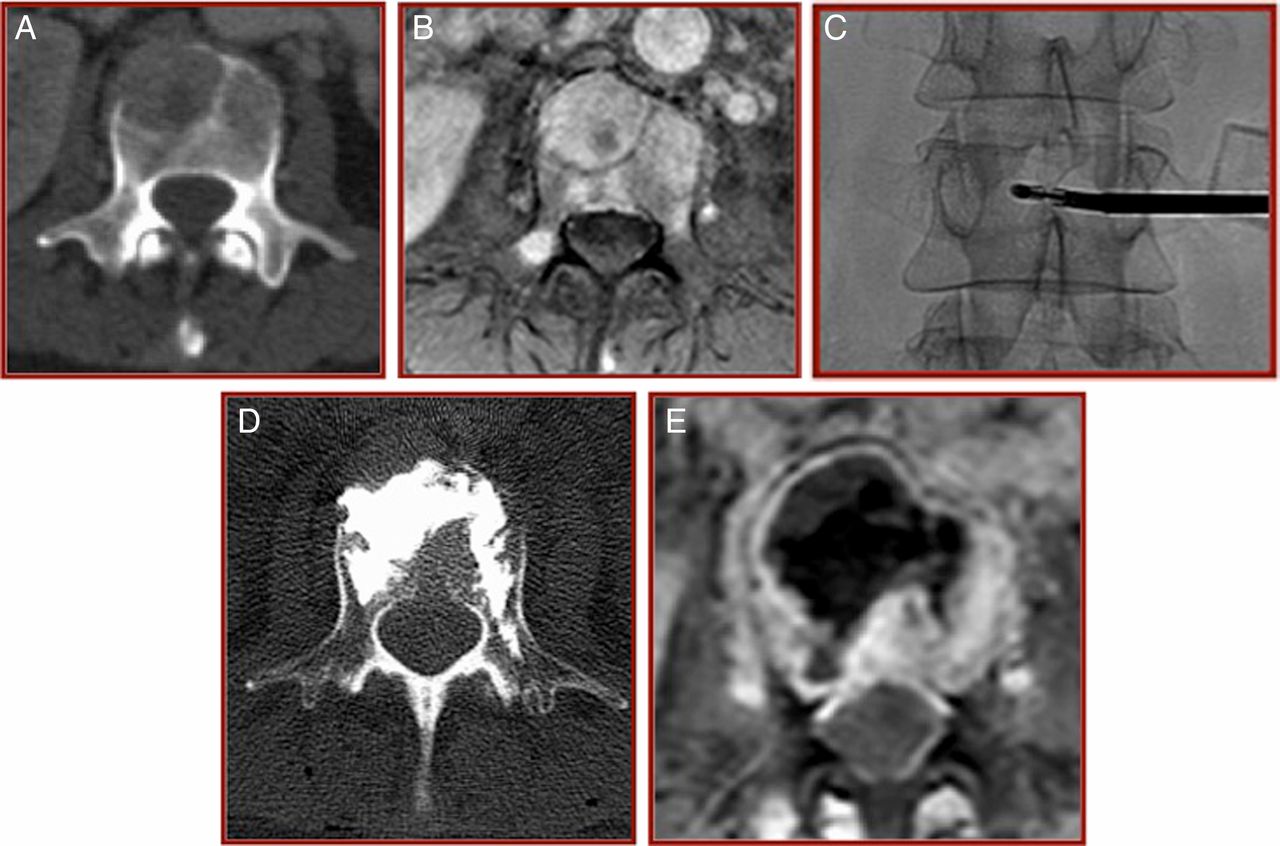
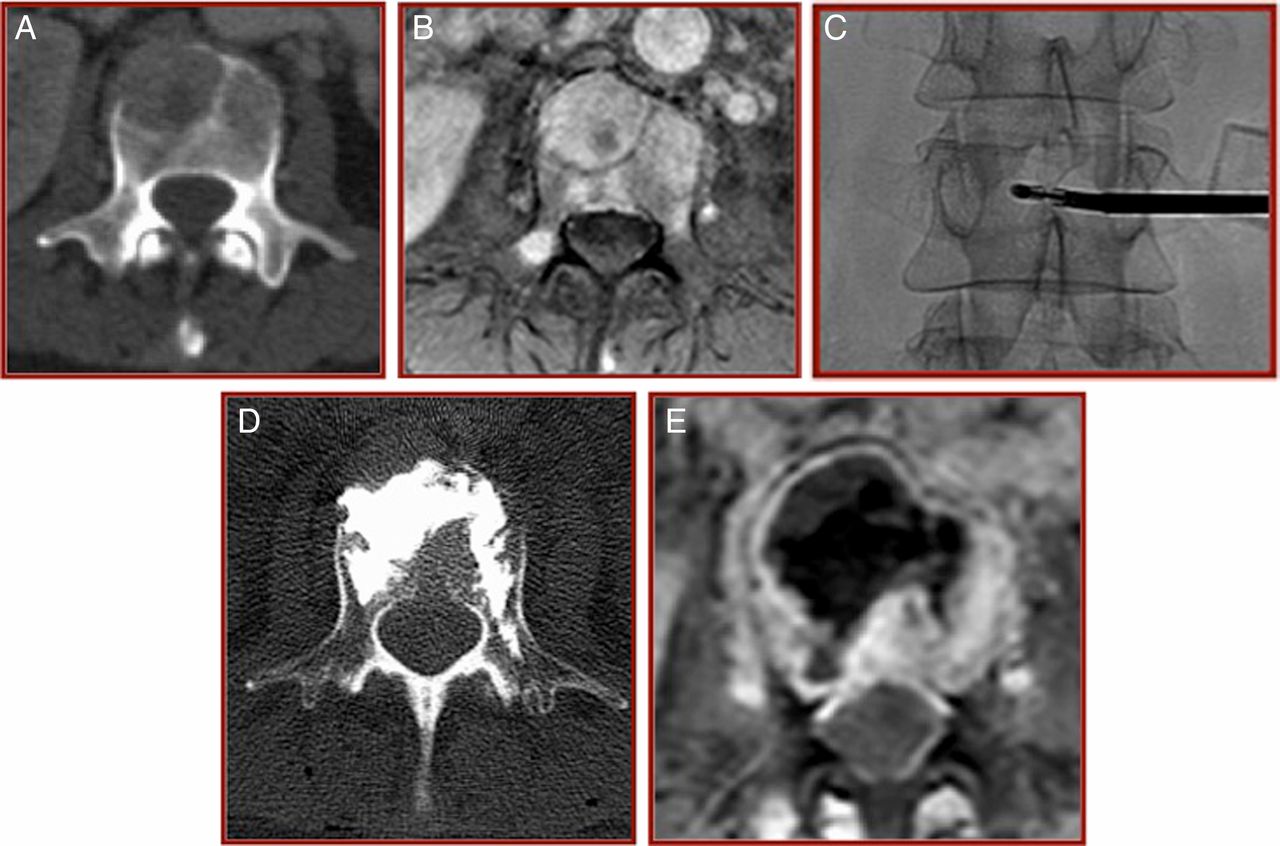
Middle-aged patient newly diagnosed with breast lump and back pain. (A, B) Axial images of the L2 vertebra showing a lytic lesion on CT examination (A) and corresponding enhancing tumor mass on contrast-enhanced T1-weighted fat suppression image (B). (C, D) The patient underwent a biopsy and radiofrequency ablation of the metastatic lesion followed by cement augmentation. (E) Post-procedure CT axial image showing almost uniform distribution of the cement. (F) Axial post-contrast T1-weighted images with fat suppression obtained after augmentation showing a decrease in the tumor bulk, a rim of reactive enhancement and cement low signal intensity.
