Article Text

Abstract
Background Spinal aneurysms are rare among spinal arteriovenous malformations (SAVMs). There are few reports of endovascular management of spinal aneurysms associated with SAVM.
Objective To present endovascular management of aneurysms associated with SAVM.
Methods Of 91 patients with SAVMs,eight (9%) presented with aneurysms. Of these, three were male and five were female with a median age of 18 years (range 11–38). We evaluated the presenting pattern, lesion level, type of the target aneurysm related to the presenting pattern and AVM nidus, and the result obtained after embolization or open surgery. Clinical status was evaluated by Aminoff–Logue (ALS) gait and micturition scale scores.
Results The presenting patterns were subarachnoid hemorrhage (SAH, n=3) or mass effect caused by extrinsic (n=4) or intrinsic (n=1) cord compression. Aneurysms were located in four cervical, two thoracic, and two lumbar enlargement areas. There were two prenidal (arterial), three nidal, and three postnidal (venous) aneurysms. The mean diameter of the aneurysms was 9 mm (range 3–27). Glue embolization (n=6), open surgery (n=1), and combined surgery and embolization (n=1) was performed to obliterate the aneurysms. Obliteration of the target aneurysms resulted in improvement of symptoms and clinical stabilization of SAVMs in all patients during a mean of 55 months (range 7–228) of follow-up.
Conclusions Identification of a symptomatic aneurysm should be associated with clinical presentation pattern. Targeted obliteration of the aneurysm by embolization and/or surgery resulted in improvement of symptoms and stabilization of SAVM.
- spine
- arteriovenous Malformation
- aneurysm
- embolic
Statistics from Altmetric.com
Introduction
Clinical presentations of spinal cord arteriovenous malformation (AVMs) can involve either progressive myelopathy or acute hemorrhage (subarachnoid or intramedullary).1 Patients with nidus-type AVMs are younger at presentation and more often present with hemorrhage, with a higher proportion of hematomyelia than fistulous-type AVMs.2 Non-hemorrhagic acute neurological deficits may be present because of acute thrombosis of venous pouches with mass effect and disturbance of venous outflow. Fistulous AVMs have been reported to present more frequently with progressive myelopathy, whereas the nidus types have been associated with an increased risk of hemorrhage.3
Spinal aneurysms are very rare, unlike their cranial counterparts. Spinal aneurysms can be divided into two groups: those associated with AVMs and isolated aneurysms.4 Patients with aneurysms associated with AVMs are older and more likely to present with bleeding than those with isolated aneurysms.4
The hemorrhage risk of nidus-type AVMs before treatment has been shown to be 4%/year in unruptured AVMs and 10% for AVMs with previous hemorrhage.5 In that meta-analysis, it was stated that the hemorrhage rate decreased significantly even after partial obliteration.
Aneurysm was found in 29% of spinal glomus (type II) AVMs and 10% of spinal (type IV) arteriovenous fistulae, and was associated with increased hemorrhagic risk in spinal (type II) AVMs.3 5 About 8% (9 out of 112) of aneurysms underwent spontaneous regression.4 None of them had an associated AVM; all had presented with hemorrhage. Only two lesions in this group were pseudoaneurysms; the other seven were true aneurysms.
There have been few reports on spinal aneurysm related to clinical presenting pattern in spinal arteriovenous malformation (SAVM) as a pathophysiology of SAVM.6 We present our experience of the diagnosis and treatment of patients with SAVM who presented with hemorrhage, myelopathy or compression symptoms caused by a mass effect related to spinal aneurysms.
Materials and methods
We reviewed the presence of spinal aneurysms in 91 patients with SAVM treated at our institution between May 1997 and October 2014.7 This study was approved by our institutional review board. Informed consent was obtained from each patient or their relatives during diagnostic and therapeutic procedures.
