Article Text

Abstract
Background The choice of the embolic agent and the embolization technique can have a significant impact on the success of endovascular embolization.
Objective To evaluate a novel iodinated copolymer-based liquid embolic agent (precipitating hydrophobic injectable liquid (PHIL)) in the porcine rete mirabile (RM), serving as an endovascular embolization model. Onyx, as an established liquid embolic agent, served as comparator.
Materials and methods Sixteen embolization procedures were performed using PHIL (n=8) or Onyx (n=8) as liquid embolic agent. Waiting time between injections was set to 30 or 60 s (n=4 per study group). Survival time after intervention was 2 hours or 7 days. Embolization characteristics (eg, procedure times, number of injections and volume of embolic agent) and embolization extent (percentage of embolized RM in post-interventional x-ray) were assessed. Post-interventional CT and histopathological analyses were performed.
Results Embolization characteristics and embolization extent were not significantly different for PHIL and Onyx, including subgroups (eg, embolization extent 44% vs 69% (medians); p=0.101). For PHIL, extension of the waiting time from 30 to 60 s led to a significantly higher embolization extent (24% vs 72% (medians); p=0.035). Moderate disintegration and mild inflammation of the embolized blood vessels were present for both embolic agents.
Conclusion PHIL is feasible for transarterial embolization in an acute and subacute endovascular embolization model. In this preliminary experimental in vivo study, embolization characteristics, embolization extent, and biocompatibility seem to be similar to those of Onyx.
- arteriovenous malformation
- liquid embolic material
- intervention
Statistics from Altmetric.com
Introduction
Endovascular embolization can play an important role in the management of some vascular malformations.1 Among those, cerebral arteriovenous malformations (AVM) are of particular relevance due to their ability to cause impairing neurological symptoms and their significant risk of hemorrhage.1 A variety of embolic agents are used for AVM embolization, of which the liquid embolic agents (LEA) ethylene-vinyl alcohol copolymer (EVOH) and n-butyl cyanoacrylate (n-BCA) are used most frequently.2 New embolic agents are being introduced in an attempt to improve embolization features such as embolization efficacy, intraprocedural handling and control, as well as to improve fluoroscopic visibility and reduce artefacts in post-interventional imaging.
There are several important requirements for an ideal embolic agent. First, there should be no complex preparation process. Second, it should be adequately visible in fluoroscopy during intervention and in post-interventional imaging without causing artefacts. Third, the precipitation process and, related to this, the plug formation time should be short enough not to extend the procedure time and long enough to enable adequate embolization control. Fourth, the embolization should be permanent without recanalization over time. Fifth, the embolic agent should be biocompatible (no major inflammatory or major vasodestructive reactions). Beside the requirements for the LEA itself, it is crucial and often complex to select the ideal embolic agent for the specific features of the vascular malformation to be treated, especially regarding viscosity/concentration and precipitation time.
Usually, embolization of an AVM is not performed by one single injection but through multiple injections. The injections are stopped several times due to reflux into the feeding artery or passage into the draining veins. The relevance of the pause time between two injections and its optimal duration has not yet been the focus of investigation and is presumably different for different embolic agents.
The aim of this study was to evaluate a novel iodinated copolymer-based LEA (precipitating hydrophobic injectable liquid (PHIL); MicroVention, Tustin, California, USA) in an in vivo endovascular embolization model in an acute setting and in a subacute setting with comparison to an established EVOH-based LEA. The principal aim of the acute setting was evaluation of feasibility, efficacy, and safety of PHIL, while the aim of the subacute setting was evaluation of mid-term effects including safety and biocompatibility.
Materials and methods
Embolic agents
PHIL is a newly developed LEA composed of a non-adhesive copolymer (polylactide-co-glycolide and polyhydroxyethylmethacrylate) dissolved in dimethyl sulfoxide (DMSO) with triiodophenol as iodine component, being covalently bound to the copolymer causing radiopacity. PHIL is a ready-to-use product that does not require any preparation and is pre-filled in syringes of 1 mL. Three different concentrations of PHIL are available: PHIL 25, 30 and 35 (increasing in viscosity; numbers indicating concentration in weight/weight).