Pre- and post-procedure PET scans were available for 10 patients (17 lesions; 22%). Ten lesions showed increased metabolic activity before ablation but no activity in the follow-up scan (figure 4). Seven lesions showed no activity on PET before ablation despite MRI indicating the presence of a metastatic lesion. One of those lesions showed recurrence of tumor and increased metabolic uptake in a neural foramen in post-procedure study.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
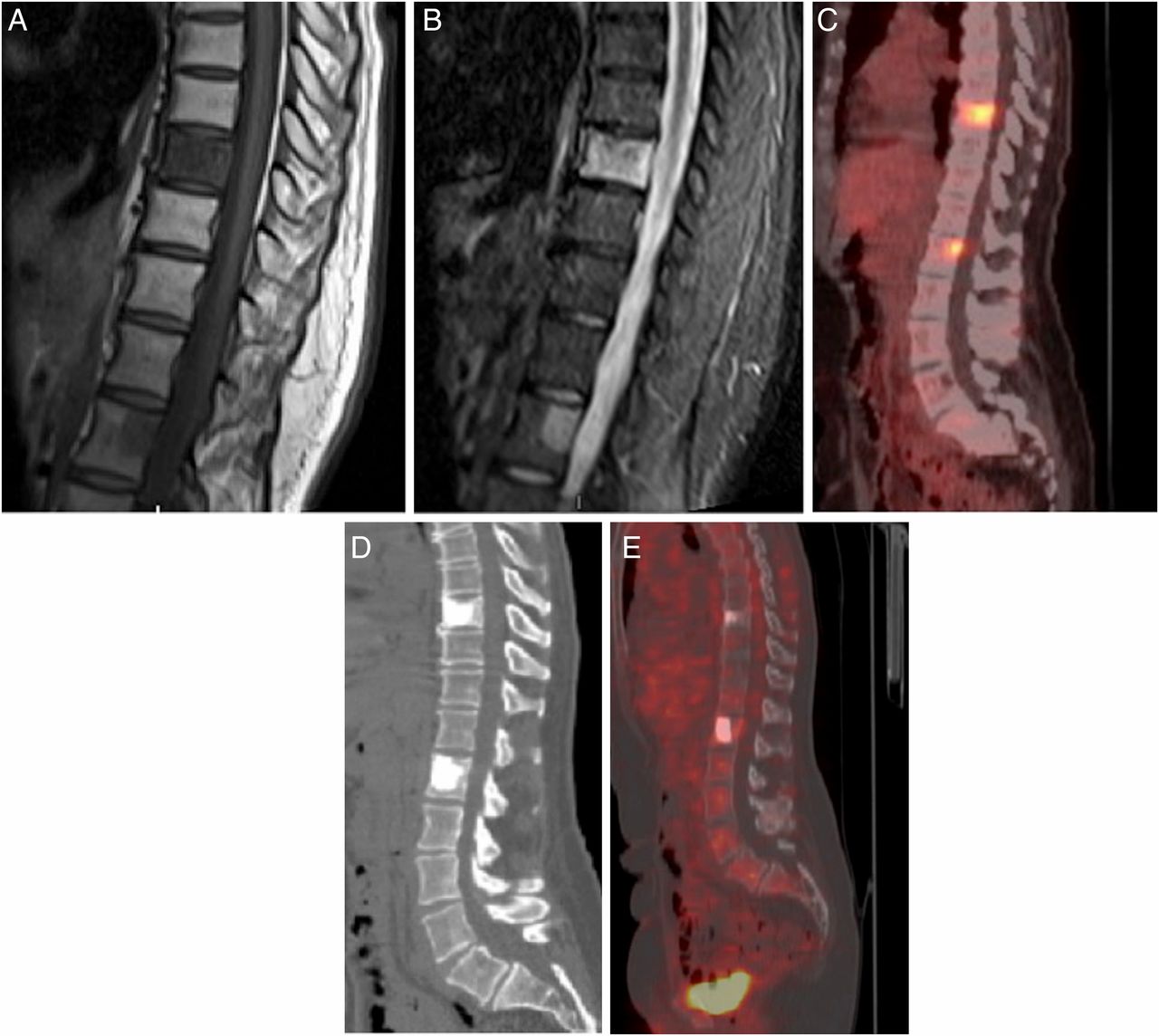
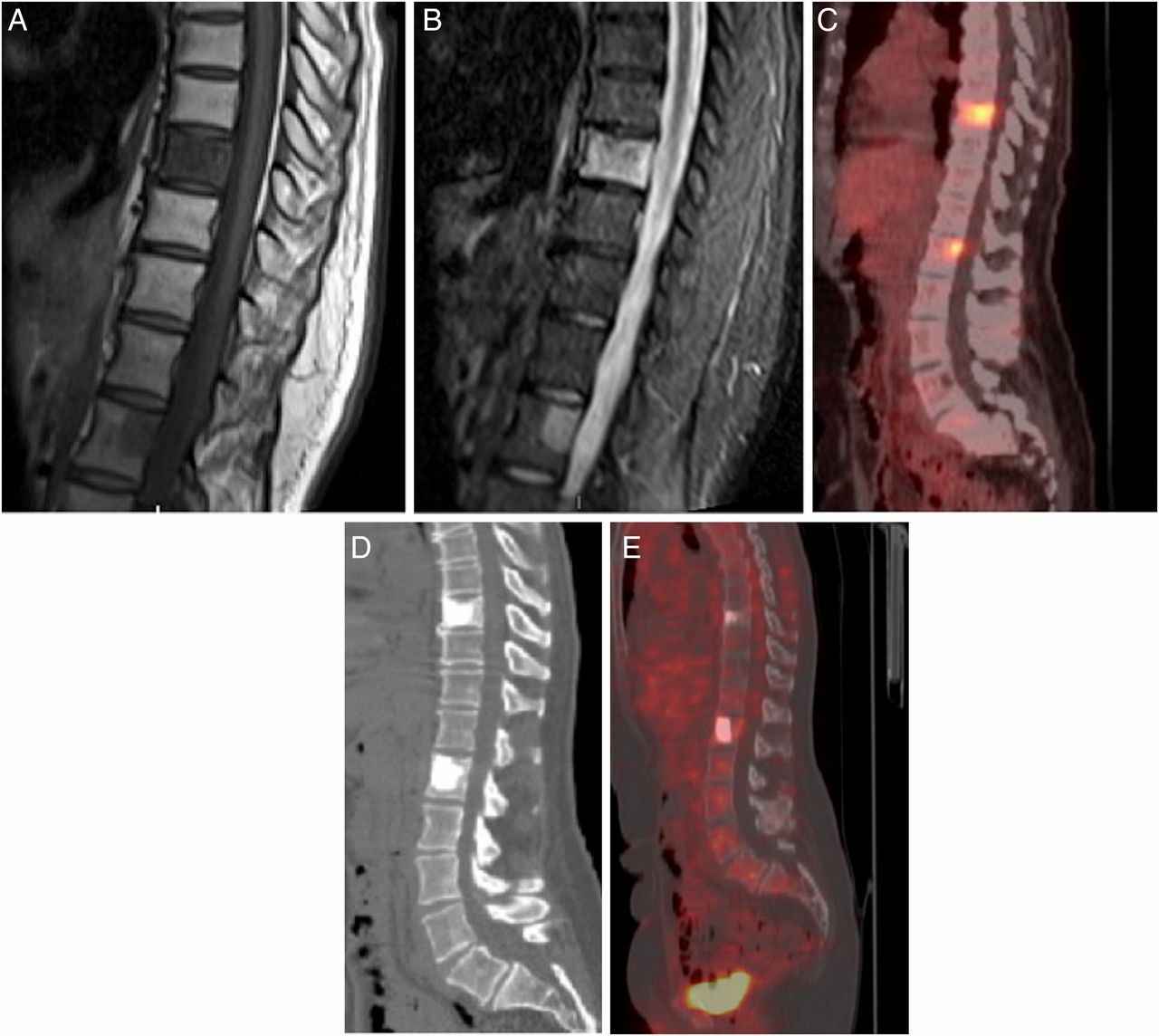
Elderly patient with a history of breast cancer and metastatic lesions at the T9 and L1 levels treated with chemotherapy. (A) T1-weighted and (B) STIR MRI images showing a diffuse abnormal signal involving the whole T9 vertebra and the posterior aspect of L1. (C) Sagittal reconstruction PET image showing increased metabolic activity at both levels. (D) Sagittal reconstruction CT image after radiofrequency ablation and cement augmentation showing uniform cement distribution with no leakage. (E) Sagittal reconstruction PET image taken 1 month after ablation showing no metabolic activity. The patient's Visual Analog Score and Oswestry Disability Index were 0 at that time.