MRI acquisition (1.5 or 3T) varied among included patients, with sequences of T1- and T2-weighted axial and sagittal images, as well as T1-weighted images with and without contrast enhancement. Selective single or biplane and rotational angiographies of the feeding segmental arteries were performed. We used information from 3D rotational angiography, showing the association between aneurysm size and localization and clinical presentation, to determine whether the aneurysm was the cause of presenting symptoms or signs.8
We included patients who had spinal aneurysm associated with SAVM and excluded patients with dural arteriovenous fistula at the craniovertebral junction level of C1 or with inadequate image quality, even though the lesion was diagnosed as having aneurysm at the operation.
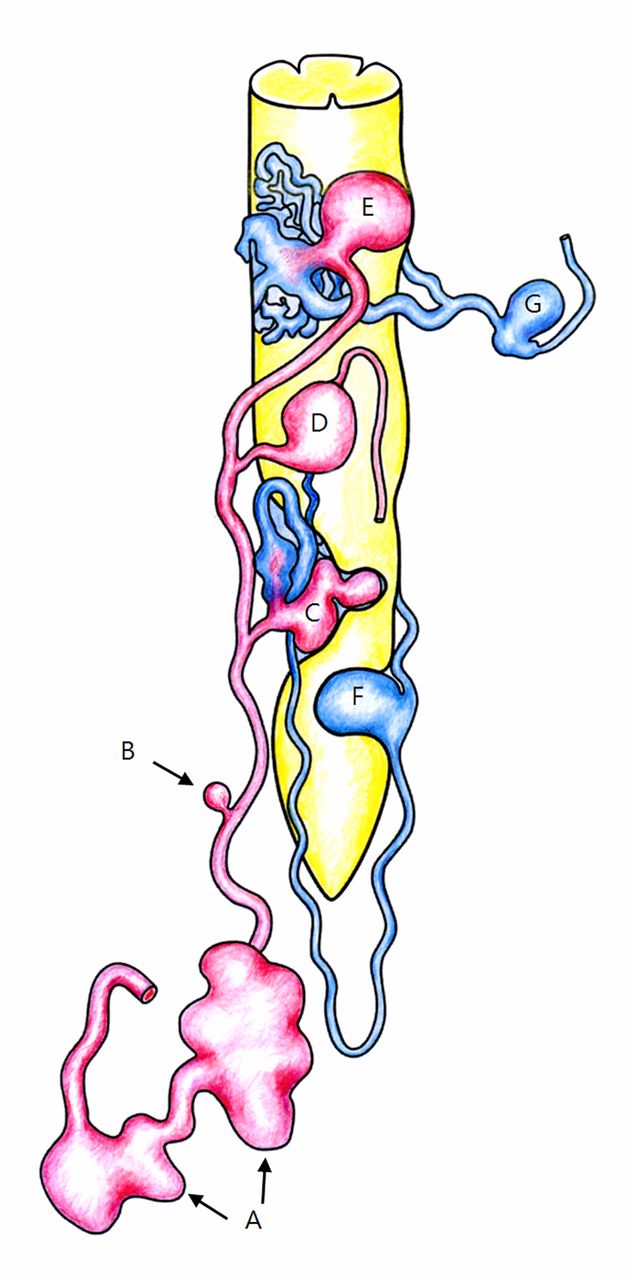
We defined three types of aneurysms related to the SAVM nidus: prenidal (arterial),9 nidal, and postnidal (venous), because spinal aneurysm has not been clearly defined in the literature (figure 1). Prenidal aneurysm was identified on 2D and 3D rotational angiograms by a morphological change of the lumen diameter at least more than twice that of the adjacent normal looking vessels. Nidal aneurysm was defined by abnormally dilated pouch at the nidus on an angiogram and/or on MR images, corresponding to the hemorrhagic focus or symptom presentation. Postnidal aneurysm was a dilated pouch, identified at the venous side, which showed stasis of the contrast agent and was regarded as having an angiographic feature of a pseudoaneurysm.10

Schematic diagram of the spinal aneurysms associated with spinal arteriovenous malformation. (A) Prenidal aneurysm with radiculopathy due to mass effect to nerve root (n=1), (B) prenidal aneurysm associated with subarachnoid hemorrhage (n=1), (C) nidal aneurysm with intrinsic compression of the spinal cord (n=1), (D) prenidal aneurysm with extrinsic compression of the spinal cord (n=1), (E) nidal aneurysm associated with subarachnoid hemorrhage (n=1), (F) postnidal aneurysm with mass effect (n=2), and (G) postnidal aneurysm with subarachnoid hemorrhage (n=1).
