Article Text

Abstract
Objective To evaluate direct transfer to the angiosuite protocol of patients with acute stroke, candidates for endovascular treatment (EVT).
Methods We studied workflow metrics of all patients with stroke who had undergone EVT in the past 12 months. Patients followed three protocols: direct transfer to emergency room (DTER), CT room (DTCT) or angiosuite (DTAS, only last 6 months if admission National Institute of Health Stroke Scale (NIHSS) score >9 and time from onset <4.5 hours) according to staff/suite availability. DTAS patients underwent cone-beam CT before femoral puncture. Dramatic clinical improvement was defined as 10 NIHSS points drop at 24 hours.
Results 201 patients were included: 87 DTER (43.3%), 74 DTCT (36.8%), 40 DTAS (19.9%).
Ten DTAS patients (25%) did not receive EVT: 3 (7.5%) showed intracranial hemorrhage on cone-beam CT and 7 (17.5%) did not show an occlusion on angiography. Mean door-to-puncture (D2P) time was shorter in DTAS (17±8 min) than DTCT (60±29 min; p<0.01). D2P was longer in DTER (90±53 min) than in the other protocols (p<0.01). For outcome analyses only patients who received EVT were compared; no significant differences in baseline characteristics, including time from symptom-onset to admission, puncture-to-recanalization, or recanalization rate, were seen. However, time from symptom-to-puncture (DTAS: 197±72 min, DTER: 279±156, DTCT: 224±142 min; p=0.01) and symptom-to-recanalization (DTAS: 257±74, DTER: 355±158, DTCT: 279±146 min; p<0.01) were longer in the DTER group. At 24 hours, there were no differences in NIHSS score (p=0.81); however, the rate of dramatic clinical improvement was significantly higher in DTAS: 48.6% (DTER 24.1%, DTCT 27.4%); p=0.01). An adjusted model pointed to shorter onset-to-puncture time as an independent predictor of dramatic improvement (OR=1.23, 95% CI 1.13 to 133; p<0.01)
Conclusion In a subgroup of patients direct transfer and triage in the angiosuite seems feasible, safe, and achieves significant reduction in hospital workflow times.
- Stroke
- Thrombectomy
- Intervention
Statistics from Altmetric.com
Time from symptom onset to reperfusion has been repeatedly shown to be the most powerful predictor of outcome in patients with acute stroke.1 ,2 In the first 6–8 hours after symptom onset the chances of functional recovery without disability decrease 10–15% for each 30 min delay to reperfusion.3 In 2015 several clinical trials demonstrated the efficacy of reperfusion induced by endovascular treatment (EVT) to reduce disability in patients with acute ischemic stroke,4 emphasizing this important tenet in treatment of this disease.
As a result, the number of endovascular procedures for acute stroke is increasing exponentially around the world. Major efforts are being made to create EVT-capable centers and redefine prehospital circuits to ensure a timely arrival to as many appropriate centers as possible, with the ultimate goal a reduction of the time to reperfusion. Despite that in most cases the bulk of the workflow time corresponds to the prehospital setting; in-hospital circuits and protocols also need to be reassessed to minimize the time to recanalization.
Investigators from Helsinki have shown that with multiple concurrent strategies it is possible to reduce the median door-to-needle time for IV tissue plasminogen activator (tPA) treatment from 300 to 20 min.5 A recently published study showed that for patients undergoing endovascular procedures the door-to-puncture (D2P) time is an independent predictor of further good outcome.6
We aim to investigate the safety and feasibility of a new direct transfer to angiosuite (DTAS) protocol that will dramatically reduce the in-hospital workflow times.
