Article Text

Abstract
Introduction Syringe aspiration for manual aspiration thrombectomy (MAT) is a cost- and time-efficient alternative to an aspiration pump with likely similar efficacy. It is counterintuitive to expect the pump to perform better than direct vacuum with a syringe, as the pump must deliver vacuum additionally through a canister and meters of tubing.
Objective To present in vitro and clinical results of MAT with a syringe.
Methods An in vitro analysis was performed comparing vacuum pressures generated by syringe aspiration and with pump aspiration. This was then complemented with prospective clinical data providing details of angiographic and clinical outcomes for syringe MAT.
Results The in vitro analysis demonstrated that equal to slightly greater vacuum pressures were generated by a 60 cc syringe as compared with the pump in both static and partial flow conditions. In our clinical series, 106/113 acute stroke thrombectomies over a 6-month period were performed with syringe MAT on the first pass. Syringe usage instead of pump tubing and a canister led to a total savings of $58 300. The rate of Thrombolysis in Cerebral Infarction 2b/3 recanalization was 93%. Adjunctive stentriever usage was performed in 23% of cases. Median puncture to reperfusion time was 25 min; mean change in National Institute of Health Stroke Scale score at 24 hours was an improvement of 5.1 (median 6). The in-hospital mortality rate was 10%. Seventy percent of patients were discharged to home (modified Rankin Scale (mRS) score 0–2) or a rehabilitation facility (mRS score 2–4).
Conclusion MAT using a syringe is a safe, fast, and more cost-effective approach than using an aspiration pump.
- thrombectomy
- stroke
Statistics from Altmetric.com
Introduction
Since inception of the concept of intracranial thromboaspiration as described by Chapot and colleagues in 2002,1 there has been considerable evolution of manual aspiration thrombectomy (MAT) as applied to acute ischemic stroke.2–4 Following the original large retrospective publications describing MAT,2–4 the phrase, "a direct aspiration first pass technique" (ADAPT) was more recently popularized, emphasizing usage of MAT or pump aspiration on the first pass.5
Although well-known randomized clinical trials that demonstrated better clinical outcomes after mechanical thrombectomy as compared with medical management used stentrievers,6–8 aspiration catheter technology has evolved considerably. Many centers empirically perform MAT, a cost-efficient and potentially time-efficient alternative to stentriever-mediated thrombectomy.9–11 The recent ASTER trial demonstrated similar angiographic and clinical outcomes between patients undergoing thrombectomy using aspiration as compared with stentrievers.12 This trial, together with innumerable case series, reinforces the safety and feasibility of this technique.2 9–11
Oft-cited literature evaluating MAT has described the use of an aspiration pump.9–11 This requires an unsterile assistant to be available to attach added tubing to an aspiration pump. In contrast to simply attaching a sterile syringe to the aspiration catheter, the use of an aspiration pump adds time and cost to the procedure. It is counterintuitive to expect the pump to perform better than excellent direct vacuum with a syringe, as the pump must deliver vacuum pressure through a 1.5 liter canister and 9 feet of tubing in addition to the aspiration catheter. Nevertheless, the safety and feasibility of MAT specifically using a syringe has been less often explored. In this report, we present in vitro and clinical results of MAT with a syringe.
