Article Text

Abstract
Background Neurointerventional surgeries (NIS) benefit from supportive endovascular constructs. Sofia is a soft-tipped, flexible, braided single lumen intermediate catheter designed for NIS. Sofia advancement from the cervical to the intracranial circulation without a luminal guidewire or microcatheter construct has not been described.
Objective To evaluate the efficacy and safety of the new Sofia Non-wire Advancement techniKE (SNAKE) for advancement of the Sofia into the cerebral circulation.
Methods Consecutive patients who underwent NIS using Sofia were identified. Patient information, SNAKE use, and patient outcome were determined from electronic medical records. Sofia advancement to the cavernous internal carotid artery or the V2/V3 segment junction of the vertebral artery was the primary outcome measure. Secondary outcomes included arterial vasospasm and arterial dissection.
Results 263 Patients (181 females, 69%) who underwent a total of 305 NIS using Sofia were identified. SNAKE (SNAKE+) was used in 187 procedures (61%). Two hundred and ninety-three procedures (96%) were technically successful, which included 184 SNAKE+ NIS and 109 SNAKE− NIS. Primary outcome was achieved in all SNAKE+ procedures, but not in five SNAKE− procedures (2%). No arterial dissections were identified among 305 interventions. In the intracranial circulation, a single SNAKE+ patient (0.5%) had non-flow limiting arterial vasospasm involving the petrous internal carotid. Three SNAKE+ patients (1.6%) and one SNAKE− patient (0.8%) demonstrated external carotid artery branch artery vasospasm during dural arteriovenous fistula or facial arteriovenous malformation treatment.
Conclusion SNAKE is a safe and effective technique for Sofia advancement. Sofia is a highly effective and safe intermediate catheter for a variety of NIS.
- sofia
- safety
- intermediate catheter
- stroke
- aneurysm
- AVM
- dural arteriovenous fistula
Statistics from Altmetric.com
Introduction
Neurointerventional surgeries (NIS) treat a wide range of cerebrovascular pathology that includes cerebral aneurysms, arteriovenous malformations, dural arteriovenous fistulae, ischemic stroke, and intracranial atherosclerotic disease among other pathologies. Intermediate catheters provide additional support to endovascular constructs to facilitate NIS.1–5 While some have found that intermediate catheters increase the safety of NIS,3 others have found similar complication rates between NIS performed with and without intermediate catheters.2
A variety of methods are used to advance intermediate catheters into the proximal cerebral circulation. For example, an intermediate catheter may be advanced over a guidewire or over a microcatheter construct, both of which require equipment introduction through the intermediate catheter. Placement of equipment into an intermediate catheter has greater potential for complications, either by introducing air into the endovascular construct or thrombus formation within the lumen of the intermediate catheter, by decreasing luminal dead space.
Here we describe the Sofia Non-wire Advancement techniKE (SNAKE), a new technique by which the soft-tipped Sofia intermediate catheter (MicroVention, Tustin, California, USA) is introduced into the intracranial circulation without the assistance of a guidewire or microcatheter construct within the Sofia lumen. The safety and efficacy of SNAKE is evaluated relative to conventional means of advancing the Sofia over a guidewire or microcatheter construct.
Materials and methods
Patient identification and inclusion
Our hospital’s Institutional review board approved this study, which complied with the Health Insurance Portability and Accountability Act. We retrospectively identified all patients who underwent a NIS using the 5-French Sofia or 6-French Sofia Plus intermediate catheter (MicroVention, Tustin, California, USA) between January 1, 2014 and April 1, 2017 at our neurovascular referral center from a prospectively collected neurointerventional database. Patient data were obtained from the electronic medical record.
Procedural technique
All procedures were performed using a Siemens Artis Zee biplane system in a dedicated neuroangiography suite. Procedures were performed under monitored anesthesia care or general anesthesia. Neurophysiologic monitoring was used for all procedures except for tumor embolizations and stroke interventions.
Neurointerventional procedures were performed after catheterizing the common femoral artery with a 6-French shuttle SL sheath (Cook Medical, Bloomington, Indiana, USA) or an 8-French Brite Tip sheath (Cordis, Milpitas, California, USA). Intravenous heparin was administered to achieve an activated clotting time of 250–300 s after arterial access was obtained. Cerebral digital subtraction angiography (DSA) was performed with a 5-French Berenstein II catheter (Cook Medical, Bloomington, Indiana, USA) positioned in the common carotid artery, internal carotid artery (ICA) or the vertebral artery. The Berenstein catheter was then replaced with a 5- or 6-French Sofia catheter, which was advanced into the supraclinoid ICA, M1 segment of the middle cerebral artery, V4 segment of the vertebral artery, or basilar artery for the subsequent NIS. All sheaths, Berenstein catheters, Sofia catheters, and microcatheters were connected to a continuous heparinized saline flush with a Tuohy Borst adapator.