Methods
We studied in-hospital workflow metrics of all admitted patients with acute stroke in our comprehensive stroke center who had undergone EVT between December 2015 and November 2016. In previous years, all patients with suspected acute stroke admitted to our institution followed one of two different admission protocols: (1) direct transfer to the emergency room (DTER) for initial clinical evaluation before a CT scan or (2) direct transfer to the CT room (DTCT) for simultaneous clinical evaluation/CT scan. The second option was favored but depended on preadmission notification by the emergency medical systems (Rapid Arterial oCclusion Evaluation (RACE) score >47) and stroke team/CT scan immediate availability. Starting June 2016, a third option was implemented: (3) DTAS: this option was considered and favored upon preadmission notification by the emergency medical systems (RACE score >4) and depending on stroke team/angiosuite immediate availability. Before entering the angiosuite a quick neurological assessment was performed by the stroke neurologist in charge in order to confirm an NIHSS score >10, as a predictor of large vessel occlusion (LVO), and time from symptom onset <4.5 hours. If the NIHSS score was <10 or time from onset >4.5 hours the patient was excluded from the DTAS option and followed the DTER or DTCT admission protocol.
DTER and DTCT patients were selected for EVT according to a standard CT protocol (Alberta Stroke Program Early CT Score (ASPECTS) ≥6) and confirmation of LVO on CT angiography. DTAS patients underwent cone-beam CT (Xpert-CT, high dose/fast acquisition, Allura Clarity FD 20/20 Philips 2015) in the angiosuite immediately before femoral artery puncture. Absence of intracranial hemorrhage and absence of large infarct signs were used as selection criteria for EVT treatment. Confirmation of LVO could not be performed in the DTAS group.
All patients received IV tPA, when indicated, after either conventional CT scan or Xpert-CT. Independently of the admission protocol, endovascular procedures were performed by experienced interventionalists using commercially available stent retrievers and aspiration catheters. At the end of the procedure recanalization was assessed; complete recanalization was considered if the Thrombolysis in Cerebral Infarction (TICI) score was 2b or 3.
For all patients, major workflow times were recorded. For procedural and outcome analysis DTAS patients were compared with DTER and DTCT patients with the same clinical features on admission: NIHSS score >10 and symptom onset <4.5 hours. Main recorded outcome measures were rate and time of complete recanalization (TICI≥2b), incidence of symptomatic intracranial hemorrhage8 at 24 hours, and NIHSS score at 24 hours and at discharge or 5 days. Dramatic clinical improvement was defined at 24 hours as ≥10 points drop in NIHSS score as compared with admission or NIHSS score ≤1.9
The study protocol was approved by the local ethics committee.
Statistical analysis
Descriptive and frequency statistical analyses were obtained using SPSS V.17.0 software. Categorical variables are presented as absolute values and percentages and the continuous variables as median±SD, if normally distributed, or median (interquartile intervals), if not normally distributed. Statistical significance for intergroup differences was assessed by Pearson χ2 or Fisher exact test for categorical variables and by Student t or Mann–Whitney U test for continuous variables. Multivariable logistic regression analyses were used to determine factors that could be considered as independent predictors of dramatic clinical improvement or shorter time to femoral puncture. A receiver operating characteristic curve analysis was used to calculate the best cut-off time point, after which dramatic clinical improvement is infrequent. A probability value of <0.05 was considered significant for all tests.
Results
Between December 2015 and November 2016 (12 months) 201 patients were included: 87 DTER (43.3%), 74 DTCT (36.8%), 40 DTAS (19.9%). The distribution of admission protocols according to study trimester is shown in figure 1. Baseline characteristics are shown in table 1.
Patient baseline characteristics according to study group

Distribution of admission protocols according to study trimesters (A) workflow times in minutes for each study group (B). DTAS, direct transfer to angiosuite; DTCT, direct transfer to CT; DTER, direct transfer to emergency room.
From the 40 patients in the DTAS group, 31 (77.5%) were transferred from another hospital where they had undergone a previous CT scan and 9 (22.5%) were primary admissions in our center. Ten (25%) of the DTAS patients finally did not received EVT: three patients (7.5%) showed an intracranial hemorrhage on Xpert-CT and seven (17.5%) did not show a treatable occlusion on the initial angiogram. The number of patients who did not receive EVT owing to the absence of a treatable occlusion on the initial angiogram, despite confirmation by previous CT angiography, was 1 (1.1%) in the DTER group and 4 (5.4%) in the DTCT group. The mean D2P time was significantly shorter in the DTAS group (17±8 min) than in the DTCT group (60±29 min; p<0.01). The D2P time was longer in the DTER group (90±53 min,) than in both other groups (p<0.01) (figure 1).
