Article Text

Abstract
Introduction It remains unclear whether patients presenting with large vessel occlusion strokes and mild symptoms benefit from thrombectomy.
Objective To compare outcomes of endovascular therapy versus medical management in patients with large vessel occlusion strokes and National Institute of Health Stroke Scale (NIHSS) score ≤5.
Methods This was a retrospective analysis combining two large prospectively collected datasets including patients with (1) admission NIHSS score ≤5, (2) premorbid modified Rankin Scale (mRS) score 0–2, and (3) middle cerebral-M1/M2, intracranial carotid, anterior cerebral or basilar artery occlusions. Groups receiving (1) endovascular treatment and (2) medical management were compared. The primary and secondary outcome measures were NIHSS shift (discharge NIHSS minus admission NIHSS) and the rates of mRS 0–2 at discharge and 3–6 months, respectively. Univariate, multivariate, and matched analyses were performed.
Results Eighty-eight patients received medical management and 30 thrombectomy. Multivariable analysis indicated thrombectomy was the only predictor of favorable NIHSS shift (β −3.7, 95% CI −6.0 to −1.5, p=0.02), as well as independence at discharge (β −21.995% CI −41.4to −20.8, p<0.01) and 3–6-month follow-up (β −21.1, 95% CI −39.1 to −19.7, p<0.01). A matched analysis (based on age, baseline NIHSS and intravenous tissue plasminogen activator use) produced 26 pairs. Endovascular therapy was statistically associated with lower NIHSS at discharge (p=0.04), favorable NIHSS shift (p=0.03), and increased independence rates at discharge (p=0.03) and 3–6-month follow-up (p=0.04).
Conclusion In patients presenting with minimal stroke symptoms (NIHSS score ≤5) and large vessel occlusion strokes, mechanical thrombectomy appears to be associated with a favorable shift of NIHSS at discharge, as well as higher rates of independence at discharge and long-term follow-up. Confirmatory prospective studies are warranted.
- stroke
- intervention
- thrombectomy
Statistics from Altmetric.com
Introduction
Mechanical thrombectomy is considered the standard of care for patients with large vessel occlusion strokes (LVOS) presenting with National Institutes of Health Stroke Scale (NIHSS) score ≥6 within 6 hours.1 However, it remains unclear whether thrombectomy benefits patients with LVOS with milder clinical presentations.2 Considering that the underlying presence of a large vessel occlusion is the main predictor of deterioration in patients with mild strokes and that contemporary thrombectomy can be performed with considerable efficacy and safety, endovascular therapy may represent a viable treatment modality with low NIHSS at presentation.3
We aim to compare endovascular therapy (ET) with medical management in patients with LVOS presenting with mild stroke symptoms by using two large prospectively collected stroke cohorts.
Methods
This was a multicenter retrospective analysis of prospectively collected datasets from three comprehensive stroke centers, which received institutional review board approval at the participating institutions and was Health Insurance Portability and Accountability Act compliant.
Grady Endovascular Stroke Outcomes Registry (GESTOR), a prospectively maintained institutional registry of all consecutive patients with LVOS treated with ET at Grady Memorial Hospital;
Screening Technology and Outcomes Project in Stroke (STOPStroke), a prospectively collected cohort enrolled at the Massachusetts General Hospital and the University of California at San Francisco including all consecutive patients with suspected stroke undergoing admission non-contrast CT and CT angiography within 24 hours of symptom onset. Patients were excluded if there was evidence of intracranial hemorrhage on non-contrast CT.