Onyx (Medtronic Neurovascular, Irvine, California, USA) is composed of non-adhesive EVOH dissolved in DMSO in mixture with tantalum powder, the latter causing radiopacity. In order to ensure proper mixing of the tantalum powder, Onyx vials have to be kept on a shaker for at least 20 min prior to injection. Three different concentrations of Onyx are available: Onyx 18, 20 and 34 (increasing in viscosity; numbers indicating viscosity in centipoise).
For both LEAs the least viscous concentration (PHIL 25 and Onyx 18) was used in order to achieve deep penetration and consequently maximal filling of the embolization model.
Endovascular embolization model
The rete mirabile (RM) is a fine vascular network, consisting of a tangle of microarteries and arterioles, located bilaterally at the cranial base of pigs with a plexiform anastomosis through the midline.3 4 Its vessels resemble human arterioles with the same histological structures, including a vascular intima, tunica media (smooth muscle layer), vascular adventitia and connective tissue among the vessels.3 4 The RM is mainly supplied by the ascending pharyngeal artery (APA), which is a main branch of the common carotid artery (CCA). The porcine RM has been used as an endovascular embolization model by a number of investigators.5–8
Animal procedure
State Animal Care and Ethics Committee approval was obtained. Landrace pigs with a weight of 36–40 kg were used. Anaesthesia, animal preparation, and sacrifice were performed as previously described.9 Before and after intervention, non-enhanced CT scans (Somatom Definition Flash; Siemens, Forchheim, Germany), diagnostic angiographies (Artis zee; Siemens) using a 4 F catheter (Radiofocus Glidecath Vertebral 4 F; Terumo Europe, Belgium), positioned proximal to the origin of the APA, and x-rays (Artis zee; Siemens) were performed. Pigs were sacrificed either 2 hours (acute setting) or 7 days (subacute setting) after intervention. The animals that were designated to survive 7 days (two per study group) were fed standard food pellets and water ad libitum during the survival time; antibiotics and analgesics were administered daily. On day 7, final imaging (CT, diagnostic angiography and x-ray) was performed. After sacrifice, the RMs were explanted.
Embolization technique
A DMSO-compatible 1.3 F microcatheter (Headway Duo; MicroVention) was inserted coaxially through the guiding catheter. The catheter tip was positioned in the origin of the RM, defined as the first branching of the APA. Superselective diagnostic angiography confirmed the adequate embolization position. A syringe-catheter interface adapter was connected to the microcatheter. After flushing the microcatheter with 1 mL DMSO, pulsatile manual injection was performed using 1 mL DMSO-compatible syringes under fluoroscopy guidance. The qualitative visibility of the LEAs under fluoroscopy and in intra- and post-interventional x-rays was evaluated by applying a 3-point scale: 0, definitely not visible; 1, probably visible; and 2, definitely visible.10 11 Per injection, a certain amount of reflux into the APA was tolerated, defined as 5 mm distance of the APA. In case of reflux exceeding this limit, injection was stopped and paused for 30 or 60 s (see ‘Study groups’). In the case of complete embolization of the APA with imminent embolization of the CCA, in the case of embolization distal to the RM with imminent embolization of the brain, or in the case of embolization of the contralateral RM, the procedure was terminated. All interventions were performed in the same fashion by the same interventionalist (MAM with 12 years of experience in neurointerventions).
Study groups
In total, 16 embolization procedures were performed. For eight procedures PHIL 25 (Group PHIL) was used and for eight procedures Onyx 18 (Group Onyx) was used. Pause time between the injections was set to 30 or 60 s (n=4 per study group, respectively). Accordingly, four subgroups were defined: subgroup PHIL_30s (n=4), subgroup PHIL_60s (n=4), subgroup Onyx_30s (n=4), and subgroup Onyx_60s (n=4).