The target aneurysm was correlated with the clinical presenting pattern—that is, hemorrhage or mass effect caused by spinal cord or root compression. In addition, the presence and contribution of symptoms and signs were further confirmed by the immediate improvement of symptoms after treatment and subsequent continuous improvement or stability of clinical status during the follow-up period.11 12 To examine the mass effect of an aneurysm related to compression of the spinal cord or nerve root, we correlated a patient’s symptoms or neurological deficit with the aneurysm on angiography and MRI to confirm that mass effect of the aneurysm was the cause of the presenting symptoms and signs.
We chose the mode of treatment after considering surgical and endovascular treatment options. Various microcatheters and wires were used in each patient for endovascular treatment. The first-line system included Excelsior 10 (Boston Scientific, Natick, Massachusetts, USA), Marathon (Covidien, Irvine, California, USA), Excelsior 1018 (Boston Scientific), Prowler 10–45 (Cordis, Miami, Florida, USA), and Apollo 1.5Fr (Covidien) for the microcatheter; and Mirage 008 (Medtronic, Dublin, Ireland), TRAXCESS 14 (Microvention, Tustin, California, USA), and Synchro 14 (Target, Boston Scientific, West Valley City, Utah, USA) for the microguidewire. Improvement of neurological status was evaluated using the Aminoff–Logue disability scale before treatment and during follow-up. The mean clinical follow-up period was 55 months (range 7–228).
Results
Among 91 patients with SAVM, eight (9%) had spinal aneurysms. There was no isolated aneurysm in our study. The clinical and radiologic findings of the eight patients are summarised in table 1. Patients were three men and five women with a median age of 18 years (range 11–38). Aneurysms were located in four