Discussion
This study shows that t-RFA of spinal metastases followed by concurrent vertebral augmentation is safe and clinically feasible. t-RFA combined with vertebral augmentation results in a statistically significant reduction of pain as measured by the VAS and disability as measured by the ODI. Our imaging data are consistent with previously published reports in that contrast-enhanced MRI is potentially useful to document tumor debulking and can be used to assess post-ablation tumor mass burden. FDG PET scanning can also show decreased metabolic activity after RFA and can potentially be useful in assessing tumor activity after focal treatment.
RFA of metastatic bone tumors of the axial and peripheral skeleton has been described extensively in the literature. Reports of RFA alone or adjuvant to other treatment modalities has also been described.11 ,12 ,15 ,16 RFA can be performed safely for solitary metastatic bone lesions with a statistically significant increase in pain relief and a decrease in pain intensity 1 and 3 months following the procedure.12 These authors concluded that RFA could safely palliate pain from bone metastasis with no complications.12 These results are similar to previously published data where the authors showed that RFA of painful osteolytic metastases provides significant pain relief for cancer patients who have failed standard treatments.17 Another study using RFA alone with no cement augmentation to treat 39 spinal metastatic lesions showed significant pain relief and no reported complications.18 Treatment of bone metastases to the spine combining RFA and cementation has resulted in pain relief and minimal complications using commercially available RFA probes originally designed for other parts of the body.19 ,20 A previous retrospective study reported the safety and efficacy of the bipolar RFA device but did not use vertebral augmentation in all of the cases.15 These authors showed that this was a safe procedure and reported no complications. Efficacy was shown by a reduction in pain scores and analgesic use.15 In this study, the authors used the same articulating navigational device as it allowed unipedicular targeted access to the malignant lesions with continuous monitoring of the treated tissue temperature via multiple thermocouples embedded along the length of the electrode. This proved to be efficient compared with a report requiring multiple access sites for spine ablation using straight devices.21
According to the Metastatic Spine Disease Multidisciplinary Working Group algorithm, ablation is a reasonable therapeutic option for radio-resistant spine tumors, patients with persistent and/or recurrent pain who have reached their maximum radiation dose and where radiation therapy cannot be offered due to concomitant chemotherapy or is ineffective, given the low risk and potential for local tumor control.22
A recently published series of posteriorly located metastatic lesions of the spine treated by the navigational STAR RFA probe before cement augmentation showed no significant complications.23 Restoration of intact vertebral stability is possible in metastatic vertebrae after 30% tumor ablation and the injection of 1–2 mL bone cement.24 A protocol was developed by these authors on the basis of the findings of this study, recommending that the cement volume for injection be a function of the ablated tumor volume after ablation.24 Our data confirm and support the results of these studies.15 ,23 ,24
Adding RFA to conventional radiation therapy might improve the rate and degree of pain relief in the treatment of solitary bone metastasis.16 These results were corroborated in a small series of 21 patients which showed that percutaneous ablation and cement augmentation with concurrent radiation therapy is effective in palliating painful spinal metastases and controlling local tumor progression and can be effective in those patients who have radiation-resistant tumor histology.25 With respect to imaging, one study correlated pain relief with imaging features after RFA in solitary bone lesions but not specifically in the spine.26 These authors hypothesized that RFA denaturation of cytokines and destruction of cytokine-producing tumor cells is a component of RFA analgesia. Predictors of palliative RF pain relief were found to be the presence of existing pathological fractures and smaller tumor size, with a recommendation of targeting RF electrode placement to maximize ablation of the bone–tumor interface.