Methods
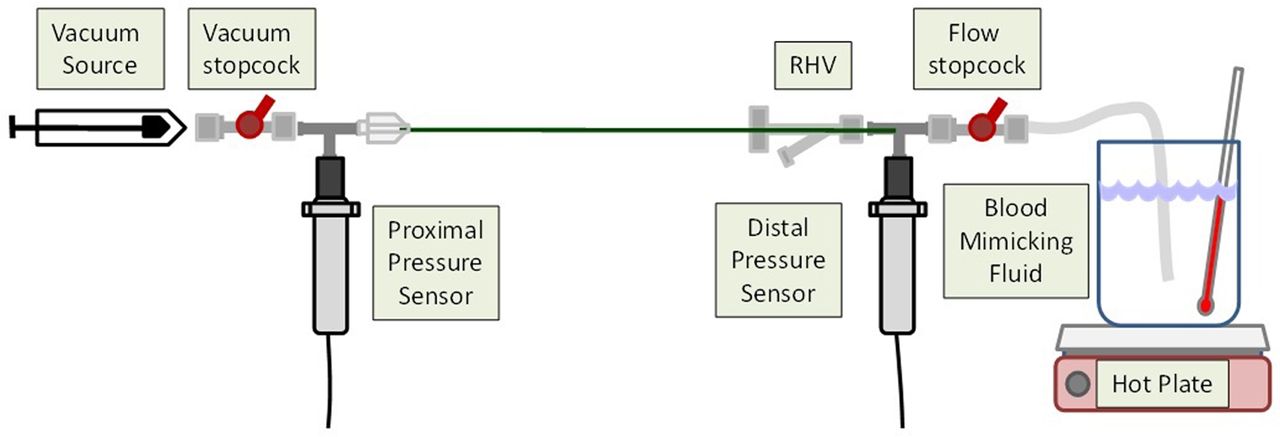
For the in vitro analysis, using the apparatus depicted in figure 1, a 0.069 inch aspiration catheter was immersed in blood-mimicking fluid, comprising 60% water, 40% glycerol, and 0.2% soap, and a vacuum source was initially used to pull fluid through the system until all air was removed. The flow stopcock was then positioned for the flow condition to be tested (partially closed for partial flow to mimic partial clot engagement or completely closed for no flow to mimic complete clot engagement). A 60 cc syringe or a Penumbra aspiration pump was then attached. For syringe aspiration, maximal initial pressure was immediately applied and the plunger was locked into place. For pump aspiration, the pump was turned on to the maximum vacuum setting for one evaluation and was also evaluated at a recommended setting of 20 inHg on the pump analog pressure gauge. Pressure recordings were recorded in pounds per square inch (psi) at a rate of 10 pressure measurements per second, taken over 2 min or until the syringe was completely filled, at which time the vacuum stopcock was closed and recording ceased.

In vitro apparatus. RHV, rotating hemostatic valve.
Clinical data were acquired from a prospectively maintained stroke database from January 1, 2017 through June 27, 2017. This database contains prospective procedural and outcome data for the four interventionalist authors at two of the three adult hospitals where they perform acute stroke intervention. Patient age, presenting National Institute of Health Stroke Scale (NIHSS) score, clot location, procedural time, angiographic result, complications, and clinical results were pooled. Consistent with our previous description,2 MAT was performed using a syringe and one of multiple aspiration catheters. Access was achieved with a Neuronmax catheter; in elderly patients or those with expected tortuosity, the Neuronmax is often bolstered with an 8F 65 cm arrow sheath. The Neuronmax is advanced over a VTK catheter into the internal carotid artery. For tortuous anatomy, two exchange-length 0.018 inch microwires can be used in place of a glidewire through the VTK to facilitate advancement of the Neuronmax into the carotid artery. The VTK can also be exchanged over these wires for an intermediate catheter that can be advanced into the internal carotid artery. An Amplatz superstiff wire can then be advanced to the tip of the intermediate catheter to facilitate advancement of the Neuronmax into the internal carotid artery.