For analysis of the clinical outcome, only DTAS patients with confirmed LVO on the initial angiogram were included and compared with DTER and DTCT patients with confirmed LVO on the initial angiogram: DTAS: 30 patients, DTER: 86 patients, DTCT: 70 patients. There were no significant differences on baseline characteristics between groups (table 1), including mean time from symptom onset to hospital admission (DTAS: 179±14 min, DTER: 199±20 min, DTCT 167±18 min, p=0.21) or the mean time from femoral puncture to recanalization/end of procedure (DTAS: 61±6 min, DTER: 59±3 min, DTCT 57±3 min, p=0.88) (figure 1). However, the mean times from symptom onset to groin puncture (DTAS: 197±72 min, DTER: 279±156 min, DTCT 224±142 min, p=0.01) and symptom onset to recanalization (DTAS: 257±74 min, DTER: 355±158 min, DTCT 279±146 min, p<0.01) were longer in the DTER group. The rate of complete recanalization was similar between the three groups: DTAS: 83.3%, DTER: 82.6%, and DTCT: 72.5% (p=0.27). Safety was similar among the groups and we found no differences in the rate of symptomatic intracranial hemorrhage at 24 hours (DTAS: 5%, DTER: 6.9%, DTCT: 9.6%; p=0.66)
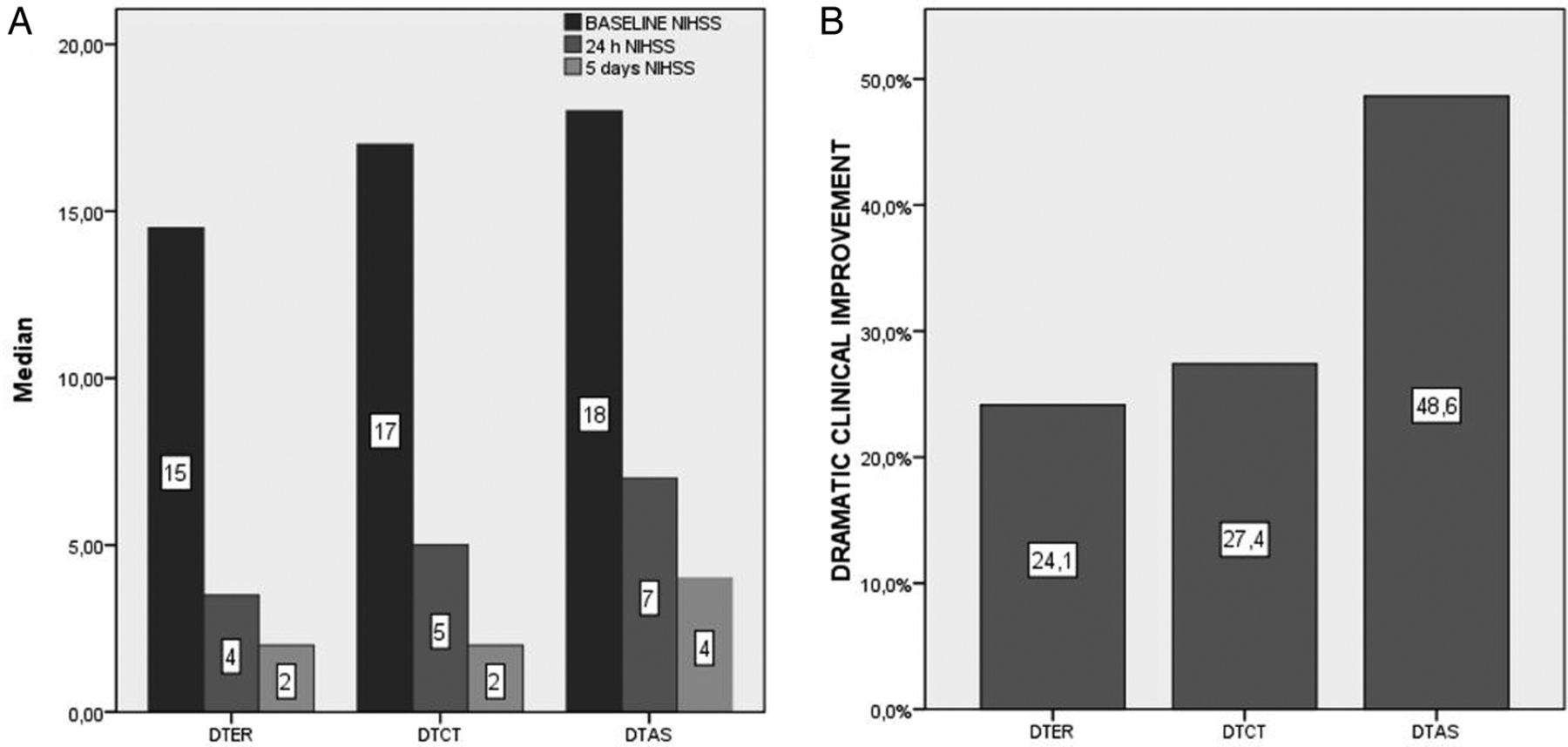
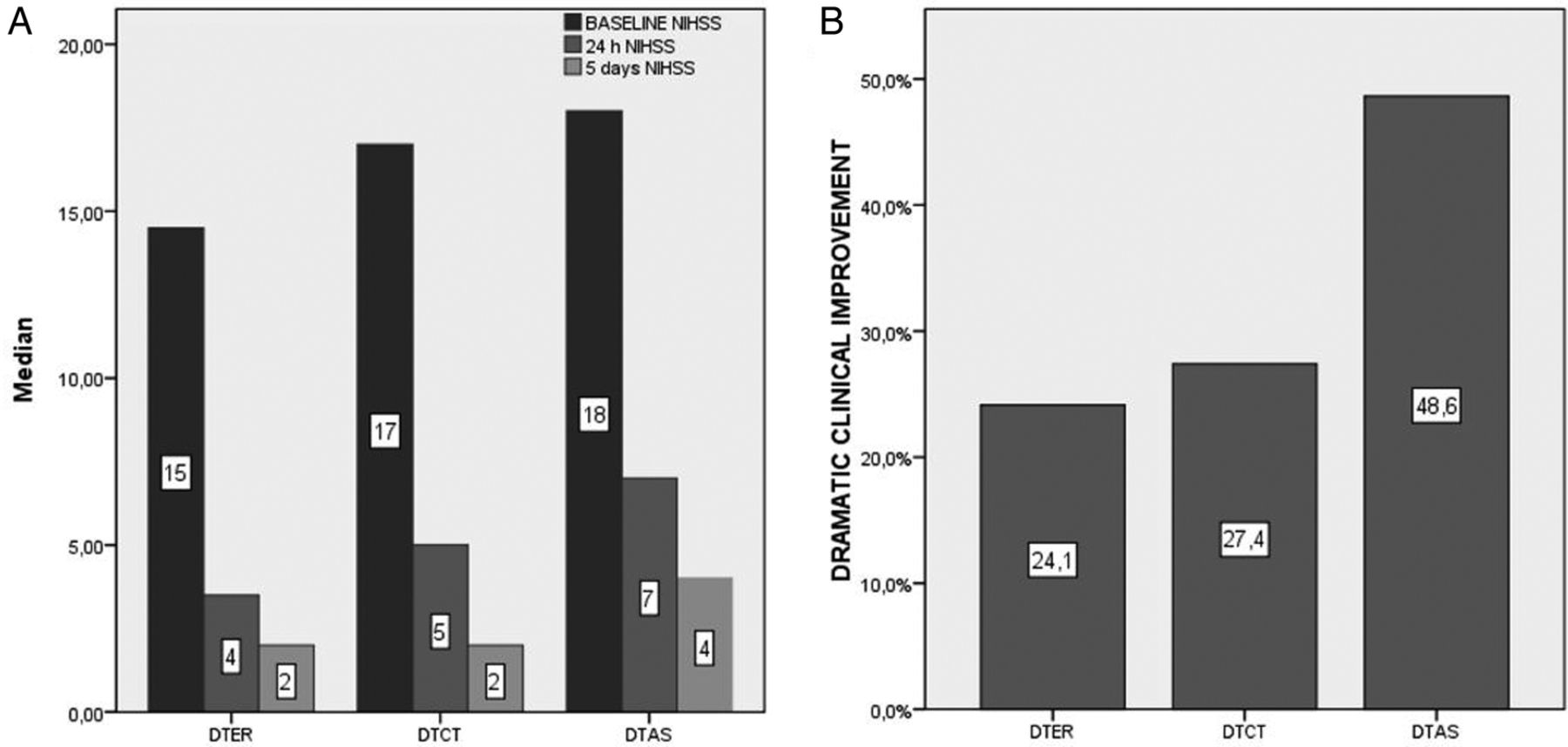
At 24 hours there were no differences in the median NIHSS score: DTAS 8 (5–15), DTER: 7 (2–18), DTCT: 8 (3–18) (p=0.81). However, the rate of dramatic improvement was significantly higher in the DTAS group, DTAS 48.6%, DTER 24.1%, DTCT 27.54% (p=0.01) (figure 2).
{kind=link}