Sofia Non-wire Advancement techniKE (SNAKE)
There are four neurointerventionalists in our practice, which includes two physicians who used SNAKE in every procedure during the time period evaluation and two physicians who did not use SNAKE. The distal end of the Sofia catheter is extremely soft and pliable, which led us to test whether the Sofia could be safely advanced into the cerebral circulation without a guiding wire, microcatheter, or microcatheter and microwire construct within it (SNAKE). SNAKE was performed by introducing the 5-French Sofia or 6-French Sofia Plus into the shuttle sheath positioned in the distal common carotid artery, proximal cervical ICA, subclavian artery, or V1 segment of the vertebral artery. Under continuous roadmap guidance, the Sofia was then advanced through the shuttle into the ICA or vertebral artery with no additional equipment within the Sofia lumen. Sofia advancement using SNAKE was stopped when moderate buckling of the Sofia was observed or any significant resistance was felt by the neurointerventionalist. If more distal navigation of the Sofia was necessary, the SNAKE was terminated and a microcatheter and microwire were then introduced into the Sofia and advanced more distally. The Sofia was then navigated over the microwire and microcatheter to the desired position in the intracranial circulation.
Imaging and outcome analysis
All DSA images from NIS in the study were reviewed by two neurointerventional radiologists with 4 and 20 years of experience. The primary outcome measure was defined as successful advancement of Sofia to at least the posterior genu of the cavernous ICA in the anterior circulation or to at least the V2/V3 segment junction of the vertebral artery in the posterior circulation. The secondary outcome measure was complications that included angiographic evidence of arterial dissection or vasospasm following Sofia introduction. The procedure reports for all studies were reviewed for mention of dissection or vasospasm. The reports were also reviewed for the use of intraprocedural nitroglycerin, which was considered a proxy for non-imaged vasospasm.
Statistical analysis
Statistical analysis was performed using XLSTAT (Addinsoft, New York, USA). Χ2 Analysis was used for discontinuous variables, and Student’s t test for continuous variables. The expected procedural success rate was 95% for the effectiveness analysis. A p value of 0.05 was considered statistically significant.
Results
Two hundred and sixty-three patients (181 females, 69%) who underwent a total of 305 interventions using the Sofia catheter were identified within the study period. Mean patient age was 59 years (IQR 47–74). Cerebral aneurysm embolization (92 procedures, 30%), acute stroke intervention (80 procedures, 26%), and cerebral arteriovenous malformation embolization (44 procedures, 14%) were the most commonly performed interventions (table 1). The 5-French Sofia was used for the majority of procedures (219 procedures, 72%) compared with the 6-French Sofia (86 procedures, 28%) (table 1). However, the 6-French Sofia (69 procedures, 75%) was more commonly used for cerebral aneurysm treatment, which was frequently performed using a balloon microcatheter (30 procedures; 33%) or stent (12 procedures, 13%) assistance.
Sofia SNAKE and complications
SNAKE was used in 186 procedures (SNAKE+ group), which included 148 procedures with the 5-French Sofia (79%) and 38 procedures with the 6-French Sofia Plus (20%). By contrast, conventional Sofia advancement with a guidewire or microcatheter construct (SNAKE− group) was used in 119 patients, which included 71 procedures with the 5-French Sofia (60%) and 48 procedures with the 6-French Sofia Plus (40%). Ischemic stroke treatment (50 procedures), cerebral aneurysm embolization (43 procedures), and cerebral AVM embolization (35 procedures) were the most commonly performed NIS that used SNAKE (table 1). The slight differences in NIS performed between the SNAKE+ and SNAKE− groups reflected variations in physician practice pattern rather than a preference for SNAKE when treating certain types of pathology.