Study goals
The aim for each embolization procedure was the complete filling of the respective side of the RM. The following embolization characteristics were assessed: total procedure time, total injection time (defined as the duration of all injections per procedure), time per single injection (defined as the average time of a single injection), number of injections, and required volume of LEA per procedure (minus the dead space of the microcatheter of 0.35 mL). For determination of the embolization extent, the area of the respective side of the RM in the pre-interventional posterior-anterior (PA) angiogram was determined using Syngo Acquisition Workplace (Siemens) by delineating the perimeter of the RM. After embolization, the embolized portion of the RM in x-ray was delineated in the same fashion and used to determine the percentage of embolized RM (see figure 1E and F).
Histopathology
Following explantation, the RM were transferred to 4% buffered paraformaldehyde and fixed at 4°C overnight. The RMs were embedded in paraffin using a Shandon Excelsior ES apparatus (Thermo Scientific, Karlsruhe, Germany). Sections were cut to 4 µm and processed following routine protocols for hematoxylin/eosin (HE) and elastica van Giesson (EVG) staining. Images were taken using a NanoZoomer 2.0-HT digital slide scanner (Hamamatsu Photonics, Hamamatsu City, Japan).
Statistics
Prism software Version 7.02 (GraphPad, La Jolla, USA) was used for data analysis. Quantitative data are presented as medians (lower quartile; upper quartile). To evaluate statistical differences between Group PHIL and Group Onyx, the Mann–Whitney test was performed. To evaluate statistical differences between the subgroups (subgroup PHIL_30s vs PHIL_60s and subgroup Onyx_30s vs Onyx_60s), the Kruskal–Wallis test with a post-hoc Dunn’s test were performed. A p value of <0.05 was defined as the level of significance.
Results
All embolization procedures could be performed as planned. No technical failure such as catheter occlusion or catheter entrapment was observed. All animals survived the designated survival time without any apparent physical restriction. After 7 days, angiographically there was no recanalization of the embolized RM for any of the LEAs.
During and after embolization, both LEAs were definitely visible under fluoroscopy as well as in intra- and post-procedural x-rays (figure 1A and B). Beam-hardening artefacts in post-interventional CT were distinct for Group Onyx and comparatively low for Group PHIL (figure 1C and D). An example of an analysis of the embolization extent is shown in figure 1E and F. Embolization characteristics and embolization extent are summarized in table 1; embolization extent is illustrated in figure 2.

Visibility in x-ray and in CT with an example of an analysis of the embolization extent. (A, B) X-ray obtained after embolization, shown for subgroup PHIL_60s (A) and subgroup ONYX_30s (B). Note the adequate visibility of both LEAs. (C, D) Post-interventional CT imaging, axial plane, standard window (width: 340, level: 60). There were mild beam-hardening artefacts for PHIL (C) and distinct beam-hardening artefacts for Onyx (D). The PHIL cast was definable at the skull base (black arrows). Due to the beam-hardening artefacts, the ONYX cast was not definable. (E, F) An example of an analysis of the embolization extent shown for an embolization procedure of subgroup PHIL_60s. The delineated area was 1.44 cm² in the pre-interventional angiography (E) and 1.14 cm² in the post-interventional x-ray (F), resulting in an embolization extent of 79%.
Embolization characteristics and embolization extent
Comparing Group PHIL and Group Onyx, the volume of LEA per procedure was significantly higher for Group Onyx (0.15 mL vs 0.45 mL (medians); p<0.001). There were no significant differences concerning total procedure time, total injection time, or number of injections. The embolization extent was not significantly different for Group PHIL and Group Onyx (44% vs 69% (medians); p=0.101).