{kind=link}
Median NIHSS on admission, 24 hours and day 5 or discharge (A), rate of dramatic clinical improvement (B) according to study groups. DTAS, direct transfer to angiosuite; DTCT, direct transfer to CT; DTER, direct transfer to emergency room; NIHSS, National Institute of Health Stroke Scale.
We studied possible reasons for the association between DTAS and dramatic improvement.
An adjusted model for admission NIHSS score, age, and recanalization, showed that shorter onset-to-puncture time was an independent predictor of dramatic clinical improvement (OR=1.23, 95% CI 1.13 to 1.33; p<0.01). Patients who experienced a dramatic clinical improvement showed shorter times from onset to femoral puncture (182±70 vs 215±90; p=0.03), and a receiver operating characteristic curve showed that >90% of such patients had a time from onset to femoral puncture of <298 min. The likelihood of achieving an onset-to-femoral puncture time <298 min was higher when the DTAS protocol was followed than with the other two protocols (OR=5.6; 95% CI 1.3 to 24.8; p=0.02).
Discussion
Our pilot study confirms that in patients with suspected acute stroke in the early time window, a direct transfer protocol to the angiosuite is feasible, safe, and helps to achieve a significant reduction in workflow times. Moreover, this time saving might be associated with improved outcome in some cases.