Two hundred and ninety-three procedures (96%) in this study were technically successful, which included 109 procedures in the SNAKE− group (92%) and 184 procedures in the SNAKE+ group (98%). In the anterior circulation, SNAKE was used to advance the Sofia to at least the posterior genu of the cavernous ICA (figures 1 and 2 and online supplementary videos 1 and 2) and as distal as the M1 segment of the ICA in all NIS. In the posterior circulation, SNAKE advanced the Sofia to at least the distal V2 segment of the vertebral artery and as distal as the basilar artery (figure 3 and online supplementary video 3) in all NIS. SNAKE was used to advance Sofia through 360 degree loops in the cervical common carotid artery and ICA without difficulty (online supplementary video 2). In the SNAKE− group, Sofia could not be advanced to at least the posterior genu of the cavernous ICA in four patients and to the V2/V3 junction in one patient owing to excessive vascular tortuosity. A stable endovascular construct that could safely facilitate embolization could not be established in these five SNAKE− procedures, which were all aborted. Four procedures in the SNAKE− group and three in the SNAKE+ group were aborted owing to unfavorable anatomy for endovascular aneurysm embolization or lack of a suitable embolization target. Although SNAKE was more likely to be associated with procedural success (p=0.02), this difference most likely reflects patient anatomic differences rather than the use of this technique.

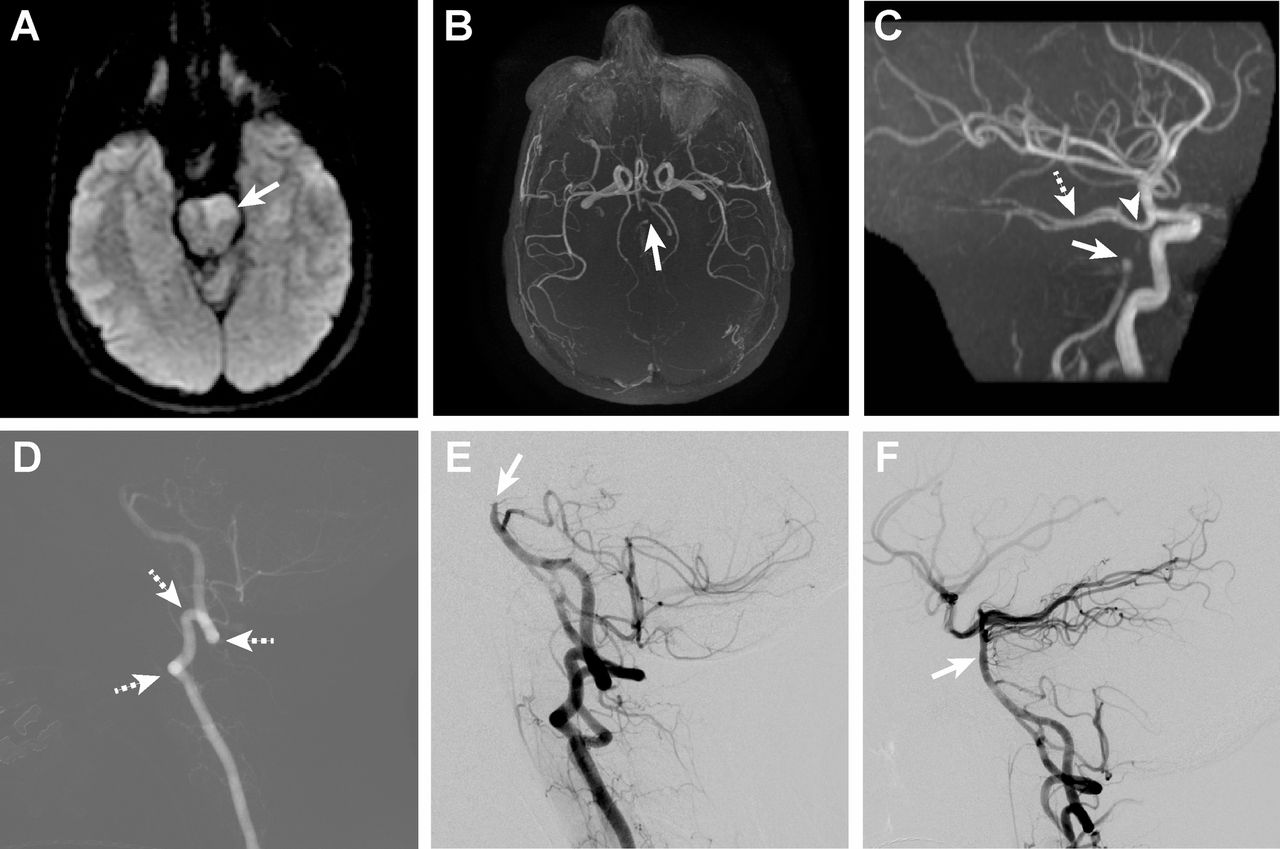
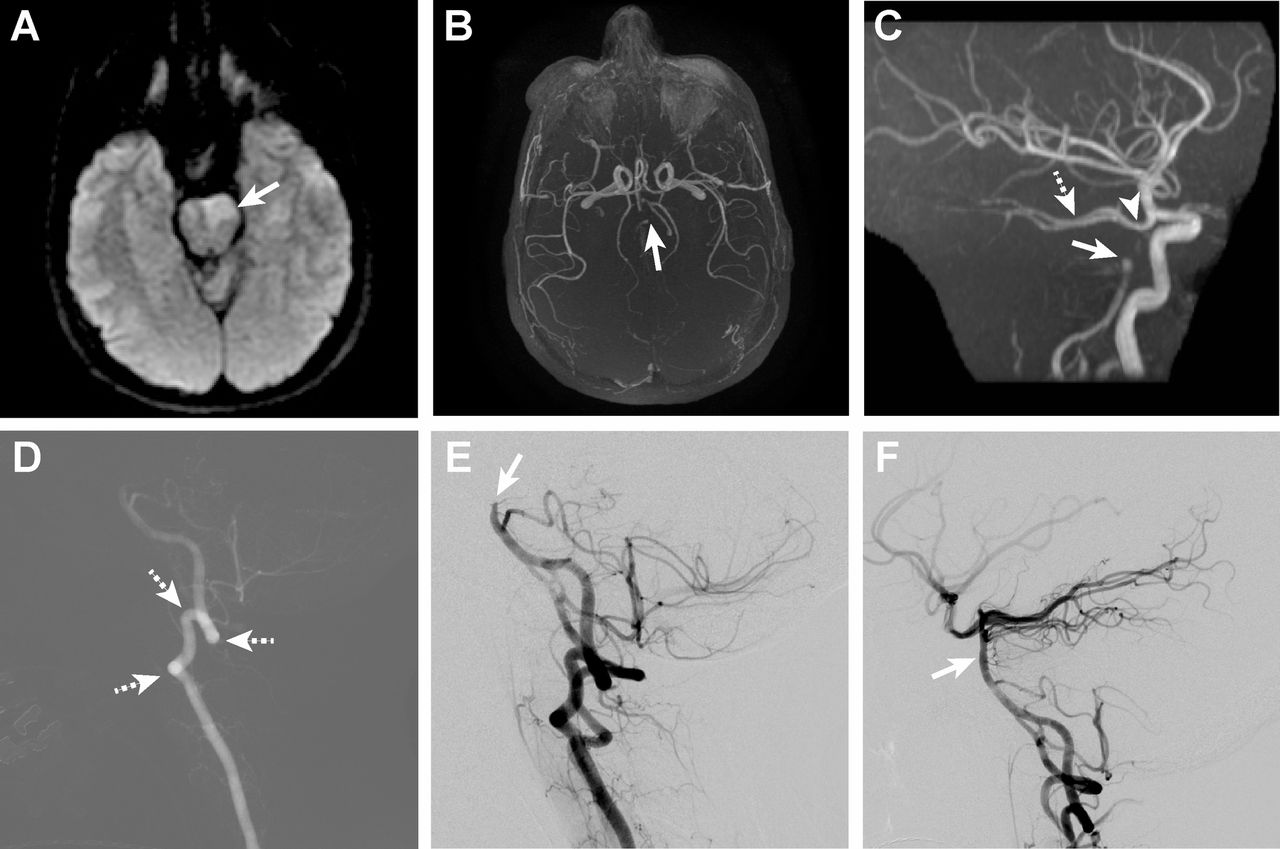
Elderly patient with an acute ischemic stroke due to occlusion of the M1 segment of the left middle cerebral artery (MCA). (A) Diffusion-weighted imaging shows a small acute infarction in the left caudate and lentiform nucleus (arrow). (B) Axial maximum intensity projection image from MR angiography shows occlusion of the M1 segment of the left MCA (arrow). (C) Perfusion-weighted imaging identifies a large penumbra (arrow) on the time-to-maximum maps. (D) Lateral roadmap image following injection of the left common carotid artery demonstrates multiple acute turns within the left internal carotid artery (ICA; dashed arrows). This vessel was traversed with a 5-French Sofia using SNAKE (see online supplementary video 1). (E) Anteroposterior view after left ICA injection demonstrates occlusion of the M1 segment of the left MCA (arrow). (F) Complete reperfusion of the left MCA (arrow) is present after combined suction and mechanical thrombectomy.