Decreased tumor mass inside the vertebral body before cement augmentation has an added value of limiting tumor embolization and spread around the vertebral body, which was described previously.13 ,14 The formation of a cavity inside the vertebra would decrease the chance of cement extravasation, particularly with compromised posterior cortex.8 We encountered only one case of increased epidural tumor in our data. This could be due to the short follow-up period or the debulking of the tumor tissue. Tumor necrosis has also been described due to the heat generated from cement augmentation.27 This area needs further longer-term studies.
To our knowledge, only one previous report has addressed the imaging findings in post-RFA lesions in the spine.28 It describes contrast-enhanced MRI as the modality of choice for assessing ablation therapy by correlating the volume of the non-enhancing ablation cavity with tumor volume on pretreatment images. Use of PET/CT is recommended to help differentiate FDG-avid tumor from granulation tissue or vascular fibrosis, which may confound post-treatment MRI assessment. In our series, post-ablation contrast-enhanced MRI consistently demonstrated a decrease in tumor bulk after ablation. Given the uniform consistent pattern of a thin enhancing rim, it was unlikely to represent residual tumor tissue but rather granulation tissue evolving into vascular fibrosis.28 No case showed a nodular or irregular enhancing rim to suggest residual or recurrent tumor. Based on these limited data, we believe that post-contrast fat saturated T1-weighed images are very suitable for following up patients after ablation procedures and pre-procedure contrast-enhanced images are required for comparison. However, interpretation of the MRI data should be considered in a setting where cement injection into the tumor bed could significantly impair the ability to assess the true volume of residual tumor.
FDG PET imaging, which was performed in a small number of patients in our series, showed either decreased or absent uptake and metabolic activity in all lesions. These data are consistent with a previous report that this imaging technique can also be useful in monitoring tumor recurrence after ablation.28
The limitations of this study include the fact that it is retrospective and limited in the length of follow-up. Long-term studies in stage IV cancer patient populations are extremely difficult as the status of the disease progression or regression coupled with other treatment modalities can interfere with the pain scale measurements and imaging findings. The multicenter nature adds to the value and validity of the results, especially given that there have been few studies in this arena. This retrospective evaluation should provide information for future controlled prospective studies. The concurrent treatment of part of our patient population with radiation therapy and chemotherapy may affect the accuracy of pain relief measurements; however, the relatively short follow-up (2–4 weeks) and the significant and rapid impact of ablation and augmentation suggest that the results are principally due to these interventional procedures. Other limitations of the study include operator-assessed outcomes, heterogeneity of the types of tumors treated, and the absence of standard pre- and post-treatment data collection and outcome algorithms.
None of the patients in our study who had cortical disruption showed epidural leakage following cement augmentation. This may argue for the role of RFA in decreasing the rate of cement leakage after augmentation due to a reduction in tumor bulk and hence a decrease in the intravertebral body pressure during cement injection.21
Conclusion
This study shows that t-RFA of spinal metastases using a navigational device followed by concurrent vertebral augmentation is safe and clinically feasible. No procedure-related complications were encountered in this series of patients treated at multiple different centers. Additionally, no clinically significant cases of cement extravasation, including epidural cement leakage, were observed in this group of patients.
References
Footnotes
Correction notice Since this paper was first published online data has been updated for accuracy. Data in the pain score management paragraph has also been updated.
Contributors All authors have made substantial contributions to the conception or design of the work and the acquisition, analysis, and interpretation of data for the work. All authors helped in drafting the work and revising it critically. All authors worked on the final approval of the submitted version and all authors agree on all aspects of the work to ensure accuracy and integrity of the work.
Competing interests BAG is a speaker and consultant for Merit Medical.
Ethics approval Ethics approval was obtained from Paloar Health Investigational Review Committee, Escondido, California, USA.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Any additional unpublished data such as unprocessed data, protocols, or images are available from the authors.