In the subgroup analysis, the volume of LEA per procedure was significantly different in the Kruskal–Wallis test but without significant differences in the post-hoc Dunn’s test. For PHIL, extending the pause time from 30 s to 60 s led to a significantly higher embolization extent (24% vs 72% (medians); p=0.035). Embolization characteristics were not significantly different between subgroups PHIL_30s and PHIL_60s. For Onyx, the embolization characteristics and the embolization extent were not significantly different between the subgroups ONYX_30s and ONYX_60s.
Macroscopically, the embolized RMs were harder than the non-embolized contralateral RM. PHIL was visible as white material and showed a solid, crumbly consistency. Onyx was visible as black material and showed a rubber-like consistency.
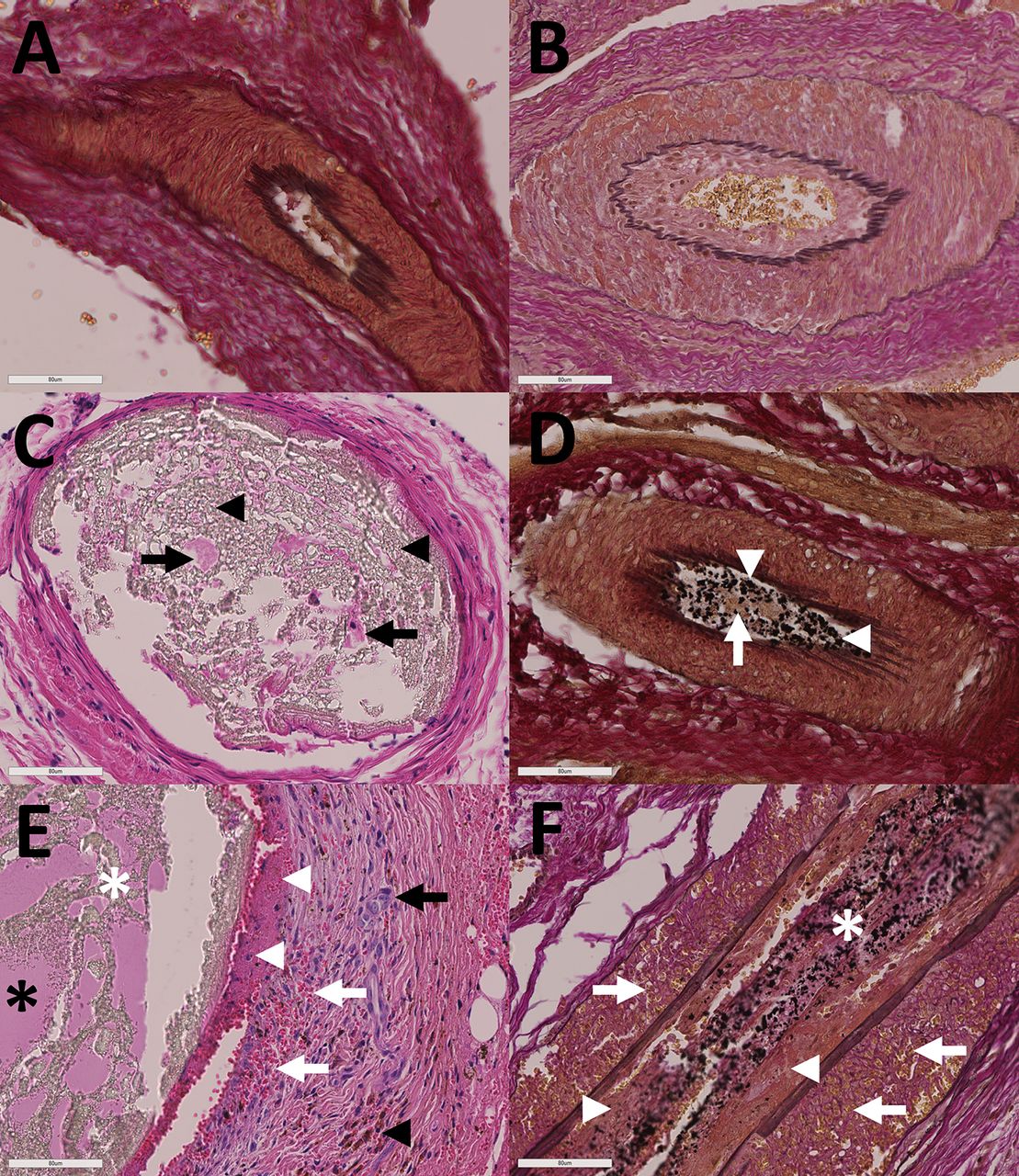
Histopathological findings are illustrated in figure 3. Both embolic agents were identified as amorphous material of white appearance for PHIL and black appearance for Onyx. The luminal diameter of embolized vessels reached from 80 to 380 µm for PHIL and from 90 to 420 µm for Onyx. The embolized vessels were filled with a mixture of LEA and fibrin accompanied by thrombus attached to the vascular lining. In the subacute series, thrombosis was more pronounced. For both LEAs, no extravasation was observed in either the acute or the subacute specimens. After 7 days, signs of moderate disintegration of the embolized blood vessels were observed for both embolic agents, represented by thinning of the tunica media and by moderate intramural hemorrhage. After 7 days, signs of mild inflammation were present for both Group PHIL and Group Onyx, represented by leukocyte infiltration of the vessel wall. No necrosis was evident. No multinucleated foreign body giant cells were detected. Recanalization of the embolized vessels was not observed in either series.

Illustration of the embolization extent. The embolization extent was not significantly different for PHIL and Onyx. Extension of waiting time from 30 to 60 s led to a significantly higher embolization extent for PHIL.
{kind=link}
{kind=link}
{kind=link}