cervical, two thoracic, and two lumbar enlargement areas. There were two prenidal (figure 2),9 four nidal (figures 3–5), and two postnidal (figure 6) aneurysms. The mean diameter of the aneurysms was 9 mm (range 3–27). Clinical presentation included severe headache caused by subarachnoid hemorrhage (SAH) (n=3) (figure 3 and 6) or mass effect (n=5). The mass effect of an aneurysm was regarded as being extrinsic (n=4, figure 2 and 4) or intrinsic (n=1, figure 5) compression and corresponded to recent aggravation of symptoms based on identified location on angiography and MRI even though spinal cord oedema (myelopathy) associated with venous congestion was also found in four patients with an aneurysm (table 1).
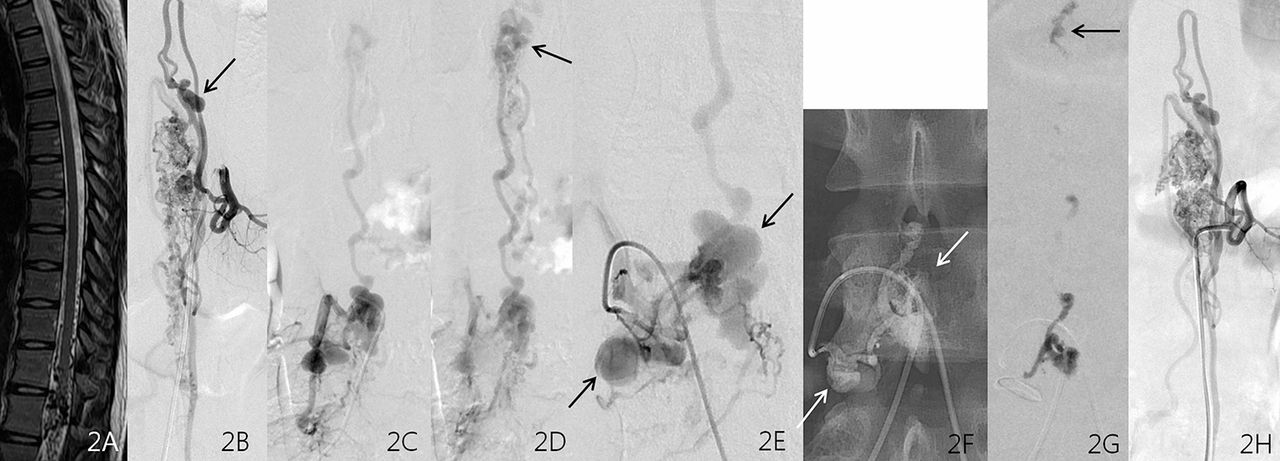
Prenidal aneurysm with extrinsic mass effect (patient 6). A 19-year-old girl presented with numbness in the right lower extremity with pain. (A) A sagittal T2-weighted image shows a spinal arteriovenous malformation (AVM) without significant cord oedema. (B) Selective angiogram of the left T12 segmental artery shows the radiculomedullary artery supplying the AVM. Note aneurysms (arrow) of the anterior spinal artery, which were not related to the patient’s symptoms. Anteroposterior arterial (C), venous (D), and oblique arterial (E) views of the right L3 lumbar arteriogram show large lobulated prenidal aneurysms (arrows in E), which are regarded as the cause of her symptoms due to the corresponding nerve root compression near the intervertebral foramen. Arrow in (D) indicates AVM nidus at the level of the conus medullaris. (F) Glue embolization (arrows) of the aneurysm and a part of the fistula at the level of conus results in marked improvement of her symptoms. (G) Part of the glue cast (arrow) reaches the fistula after obliteration of the aneurysms. (H) The left T12 segmental arteriogram after embolization shows no significant change of the flow from above.