Elderly patient with subarachnoid hemorrhage due to rupture of a recurrent left posterior communicating artery aneurysm after prior coil embolization. The aneurysm was re-treated by balloon-assisted coiling. (A) Non-contrast head CT shows diffuse subarachnoid hemorrhage (SAH) throughout the basal cisterns (arrow). (B) Roadmap image following injection of the left common carotid artery demonstrates a 360 degree loop in the proximal common carotid artery (arrow). This vessel was traversed with a 6-French Sofia Plus using SNAKE (see online supplementary video 2). (C) Lateral DSA image following injection of the cervical left internal carotid artery demonstrates a broad-based posterior communicating artery aneurysm (arrow) that is the cause of the patient’s SAH. (D) The posterior communicating artery aneurysm no longer fills following balloon-assisted coil embolization (arrow).
{kind=link}
{kind=link}
{kind=link}
Young patient with an acute ischemic stroke due to occlusion of the mid-basilar artery. (A) Diffusion-weighted imaging shows acute infarction in the left pons (arrow). (B) Axial maximum intensity projection image from MR angiography (MRA) shows minimal flow-related signal within the basilar artery (arrow). (C) Reconstructed MRA image in the lateral project demonstrates occlusion of the mid-basilar artery (arrow). The patient has widely patient posterior communicating arteries (arrowhead) that supply the posterior cerebral arteries (dashed arrow). (D) Lateral roadmap image following injection of the left vertebral artery demonstrates multiple acute turns within this vessel (dashed arrows). This vessel was traversed with a 5-French Sofia using SNAKE (see online supplementary video 3). (E) Lateral view after left vertebral artery injection demonstrates occlusion of the mid-basilar artery (arrow). (F) Complete reperfusion of the basilar artery (arrow) is present after combined suction and mechanical thrombectomy.
Complications related to Sofia and SNAKE use were extremely uncommon. No arterial dissections were identified among 305 interventions. Non-flow limiting arterial vasospasm involving the petrous ICA secondary to a 6-French Sofia was identified in a single SNAKE+ patient, and no other Sofia related vasospasm instances were identified in the anterior or posterior circulations in either group (table 2). One SNAKE− patient and three SNAKE+ patients demonstrated external carotid artery branch artery vasospasm after placement of a 5-French Sofia for treatment of dural arteriovenous fistula or facial arteriovenous malformations. None of the instances of vasospasm was symptomatic, procedurally significant, or clinically significant. There was no significant difference in the complication rate between the SNAKE− and SNAKE+ groups (p=0.5).
Complications due to sofia and SNAKE
Discussion
Cerebrovascular diseases, such as aneurysms, AVMs, ischemic stroke, and dural arteriovenous fistulae, are increasingly treated by endovascular approaches.6 The technological advancements in guide catheters, intermediate catheters, microcatheters, and other neurointerventional equipment contribute to the ability to treat these complex lesions. Intermediate catheters have emerged as an important technological advance that facilitate more efficient treatment of cerebrovascular disease.2 They provide flexibility to the neurointeventionalist, who can adapt the stability, support, and length of the endovascular construct to his or her needs.1–3 In addition, intermediate catheters may reduce procedure time and likely reduce the risk of arterial dissection given the ability to re-access the cerebral circulation by traversing fewer vascular segments multiple times and improving the stability of support of the endovascular construct.3 Despite these purported advantages of intermediate catheters, NIS complication rates are similar to historical procedures without intermediate catheters.2
The Sofia (Soft torqueable catheter Optimized For Intracranial Access; MicroVention, Tustin, California, USA) is an intermediate catheter approved for intracranial use. It has an extremely soft distal tip and has been shown to be an effective tool for ischemic stroke treatment and stent-assisted aneurysm coiling,4 7–10 although its effectiveness for other NIS has not been reported.
Early in our experience with Sofia, we discovered that Sofia’s soft distal tip allowed this intermediate catheter to be advanced into the intracranial circulation without a guidewire, microcatheter, or other luminal device (SNAKE). In this study, we describe SNAKE as an effective and safe technique for Sofia advancement during NIS. In addition, this study is the largest series to evaluate the technical success and complication rates related to the Sofia intermediate catheter across a variety of NIS.
SNAKE was rapid and highly effective in introducing both the 5-French and 6-French Sofia into the intracranial circulation. The Sofia was advanced to the posterior genu of the cavernous ICA or the V3 segment of the vertebral artery without any resistance or difficulty in all cases. In one stroke intervention, the Sofia was advanced using SNAKE to a clot interface in the M1 segment of the middle cerebral artery, which facilitated rapid revascularization in this patient.