Histopathological findings. (A, B) Group PHIL, elastica van Giesson (EVG) staining (A) and Group Onyx, EVG staining (B). Subacute specimens. Non-embolized blood vessels did not show pathologic alterations. (C, D) Group PHIL, HE staining (C) and Group Onyx, EVG staining (D). Acute specimens. PHIL was visible as amorphous material with white appearance (black arrowheads), Onyx as amorphous material with black appearance (white arrowheads) inside the blood vessels of the RM. Fibrinous thrombus was seen within the embolic agent cast for both embolic agents (black and white arrows). There was no vascular pathology in the acute specimens. Note the preparation artefacts inside the vessel lumen (white areas) caused by dissolving of the embolic agents during histopathological workup (also evident in the subacute specimens; see also figure 2E and F). (E, F) Group PHIL, HE staining (E) and Group Onyx, EVG staining (F). Subacute specimens. For both embolic agents there was moderate intramural hemorrhage indicated by erythrocyte infiltration of the vessel wall, predominantly within the tunica media (white arrows; erythrocytes stained red in HE and yellow in EVG staining), and by intramural deposition of hemosiderin, predominantly within the deeper layers of the tunica media (black arrowhead). Additionally, there was thinning of the tunica media for both embolic agents. Leukocyte infiltration of the vessel wall, mainly affecting the tunica media, was present for both study groups (black arrow). Inside the vessel lumen there was a mixture of fibrin (black asterisk) and embolic agent (white asterisk), accompanied by thrombus attached to the vascular lining (white arrowheads) for both study groups.
Discussion
In this experimental study the novel LEA PHIL was evaluated and compared with an established LEA in an in vivo endovascular embolization model in an acute and in a subacute setting. As a major finding of this study, technical embolization characteristics as well as embolization extent were not significantly different for PHIL and Onyx. With respect to PHIL only, pause time between injections had a significant influence on the embolization extent.