Nidal aneurysm with subarachnoid hemorrhage (patient 5). A 17-year-old boy presented with sudden headache related to subarachnoid hemorrhage on CT scan (not shown). (A) Sagittal T2-weighted image shows a cervical spinal arteriovenous malformation (AVM) without significant cord oedema. (B) Selective angiogram of the right T3 segmental artery shows the radiculomedullary and radiculopial arteries supplying the AVM. (C) Selective angiogram shows a nidal aneurysm which was regarded as a source of hemorrhage. (D) Glue embolization (arrow) of the aneurysm results in marked improvement of her symptom and stable clinical condition during 34 months’ follow-up.
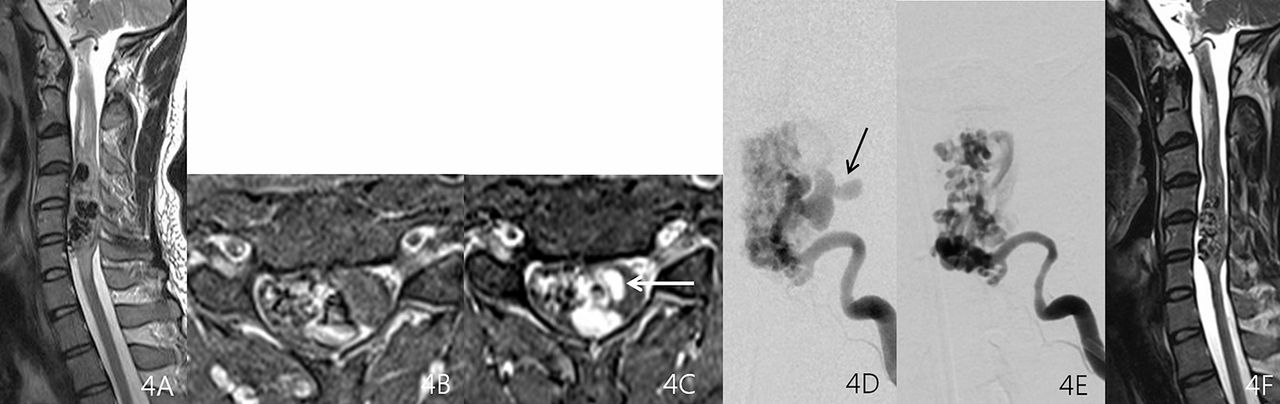
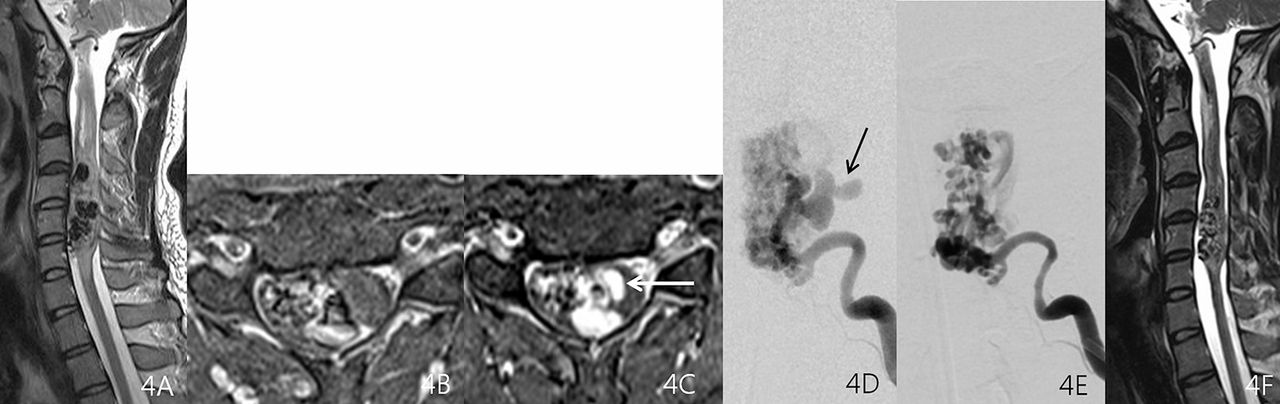
Nidal aneurysm with extrinsic mass effect (patient 2). A 29-year-old man presented with rapid progression of left hemiplegia. (A) Sagittal T2-weighted image shows a cervical spinal cord arteriovenous malformation (AVM) with multiple signal voids and cord oedema. Comparison with enhanced axial fat-suppression T1-weighted images at the same level taken initially (B) and 8 days later (C) shows development of a large aneurysm within the cervical spinal cord (arrow), which corresponds to recent aggravation of neurological status. (D) Left ascending cervical arteriogram shows that the anterior spinal artery fed an AVM nidus with a bird-beak-like aneurysm (arrow). (E) The aneurysm disappears after glue embolization of a portion of the nidus. (F) Sagittal T2-weighted imaging 3 months later shows decreased size of the nidus. Symptoms including motor deficits markedly improved after the procedure (modified Rankin score=1) and the patient was stable during 26 months of follow-up.

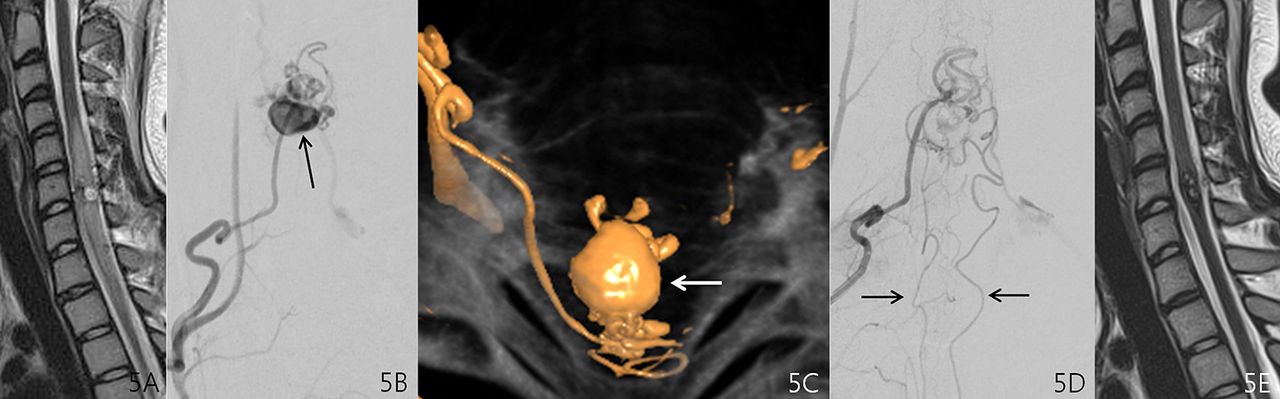