Via the Neuronmax in the parent artery, one of five 0.060 to 0.072 inch aspiration catheters is advanced over a 3F or 3.2F microcatheter to engage the clot. More distal occlusions are approached with 0.041 or 0.044 inch aspiration catheters. The microcatheter is removed and direct aspiration is applied to the aspiration catheter with a syringe as it is removed. This technique specifically involves swift withdrawal of the syringe plunger to full aspiration, rather than gradual withdrawal. In cases where two or three passes of MAT alone prove ineffective, the microcatheter is subsequently used to deploy a stentriever. The reperfusion catheter is then advanced over the stentriever, and the device is removed. Next, aspiration is applied to the aspiration catheter with a syringe as it is removed. This stent-assisted MAT is referred to as SMAT.13
Results
In vitro analysis
Under static (no flow) conditions, a 60 cc syringe generated a vacuum pressure of 13.8 psi at the source of aspiration, delivering a vacuum pressure of 13.4 psi to the distal tip of the aspiration catheter. The Penumbra pump on its maximum vacuum setting (26.7 inHg) generated a vacuum pressure of 13.1 psi and a pressure at the distal tip of 13.0 psi; at its recommended setting (20 inHg), it generated a lower vacuum pressure of 9.6 psi at the proximal pressure sensor and 9.2 psi at the distal pressure sensor (figure 2A).

{kind=link}
{kind=link}
Comparison of vacuum pressure between syringe and pump aspiration in static (A) and partial flow (B) conditions.
Under partial flow conditions (flow rate 1 mL/s), the 60 cc syringe generated a peak vacuum pressure of 13.6 psi and a mean vacuum pressure of 13.2 psi during the first 30 s of flow. This delivered a peak pressure of 12.4 psi to the distal tip of the catheter and a mean pressure of 12.0 psi during the first 30 s of flow. Surprisingly, the syringe maintained the same degree of suction force up until the entire syringe was filled with fluid, which was consistently >60 s. The Penumbra pump on its maximum vacuum setting generated a peak pressure of 12.4 psi and a mean vacuum pressure of 12.1 psi during the first 30 s of flow. This delivered a peak pressure of 11.5 psi to the distal tip of the catheter and a mean vacuum pressure of 11.1 psi at the tip. At its recommended setting, the pump generated a peak pressure of 9.0 psi and a mean pressure of 8.7 psi during the first 30 s of flow. This delivered a peak pressure of 8.3 psi to the distal tip and a mean vacuum pressure of 7.9 psi (figure 2B).
Clinical series
Over a 6-month period, we performed 113 acute stroke thrombectomies at two of three hospitals. In seven cases, as a result of involvement in a trial or operator decision to use a mechanical device initially for a distal occlusion, MAT was not performed on the first pass and these cases were excluded from the analysis. For the remaining 106 cases performed using MAT on the first pass, mean patient age was 71 (SD 15), and 35 patients were at least 80 years old (33%). Mean NIHSS score at the time of treatment was 17 (SD 6), and 35 patients received tissue plasminogen activator before thrombectomy (33%). Twenty-five patients underwent thrombectomy more than 6 hours after symptom onset (24%). Initial clot location was most commonly within the M1 (46%); in the remaining cases, initial clot location was within the intracranial internal carotid artery (27%), M2/3 (18%), and basilar artery/proximal P1 (8%). In 24 cases, initial passes via MAT alone did not lead to adequate recanalization and thus a stentriever was used adjunctively to perform the SMAT technique (23%). The rate of Thrombolysis in Cerebral Infarction (TICI) 2b/3 recanalization was 93%. Median puncture to recanalization time was 25 min (mean 35 min, SD 25). Complications included five cases of postprocedural symptomatic intracranial hemorrhage. Three cases of vessel perforation occurred, one as a result of dissection and two as a result of perforation of an M2 or M3 branch by the wire in attempting to aspirate distal emboli after an initial pass at a more proximal occlusion. There were two cases of catheter fracture necessitating retrieval, which was successful in both cases. Mean change in NIHSS score at 24 hours was an improvement of 5.1 (SD 7.9; median 6). The in-hospital mortality rate was 10%. Seventy-four patients (70%) were discharged to home (modified Rankin Scale (mRS) score 0–2) or a rehabilitation facility (mRS 2–4; 70%).