In the coronary field, results from the CathPCI registry showed that any delay in the ‘door-to-balloon’ time in primary percutaneous coronary intervention after a patient arrives at hospital is associated with higher mortality. Between 2005 and 2008 the number of hospitals in the registry that achieved door-to-balloon times of <90 min increased from 52% to 76%, reflecting successful implementation of the best practices associated with systems of care for these patients.10 In the same way, in the stroke field, investigators from Helsinki have shown that with multiple concurrent strategies it is possible to achieve very ambitious goals and reduce the median door-to-needle time for IV tPA treatment from 300 to 20 min.5
In 2011, the Brain Attack Coalition proposed D2P times of 2 hours as a benchmark for patients with stroke undergoing EVT.11 The following recommendation was given: “we encourage Comprehensive Stroke Centers to at least aim for a goal of 2 hours, given that patients with stroke need to undergo imaging before any endovascular procedure …”. A recent study showed that in EVT for acute stroke different major centers reported median D2P times ranging from 75 to 259 min, and that the D2P time was an independent predictor of further good outcome.6 More recently, the Endovascular Treatment for Small Core and Anterior Circulation Proximal Occlusion with Emphasis on Minimizing CT to Recanalization Times trial (ESCAPE) reported a median CT-to-puncture time of 51 min.12 It has become clear that as EVT for stroke evolves and increases in volume, the initial recommendations aiming for D2P times <120 min seem too lax and more ambitious goals should be set.