Patient selection
Two groups were identified and compared: ET and medical management groups. The interventional arm originated from the GESTOR cohort and was composed of all consecutive patients treated with endovascular therapy between August 2012 and September 2016. The medical management arm obtained from the STOPStroke cohort and comprised all consecutive patients given medical therapy alone between March 2003 and September 2005. Patients with NIHSS score ≤5 on arrival at the comprehensive stroke center who were confirmed to have middle cerebral artery M1 or M2, intracranial carotid artery (ICA), anterior cerebral artery or basilar artery occlusion were included. Patients who were not independent (modified Rankin Scale (mRS) score >2) at baseline were excluded. The NIHSS score was assessed on arrival by a certified neurologist. Ischemic core was evaluated by the Alberta Stroke Programme Early CT Score (ASPECTS). Hemorrhagic transformation was graded by the European Cooperative Stroke Study and reperfusion rates by modified Thrombolysis in Cerebral Infarction (mTICI) criteria.
Outcome analysis
The primary outcome measure was a change in the NIHSS (discharge NIHSS minus admission NIHSS = ‘NIHSS shift’).3 4 Secondary efficacy outcome included the rates of mRS score 0–2 (good outcome) at discharge and long-term follow-up (3 months for the interventional cohort and 6 months for the medical therapy group).
Matching methodology
A matching method based on weighted Euclidean distances was used to obtain a pair of subjects considered to be the nearest neighbors in a three-dimensional space of age, baseline NIHSS, and IV tissue plasminogen activator (tPA) use, as previously described.5 The distance between each intervention–control pair was computed using the %FIND_NEIGHBORS Macro in SAS University Edition (SAS Institute, Cary, North Carolina, USA).
After matching, the distribution of Euclidian distances was studied to identify outliers and a threshold was determined as follows: threshold=Q75+1.5*(Q75−Q25) where Q25 and Q75 are respectively the 25th and 75th percentile.6 Pairs with distances greater than the threshold were considered extreme values at the tail of the distribution and eliminated from further consideration.
Statistical analysis
Continuous variables were reported as median (IQR). Categorical variables were reported as proportions. Between groups, comparisons for continuous/ordinal variables were made with, Mann–Whitney U or Wilcoxon rank sum test, as appropriate. Categorical variables were compared by Χ2 test, Fisher exact test, or McNemar test for discordant pairs, as appropriate. Multivariable linear regression analyses for predictors of NIHSS shift and logistic regression for predictors of discharge and follow-up mRS were performed for variables at the 0.1 level of significance on univariate analysis. The parameters of the final models were estimated with bootstrapping (2000 samples). Significance was set at p<0.05 and all p values were two-sided. Statistical analysis was performed using IBM SPSS Statistics 23 (IBM-Armonk, New York, USA).
Results
Of 822 GESTOR patients treated within the study period, 30 fit the inclusion criteria and were included in the interventional arm. Also, of 741 patients enrolled in the STOPStroke cohort, only one patient with low NIHSS was treated with intra-arterial therapy and hence excluded, leaving 88 patients in the medical management group.
Primary analysis
The primary analysis (table 1) indicated comparable demographics with the following exceptions: interventional patients were younger, had higher rates of diabetes, higher baseline NIHSS, and higher frequency of IV tPA use. Patients receiving medical management had a lower frequency of basilar occlusions and higher prevalence of intracranial carotid occlusions. The interventional group had more favorable NIHSS shift as well as discharge and long-term follow-up rates of good outcomes (figure 1). Multivariable analysis indicated thrombectomy as the only predictor of favorable NIHSS shift, as well as independence at discharge and long-term follow-up (table 2).