PHIL is a novel, inherently radiopaque, copolymer-based LEA. Four studies reported preliminary clinical experience with PHIL and demonstrated effectiveness and safety of PHIL for AVM and arteriovenous fistula (AVF) embolization, although for a limited number of cases.12–15 Gentric et al showed that PHIL is effective for endovascular embolization in the RM; however, the focus of their study was the technique of embolization and not the specific characteristics of the LEAs.16 Onyx is an established LEA, being used for embolization of vascular malformations since the 1990s.17 It has gained increasing acceptance, especially for embolization of AVMs and AVFs.18 19 Despite its high embolization potential and the advantages of Onyx over other LEAs, such as n-BCA, there are still several shortcomings reported by neurointerventionalists. These include long procedure times caused by the relatively long precipitation process of Onyx, impaired visibility during longer embolization procedures and impaired visibility of the microcatheter tip during embolization, artefacts in control CT imaging and in imaging for irradiation planning, and also its pre-interventional preparation process.20
Knowing the embolization-specific properties of a LEA is crucial when using a novel agent for embolization in clinical practice. Since embolization characteristics (eg, procedure times and number of injections) were not significantly different for PHIL and Onyx, the findings of this study suggest that the embolization technique, which is generally applied for embolization with Onyx, can be easily adapted to embolization with PHIL.
According to the results of this experimental study, the embolization extent, which can be seen as a marker of therapeutic efficacy in clinical AVM embolization, seems to be similar for PHIL 25 and Onyx 18. For PHIL, extending the waiting time from 30 to 60 s led to a significantly higher embolization extent. Precipitation times are different for different LEAs (eg, 3 min for PHIL and 5 min for Onyx, as provided by the manufacturers). The waiting time between injections until a certain degree of precipitation of the LEA is important, since not waiting for a long enough period of time can result in distal off-target embolization and waiting too long can lead to premature embolization of the feeding artery and the proximal part of the AVM or in microcatheter occlusion, eventually resulting in ineffective treatment.20–22 Nevertheless, it has to be mentioned that the precipitation time and, accordingly, also the pause time can be significantly influenced by various factors such as the plug length, the calibre of the respective blood vessel, or the flow rate in the vascular malformation.19 23 According to the results of our study, for PHIL a waiting time of 60 s seems to be appropriate for effective and controllable embolization.
Both embolic agents used in this study were visible during embolization under fluoroscopy and after embolization in x-ray. Adequate intraprocedural visibility of an embolic agent enables real-time control of target embolization and can thus reduce the risk of unwanted embolization of normal intracranial arteries, shorten the procedural time, and ultimately improve the success rate.23 24 Furthermore, real-time control can provide immediate intraprocedural feedback at a time when this information could help optimize the procedure.23 24
After embolization of cerebral AVMs with Onyx, evaluation of post-interventional CT imaging for assessment of complications (eg, bleeding), evaluation of treatment success or irradiation planning is often impeded due to significant beam-hardening artefacts caused by the tantalum powder.25 26 The lower intensity of beam-hardening artefacts for PHIL, which was also reported in the studies using PHIL in clinical practice, can be seen as an advantage for PHIL over Onyx.12–15
The lower volume of LEA per procedure for PHIL compared with Onyx may be a sign for a higher material-specific efficiency. However, in this regard, the higher embolization extent seen in Group Onyx has to be noted, even though it was not statistically significant. Furthermore, the volume inside the APA was not assessable.