Nidal aneurysm with intrinsic mass effect (patient 3). A 17-year-old girl presented with numbness in the right arm and leg with pain. (A) Sagittal T2-weighted imaging shows a perimedullary arteriovenous fistula with cervical cord oedema. (B) Selective angiogram of the costocervical trunk shows the radiculopial artery supplying the arteriovenous malformation (AVM) and aneurysm (arrow). (C) Three-dimensional angiogram shows anteriorly located aneurysm (arrow) within the spinal cord, which is supplied by the posteriorly located radiculopial artery. (D) Image after glue embolization shows aneurysm disappearance with filling of the paired pial axis downward (arrows). (E) T2-weighted imaging 14 months later shows decreased size of the spinal cord AVM and disappearance of cord oedema. Her symptoms disappeared during 15 months of follow-up.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
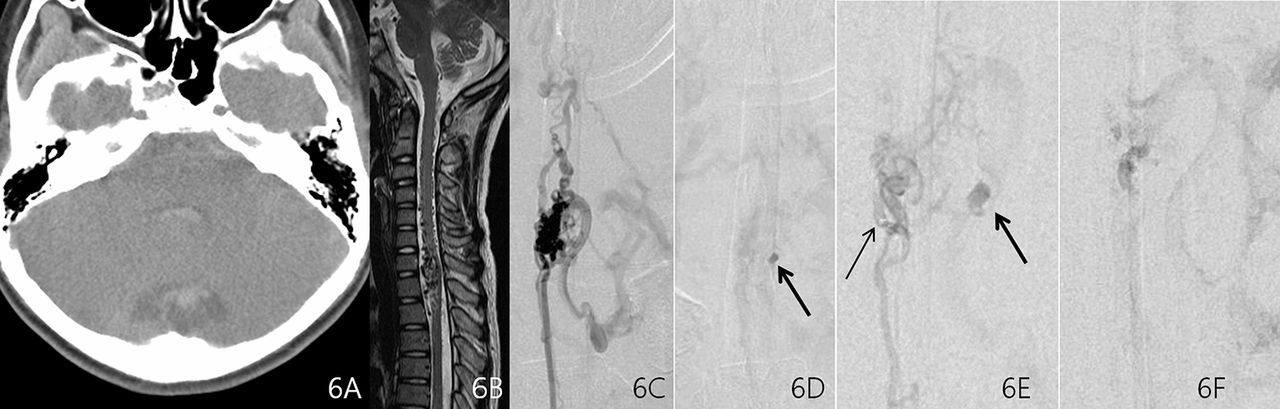
Postnidal aneurysm with subarachnoid hemorrhage (SAH) (patient 4). An 11-year-old boy presented with severe headache caused by SAH on brain CT (A). Cerebral angiography revealed no intracranial abnormality (not shown). (B) Sagittal T2-weighted imaging shows a spinal cord arteriovenous malformation (AVM). (C) The anterior spinal artery arising at left T7 fills the lower part of the spinal cord AVM. (D) Note delayed stasis of the contrast agent in a small pseudoaneurysm (arrow), which was considered to be the focus of the hemorrhage. (E) Selective angiography at a sulcocommissural artery (thin arrow) of the anterior spinal artery shows the magnified aneurysm (thick arrow). (F) Glue embolization of the part of the nidus connected to the hemorrhagic focus eliminated further filling of the pseudoaneurysm and immediately ameliorated severe headache. The patient remained stable for 68 months of follow-up.