The in-hospital selection process aims to exclude from treatment those patients who will not benefit from endovascular procedures, either because the patient does not have an ischemic stroke, has an intracranial hemorrhage, does not have a LVO or has no salvable penumbral tissue anymore.
This selection process includes tools such as physical examination, and a wide range of neuroimaging techniques. Long comprehensive hyperselective protocols will increase the rate of treated patients with favorable outcome but may deny treatment to some patients who might still benefit from EVT. Moreover, too much time spent in the selection process may lower the beneficial effects of reperfusion, particularly in those cases in which a poor collateral circulation status puts the tissue at risk in a very time-dependent situation.13
On the other hand, reducing the complexity of the selection process may increase the number of patients undergoing angiography who would not benefit from the procedure, but can minimize the workflow times. This protocol may maximize the beneficial effect of thrombectomy, especially in patients with still viable tissue at risk but poor collateral circulation who are very time sensitive in the early time window.
Our study showed that primary angiography in selected patients with a cone-bean CT scan14 ,15 in the angiosuite as the only selection criterion can dramatically reduce the mean D2P to <20 min. This spectacular reduction in workflow times was achieved at an acceptable cost: 25% of the patients transferred to the angiosuite did not finally benefit from EVT either because they had an intracranial hemorrhage or because no treatable occlusion was identified on the initial angiogram. Moreover, we found no safety problems associated with the DTAS protocol.
In comparison with the other groups, DTAS could safely reduce the time to reperfusion by at least 40–70 min as compared with DTCT or DTER, respectively, and that could theoretically mean 15–30% increase in the chance of achieving a favorable outcome. In some cases, the D2P time could be reduced to 8 min. These results could only be achieved with a high level of organization and commitment of all members of the acute stroke team, including physicians, nurses, and other medical professionals.
Our study was not powered to show outcome differences between groups but rather to study the safety and feasibility of a DTAS protocol. Despite finding no differences in median NIHSS scores at 24 hours between groups, we did find a significantly higher prevalence of dramatic clinical improvement among patients who followed the DTAS protocol. This finding might be because in some patients the dramatic clinical improvement pattern can be very time dependent9 and, as shown in our analysis, the DTAS protocol increases the chances of recanalization within 5 hours from symptom onset. This study was performed with patients directly transferred from the field with no previous neuroimaging and patients from other centers where a CT had already been performed. Specific benefits of the DTAS protocol for each of these groups remain to be described in future larger studies.
In our study the DTAS protocol aimed to perform a cone-beam CT in all DTAS patients, whether or not they had had a previous CT scan in the referring center. It might be reasonable to explore the result of omitting the cone-beam CT in transferred patients who have already undergone a CT in the referring center (especially in short transfers, ie, <90 min from initial CT scan)
Conclusion
In a subgroup of patients with acute stroke direct transfer and triage in the angiosuite seems feasible, safe, and achieves significant reduction in hospital workflow times.
Acknowledgments
To all Stroke Unit and Neurointerventional staff members who made these results possible by their hard work and commitment.
References
Footnotes
Contributors Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work: MRi, SB, MRu, AT, PC, DH, MM, DR-L, NR, JJ, JP, CAM. Drafting the work or revising it critically for important intellectual content; MR. Final approval of the version to be published and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: MRi, SB, MRu, AT, PC, DH, MM, DR-L, NR, JJ, JP, CAM.
Funding The study was funded by Stryker Neurovascular. The funding source was not involved in study design, monitoring, data collection, statistical analyses, interpretation of results, or manuscript writing.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Vall Hebron Institut de Recerca ethics committee.
Provenance and peer review Not commissioned; externally peer reviewed.