Both LEAs caused moderate disintegration and mild inflammation of the embolized blood vessels within a period of 7 days. Mild inflammatory reactions and even necrosis are also reported within the first weeks after AVM embolization in clinical practice.27 28 Besides adverse effects caused by the active substance of the LEAs themselves (EVOH for Onyx and the abovementioned copolymers for PHIL), the organic solvent DMSO, being part of both PHIL and Onyx, is known to cause significant dose-related local angiotoxic effects.29 30 The lack of foreign body giant cells in our study can be explained by the relatively short follow-up period of 7 days, because the earliest observation of these cells is approximately 1 week after Onyx embolization.27 28 Natarajan et al reported angionecrosis after AVM treatment with Onyx in 89% of patients who received resection ≥15 days after the first embolization and in only 31% of patients with an interval of <15 days between the first embolization and surgical resection.28 Accordingly, for the development of embolization-related angionecrosis, a certain period of time is needed. This might be an explanation for the lack of necrosis in our study. Recanalization, which is generally unwanted after AVM embolization, was not observed for either of the LEAs. According to the abovementioned study of Natarajan et al, recanalization at the earliest occurs 40 days after embolization.28 Clinical and experimental long-term follow-up studies are needed to assess the incidence of recanalization after AVM embolization using PHIL. Despite potential adverse effects, according to the available long-term experience, Onyx generally is a safe agent for embolization of vascular malformations. According to the results of our subacute experimental study, similarly to Onyx, PHIL can be regarded as biocompatible with mild tolerable adverse effects to the embolized vasculature.
The presence of thrombus beside LEA inside the embolized vessels is in accordance with histopathological findings after successful AVM embolization in clinical practice and should not be misinterpreted as a sign of ineffective embolization.27
There were some limitations in our study. First, the number of trials was small; however, the findings were consistent in the different groups. Second, transferability of an in vivo model to clinical practice is generally limited. Third, the size and quality of the RM are variable, which could have biased the results of this study. Fourth, although the RM is similar to an AVM, it does not contain arteriovenous shunts. The creation of an AVF could have made this model more similar to an AVM. Fifth, there might be more or other optimal pause times besides those used in this study. Sixth, the analysis of the embolization extent (delineating the perimeter of the RM) does not take into account central filling defects or the density of the LEA.
Conclusions
PHIL is feasible for endovascular embolization in an acute and subacute in vivo endovascular embolization model. In this preliminary experimental in vivo study, embolization characteristics, embolization extent, and biocompatibility seem to be similar to those of the established LEA Onyx. For PHIL, the waiting time between injections seems to have an influence on the embolization extent.
References
Footnotes
CMS and MAM contributed equally.
Contributors All listed authors contributed to the work. DFV, CMS and MAM acquired, analyzed and interpreted data for the work; designed the study; drafted the manuscript and approved the final manuscript. RO acquired, analyzed and interpreted data for the work; drafted the manuscript and approved the final manuscript. AD analyzed and interpreted data for the work; drafted the manuscript and approved the final manuscript. JP, CU, HUK and MB analyzed and interpreted data for the work; drafted the manuscript and approved the final manuscript.
Funding This study was technically supported by MicroVention (Tustin, USA) and Medtronic Neurovascular (Irvine, USA).
Competing interests JP reports personal fees from Siemens Healthcare GmbH and personal fees from Stryker GmbH & Co KG, outside the submitted work. HK reports grants, personal fees and non-financial support from Siemens, personal fees from Boehringer Ingelheim, personal fees and non-financial support from Bayer, personal fees from GSK, personal fees from Novartis, personal fees from Astra Zeneca, personal fees from Philips, personal fees from Bracco, outside the submitted work. MB: reports board membership: DSMB Vascular Dynamics; consultancy: Roche, Guerbet, Codman; grants/grants pending: DFG, Hopp Foundation, Novartis, Siemens, Guerbet, Stryker, Covidien; payment for lectures (including service on speakers' bureaus): Novartis, Roche, Guerbet, Teva, Bayer, Codman. HK: reports grants, personal fees and non-financial support from Siemens, personal fees from Boehringer Ingelheim, personal fees and non-financial support from Bayer, personal fees from GSK, personal fees from Novartis, personal fees from Astra Zeneca, personal fees from Philips, personal fees from Bracco, outside the submitted work. MM: has received consulting honoraria, speaker honoraria, and travel support outside this work from Codman, Covidien/Medtronic, MicroVention, Phenox, and Stryker. All other authors have no competing interests to disclose.
Provenance and peer review Not commissioned; externally peer reviewed.