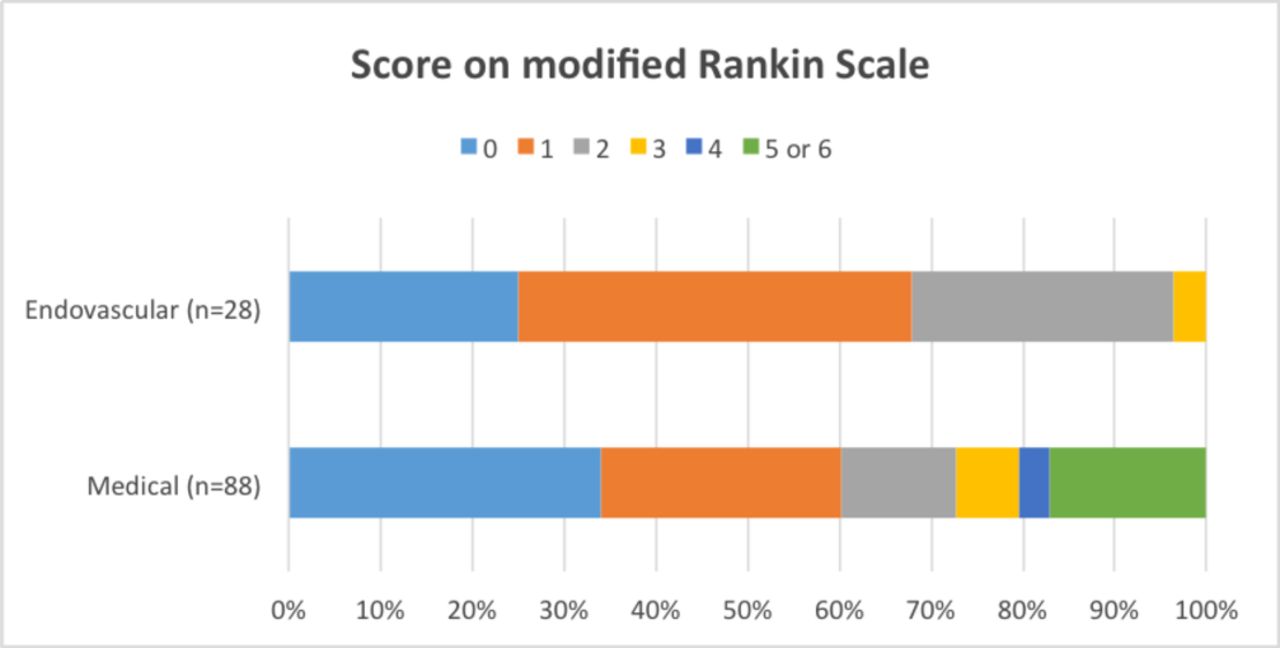
Functional outcome at follow-up according to the score on the modified Rankin scale.
Baseline characteristics and outcomes of medical therapy as compared with intervention through unmatched and matched analyses
Multivariable regression models for predictors of (A) NIHSS shift; (B) modified Rankin Scale at discharge and (C) modified Rankin Scale at follow-up
Matched analysis
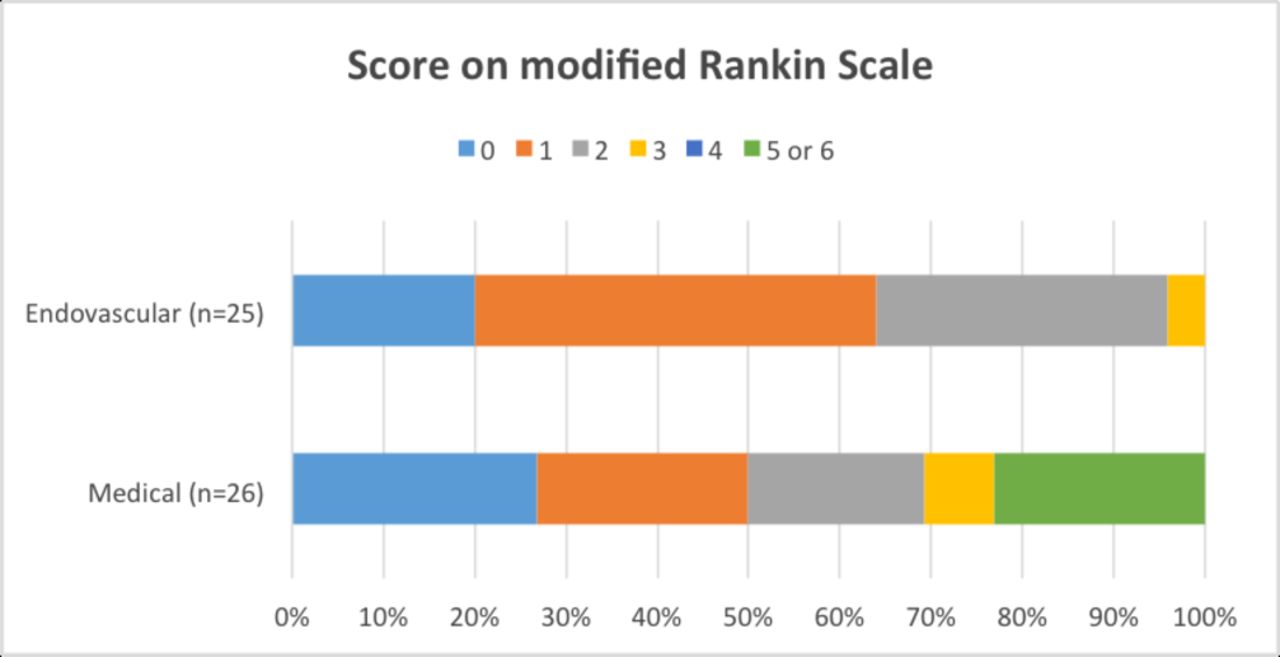
The medical therapy and interventional patients were matched for age, baseline NIHSS and IV tPA use. Of the 29 generated pairs, three had a Euclidian distance higher than the preset threshold and were therefore eliminated from further consideration leaving 26 pairs for the analysis (table 1). The matching led to well-balanced groups, with the exception of a higher frequency of atrial fibrillation in the interventional cohort. Endovascular therapy was associated with lower NIHSS at discharge, favorable NIHSS shift, and with higher chances of independence at discharge and long-term follow-up (figure 2).

{kind=link}
{kind=link}
Functional outcome at 90 days according to the score on the modified Rankin Scale (matched populations).
Interventional data
The median (IQR) time from hospital arrival to arterial puncture was 83 min (59–158). Twenty patients (67%) were treated within 1–4 hours and 8 (27%) after 4 hours from hospital arrival due to neurological worsening. The median procedure length (from puncture to last picture) was 71 min (52–90). General anesthesia was used in 23% of cases. Stent-retriever technology was used in 24 (80%) of the cases, while 4 (13%) underwent treatment with contemporary thromboaspiration technology, one patient received intra-arterial alteplase, and one had a subocclusive distal middle cerebral artery M2 occlusion that was not approached after cervical ICA stenting. One intracranial stent was used, while four cervical ICA angioplasties/three stents were performed. Successful reperfusion (mTICI score 2b–3) was achieved in 93% and complete reperfusion (mTICI score 3) in 46%.