Summary of patients with aneurysms associated with spinal arteriovenous malformation
Glue embolization was performed in six patients to obliterate the target aneurysms and stabilize the anatomical weak points or reduce the mass effect that corresponded to the patient’s neurologic deficit. Of two patients who had surgery, one underwent intraoperative targeted glue embolization.13 We used n-butyl cyanoacrylate in all cases because it is easy to control, the injection time is relatively short, and it has better visibility than Onyx.11 The use of Onyx for dural SAVM embolization has been limited by difficulty achieving venous penetration. Obliteration of the target aneurysm resulted in immediate improvement of headache after embolization of a sulcocommissural artery of the anterior spinal artery by using preferential flow to a postnidal (venous) aneurysm in a patient who presented with SAH; this was regarded as an indirect sign of successful obliteration of the aneurysm (figure 6). Obliteration of the target aneurysm which corresponded to the patient’s presenting symptoms was confirmed by postprocedural angiography, which showed improvement of symptoms in all patients. Neurological status before and after treatment are shown in table 1.
Representative case series
Case 1 (patient 2). A 29-year-old man was referred to the emergency room of our institution because of sudden right hemiplegia. He was healthy before developing the neurological deficit, which progressed over several days. MRI performed at another hospital revealed cervical cord oedema and markedly dilated vessels around the spinal cord (figure 4A). The spinal cord was progressively compressed by a dilated vascular aneurysm pouch at the level of C5 (figure 4B and C). Cervical angiography showed a lobulated aneurysm at the markedly dilated anterior spinal artery (ASA) arising from the left ascending cervical artery (figure 4D). The AVM drained into the anterior spinal vein. We used a transfemoral approach to place a 5 F catheter into the left ascending cervical artery and a microcatheter was coaxially introduced through the catheter into the aneurysm through the ASA. Advancement of the microcatheter into the aneurysm through the neck was difficult, probably owing to an eccentrically narrowed aneurysm neck, even though the aneurysm neck looked wide on the angiogram. The large and lobulated aneurysm located on the left side of the AVM nidus in the spinal canal was connected to rapid fistula flow and was considered to be an aneurysm of the feeder that displaced and compressed the spinal cord to the right side, leading to rapid development of right hemiplegia. Glue embolization of the multiple feeders of the ASA, including the aneurysm connected to the fistula, was performed. A final angiogram revealed no further filling of the aneurysm and reduction of the fistula flow, although there was a residual AVM (figure 4E). The neurological deficit was much improved after the procedure. Three-month follow-up MRI showed markedly improved cord oedema and decreased size of the flow voids in the cervical spinal cord (figure 4F). Further embolization was not done because his neurological status was stable.
Case 2 (patient 3). A 17-year-old girl presented with progressive neurological deficits of sensory changes and mild motor weakness in both lower extremities. MRI performed at another hospital revealed cervical cord oedema and round dilated signal voids within the swollen spinal cord (figure 5A). Cervical angiography disclosed an aneurysm at the posterior spinal artery arising from the right ascending cervical artery (figure 5B and C). Microcatheter selection of the feeder was possible with a stably engaged 4 F catheter using a brachial approach; 4 F catheter positioning using a transfemoral approach was not stable at the origin of the ascending cervical artery. Glue embolization was performed at the posterior spinal artery, including the aneurysm connected to the fistula. A final angiogram revealed no further filling of the aneurysm and reduction of the fistula flow (figure 5D). MRI carried out 14 months later showed improvement of the cord oedema and decreased size of the signal voids in the cord (figure 5E). The neurological deficit improved after the procedure and her clinical status was stable during 15 months of follow-up.