Discussion
Professor Chapot and colleagues were the first to describe thromboaspiration as applied to intracranial clot formation in 2002. In their presentation of two cases, 4F and 5F catheters were advanced over 0.035-inch guidewires into the basilar artery, and aspiration was subsequently applied using 50 cc syringes to remove thrombus.1 With dedicated intermediate catheters, MAT evolved considerably in 2010–2012,2–4 and with ongoing dedicated aspiration catheter development and now with a randomized control trial showing equivalence to stentriever thrombectomy,12 MAT is often the first-line approach for stroke.9–11
Avoiding the use of a stentriever in 77% of cases, MAT is a cost- and time-efficient approach.2 9–11 In our series, the median reperfusion time was 25 min. At our institution, pump tubing costs $350 per case and a new canister for the aspiration pump costs $200. In comparison, a syringe costs less than $1, translating to saving nearly $550 for each case or $58 300 for the 106 thrombectomies performed.
To achieve both time- and cost-efficiency, direct aspiration with a syringe should be favored over a pump system, assuming equal or better clinical efficacy. In this study, under static, no-flow in vitro conditions, a 60 cc syringe performed very similarly to the Penumbra pump at its maximal setting. The syringe achieved slightly higher vacuum pressures, possibly because the pump must deliver vacuum pressure through a 1500 cc canister and 9 feet of silicone tubing where some pressure might be lost. A syringe, on the other hand, delivers vacuum pressure directly to the catheter. As clot is rarely aspirated through the catheter but rather is ‘corked’ at the tip, the catheter becomes a ‘suction grasper’ and a syringe can maintain vacuum force indefinitely. It is important to underscore the technique of swift, maximal aspiration force applied to the syringe (as opposed to a gradual withdrawal of the plunger), which is maintained during removal of the aspiration catheter.
Even in circumstances of subocclusive ‘corking,’ our data show that the syringe can maintain a similar or better force than an aspiration pump for at least 30 s, a more than adequate time period for catheter and clot removal (figure 2B). Froehler recently noted similar results, with the Penumbra pump having slightly weaker vacuum pressure than a 60 cc syringe in an in vitro study.14 Our study differs from this prior study in our usage of blood-mimicking fluid instead of water, evaluation of the pump at both recommended and maximal settings, and the pressure measurements performed both proximally and distally along the aspiration catheter.
Our clinical results are markedly similar to a recent series describing MAT using an aspiration pump.10 In that series of 191 cases, mean time to recanalization was 37 min, TICI 2b/3 recanalization was achieved in 94% of cases, and in 23% of cases, adjunctive usage of a stentriever was necessary. Given these similar results, it is difficult to clinically justify the added cost and potential time introduced by using an added pump system and added tubing.
While a direct, randomized comparison of a syringe with pump aspiration would more definitively prove its equivalence or superiority, the results from this analysis are noteworthy as are the markedly comparable results between our series and multiple others using a pump.9–11 It is practical to expect clinical results to remain quite similar while cost and potentially even reperfusion times remain superior for syringe aspiration.
Conclusion
This study provides in vitro and clinical analyses demonstrating the efficacy of traditional MAT with a syringe. Manual aspiration with a syringe provides equal, if not better, aspiration force and angiographic results than an aspiration pump, underscoring its efficacy. Time efficiency is intuitive as a single operator can swiftly attach an inexpensive syringe to the catheter rather than requiring an additional assistant to operate the pump and attach the tubing. Use of tubing also adds unnecessary cost to the procedure.
References
Footnotes
Contributors Drafting the article: BAG. Acquisition of data/data analysis: BTJ, BAG. Reviewed and revised article before submission: all authors. Study supervision: BTJ.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests BTJ is a consultant for Medtronic. TGJ is a consultant for Neuravi, Codman Neurovascular, Stryker (PI DAWN; unpaid), Fundacio Ictus (PIREVASCAT; unpaid) and holds stock in Anaconda, Silk Road, Blockade.
Ethics approval Pittsburgh IRB.
Provenance and peer review Not commissioned; externally peer reviewed.