Discussion
We have demonstrated that, in comparison with medical therapy, mechanical thrombectomy in patients with LVOS with minimal symptoms on presentation was associated with improved clinical outcomes, including more favorable NIHSS shift as well as discharge and long-term follow-up rates of independence.
As most patients with stroke present with an NIHSS score of ≤5 and more than half of the patients with LVOS have an NIHSS score ≤10, it is critical to define the best strategy to treat these patients.7 8 The IV tPA literature indicates that a large proportion (~1/3) of those presenting within 3 hours may be excluded from IV thrombolysis by being considered too good to treat.4 The reality is that a large proportion of the patients with mild or rapidly improving symptoms have an unchanged or worse NIHSS at discharge.4 Notably, it has been shown that in patients presenting with an NIHSS score ≤5, those with poor 90-day outcomes had a median NIHSS that was three points higher, indicating that favorably shifting a small number of points can be sufficient for a good outcome.9
The underlying presence of a large vessel occlusion has been consistently demonstrated to predict clinical deterioration in patients with mild strokes on initial presentation.10–12 Although the meta-analysis of recent randomized thrombectomy clinical trials failed to confirm a definite benefit for thrombectomy in patients with NIHSS score ≤10,2 these patients were a small proportion of the sample which likely underpowered the analysis. Therefore, mechanical thrombectomy may still constitute a reasonable option for this patient group considering their predisposition for clinical deterioration.