Case 3 (patient 4). An 11-year-old boy was referred to the emergency room of our institution owing to sudden severe headache with neck stiffness. Brain CT angiography showed SAH, but there was no other parenchymal lesion or intracranial aneurysm (figure 6A). He was healthy until he developed the SAH. MRI performed at another hospital revealed cervical cord oedema and markedly dilated vessels around the spinal cord (figure 6B). Left T7 segmental angiogram showed a juvenile type of AVM at the cervical spinal cord supplied by the anterior spinal artery (figure 6C). There was a dilated venous pouch with delayed stasis of the contrast agent, which was regarded as a pseudoaneurysm (postnidal aneurysm) of the draining vein (figure 6D and E). Advancement of the microcatheter into the aneurysm was not possible because the aneurysm was located on the postnidal venous side. However, the aneurysm was filled by a preferential flow when the microcatheter reached a certain point of the sulcocommissural artery, where a small amount of glue was introduced to obliterate flow into the aneurysm.
Even though there was no evident glue filling of the aneurysm on fluoroscopy, the pseudoaneurysm did not fill after embolization. Further embolization was deferred because the main feeders were from the ASA. Immediate amelioration of his severe headache after the procedure was regarded as an indirect sign of successful obliteration of the symptomatic postnidal venous pseudoaneurysm, which no longer filled after embolization. He was stable during 5 years of follow-up.
Discussion
A spinal aneurysm was identified in 9% of SAVM cases in our series. The incidence of aneurysms could not be compared with other studies because only case reports or series including 1–4 cases have been published. A systematic review on spinal aneurysms showed that 55 (44.7%) were associated with an AVM and 68 (55.3%) were isolated spinal aneurysms not associated with an AVM; thus, isolated aneurysms are more commonly associated with SAVM.4 However, we did not observe any isolated spinal aneurysms in our study or any aneurysm associated with an epidural arteriovenous fistula, which is known to cause congestive venous myelopathy.14–17
Our results showed three locations for aneurysms from a nidus or fistula: one prenidal (arterial), five nidal, and one postnidal (venous). The location was not closely related to the presenting symptoms. Of three aneurysms with SAH, one was prenidal, one nidal, and one postnidal (venous). Aneurysm size was also variable, without any relationship to the presenting symptom pattern. In our cases, 63% (5/8) of the patients presented with mass effect without hemorrhage. Congestive venous myelopathy may be the cause of the symptom.18–20 However, congestive venous myelopathy is characterised by progressiveness or exertional aggravation without rapid deterioration as in our patients.6 Therefore, mass effect caused by an aneurysm needs to be correlated with symptoms and recent aggravation of neurological deficit. However, we cannot completely exclude any other possible combination of symptomatic presentations in patients with spinal aneurysm associated with SAVM.
In the study of Madhugiri et al, in which 20.8% of the spinal aneurysms were associated with SAVM and 7.8% with isolated spinal aneurysms, patients presented with complaints not attributable to bleeding from the lesion.4 Therefore, our study showed that hemorrhage of a spinal aneurysm was less common than reported in the literature. Aneurysms in our study were relatively common (4/8) in cervical cord areas, as found in a systemic review.4 Although we did not use surgical decompression to relieve the mass effect, there are several reports on surgical decompression or clipping of the feeding artery ligation.21 22
Our study has several limitations. First, it included a limited number of patients with symptomatic aneurysms, even though the aneurysms were regarded as the cause of the recent aggravation of the corresponding neurological deficit. Second, it was difficult to explain the common occurrence of mass effect without hemorrhage in our study. Mass effect without rupture of the growing aneurysm needs to be clarified.
In conclusion, we describe eight patients (9%) with an aneurysm among 91 cases of SAVM. Glue embolization and/or surgery could obliterate aneurysms and stabilize anatomical weak points or reduce mass effects. Obliteration of the target aneurysm resulted in immediate improvement of a patient’s symptoms and clinically stabilized the SAVM during follow-up.
Acknowledgments
We acknowledge the assistance of Eunja Yoon and Danbi Park.
References
Footnotes
Contributors SCJ: main idea development, manuscript writing; YS: manuscript preparation, data collection, literature review, manuscript revision; JK: literature review; SHC: data analysis, literature review; SYN: data collection, literature review; SHL, JJS: literature review; SCR, SRJ: study development, DCS: main idea development, manuscript writing and editing, study development.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Institutional review board of the Asan Medical Center.
Provenance and peer review Not commissioned; externally peer reviewed.