Reports comparing medical therapy with endovascular intervention in mild strokes are scarce. A few studies have indicated feasibility, safety, and potential benefit of the interventional approach for LVOS with mild clinical presentation. A study comparing 41 treated (IV thrombolysis, endovascular therapy, or both) and 47 untreated patients presenting with LVOS and NIHSS score ≤5 indicated a favorable shift in the treated group as compared with the non-treated patients (−2.5 vs 0; p<0.001) as well as better clinical outcomes at 3 months in the treated arm after adjustments.13 The limitation was the combination of different treatment modalities in the treated group, which blurs the potential impact of endovascular therapy. Another study with similar design, which compared 23 patients presenting with a higher NIHSS inclusion threshold (NIHSS score ≤7) and LVOS treated with either IV tPA and/or endovascular therapy against 39 controls, suggested a potential beneficial impact of reperfusion therapy in outcomes (90-day mRS score 0–2: 78% vs 53%, p=0.02).14
We have previously published the only available prospective study directly comparing medical management with thrombectomy in patients with LVOS presenting with a very low NIHSS score (≤5).3 Notably, the intention-to-treat design of this study allowed patients allocated to medical therapy to receive rescue thrombectomy if clinical deterioration occurred. In comparison with primary medical management, primary thrombectomy was independently associated with a favorable shift in the discharge NIHSS score (−2.5 vs 0; p<0.01). The current study has external consistency with a similar degree of shift of NIHSS at discharge (−3 in the interventional group vs −1 in the medical therapy group) to that in the aforementioned studies. Moreover, we corroborated the positive impact of thrombectomy in the NIHSS during the inpatient course, and also showed that thrombectomy was independently associated with better rates of independence at discharge and long-term follow-up.
Despite the prospective data collection, this study carries the limitations inherently associated with retrospective analyses. The different follow-up time points (3 months for the interventional group vs 6 months for the medical therapy group) should not have a significant influence on the study results considering that (1) the primary analysis was discharge outcome and (2) the theoretical advantage of more recovery time should have favored the medical therapy group.15 It should be noted that the groups derived from different cohorts and study periods; the advancements in medical management over time might have played an important role in the study results. A significant proportion of patients in the interventional arm were treated after deteriorating clinically as a rescue approach (>1/4 after 4 hours of arrival), and results could theoretically have been improved if thrombectomy had been performed beforehand. A significant strength of this study is the homogeneous approach for the medical therapy arm, in which all consecutive patients (but one) who presented with an NIHSS score ≤5 within the 3-year study period were consistently treated medically, reducing the possibility of residual confounding. Finally, the thrombectomy cohort was treated with contemporary techniques and should be representative of the current real-world practice.
Conclusion
In patients with LVOS presenting with minimal stroke symptoms (NIHSS score ≤5), mechanical thrombectomy appears to be associated with a favorable shift of NIHSS at discharge, as well as higher rates of independence at discharge and long-term follow-up. Confirmatory prospective studies in this patient population are warranted.
References
Footnotes
DCH and FOL contributed equally.
Contributors DCH: Study conception, design of the work, acquisition of data, interpretation of data, drafting of the manuscript. FOL, MB: Data acquisition, statistical analysis, critical revision of manuscript. JAG, GSS, MHL, KF, WK: Data acquisition, interpretation of data, critical revision of manuscript. MRF: Interpretation of data and critical revision of manuscript. RGN: Study conception, design of the work, critical revision of manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests DCH, FOL, MB, JAG, GSS, MHL, KF, WK, MRF. No relevant disclosures. RGN: Stryker-Neurovacular (Trevo-2&DAWN/Trial PI), Covidien (SWIFT&SWIFT-PRIME/Steering-Committee,STAR Trial/Core-Lab), Penumbra (3-D Separator Trial/Executive-Committee).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The unpublished data from this dataset is held by Grady Memorial Hospital/Emory University (DCH/RGN) as well as Massachusetts General Hospital (MHL). Requests for data sharing would be required to be discussed with them directly.