The main advantage of SNAKE is more rapid access to the intracranial circulation without having to introduce a guidewire or microcatheter construct. Routinely in our practice, one operator advances the Sofia into the intracranial circulation using SNAKE, while a second operator prepares the microcatheter and microwire for the planned NIS on the back table. Thus, SNAKE allows the procedure to proceed efficiently, which provides benefit to all NIS in the reduction of in-dwelling catheter times and in particular, for stroke interventions. We did not compare procedure times between the SNAKE− and SNAKE+ groups because our non-randomized study design, but a future study might assess time as an outcome measure.
A second potential advantage of SNAKE is a reduction in the distance of intracranial artery that must be traversed by a microcatheter and microwire, which may reduce the risk of arterial dissection and vasospasm.
A third advantage of SNAKE is a possible reduction in the number of times equipment is introduced into the Sofia. Guidewire and microcatheter placement within an intermediate catheter introduces the possibility of air entering the closed system. Furthermore, equipment placement within an intermediate catheter increases the likelihood of thrombus formation within the construct due to increased foreign material surface area that may contact blood, blood stasis within the intermediate catheter due to interruption of heparinized saline flush, and reduced luminal dead space. Although SNAKE does not reduce these variables throughout the duration of the procedure, it does minimize the risk of one step of the procedure, which may increase the safety of the procedure.
Lastly, our results raise the possibility of reduced equipment costs in NIS if the need for guidewires, microcatheters, and/or microwires can be eliminated. Although most procedures will still require these pieces of equipment, one can imagine how a stroke intervention performed using an aspiration thrombectomy approach might not require this equipment if Sofia can be advanced to the thrombus interface using SNAKE.
Sofia was a highly effective as an intermediate catheter in our study, and 96% of the 305 NIS were technically successful. Sofia performed well in both the SNAKE− and SNAKE+ groups, and the minor differences in procedural success between these groups reflected patient anatomic variations rather than technical differences in the procedure. Sofia was successfully navigated through significant vascular tortuosity and into the desired position in the intracranial circulation in all but five procedures. It is difficult to compare the effectiveness of Sofia with prior studies of intermediate catheters because technical success was either not described or was described for stroke interventions only.1–4 8 9 11 12 However, we have found that Sofia’s trackability into the intracranial circulation is excellent, and the technical success of this study compares favorably with prior studies of Sofia for stroke intervention.4 12
Both Sofia and SNAKE had an excellent safety profile, and no instances of arterial dissection, flow limiting vasospasm, or other complications were seen in our study. This safety profile is superior to older generation intermediate catheters.2 The external carotid artery braches were more prone to vasospasm than the vasculature of the anterior and posterior circulations (four patients versus one patient), which likely reflects the anecdotal propensity of the external carotid artery branches for vasospasm during angiography.
Sofia intermediate catheters have a couple of disadvantages. First, although the softness of the distal tip allows for SNAKE, it is less supportive than stiffer intermediate catheters. This slight decrease in support results in a need for more frequent relaxation and addition of tension in the endovascular construct. While the authors of this study have become accustomed to interacting more with Sofia relative to other intermediate catheters to adjust for this difference, others may find this property is a limitation in their practice. Next, the slightly larger outer diameter of the 6-French Sofia (0.0825 in) may lead to incompatibility with some endovascular constructs, particularly those used for ischemic stroke treatment. We routinely placed the 6-French Sofia (Sofia Plus) through a 6-French shuttle sheath (Cook Medical) without difficulty, but neurointerventionalists should note equipment sizes to ensure endovascular construct compatibility with the larger Sofia Plus. We expect that future generations of the Sofia may deal with these shortcomings.
The study has several limitations. First, this is a non-randomized study for comparison of the SNAKE− and SNAKE+ groups, which might have introduced operator bias. This study design introduces the possibility of other variables that influence the technical success and safety outcome measures. Additionally, the size of our cohorts, self-reported results, and inclusion of patients from a single neurovascular referral center might have biased our results. These shortcomings could be overcome through a larger, randomized trial. Lastly, we describe SNAKE as a technique for advancement of the Sofia intermediate catheter. We have not applied this technique routinely to other intermediate catheters, but such a study could certainly be performed. We would advocate that the application of SNAKE to other catheters be undertaken with caution as intermediate catheters have varying degrees of softness, which may affect the risk of vessel dissection during non-wire advancement.
Conclusions
The Sofia Non-wire Advancement techniKE (SNAKE) is a safe and effective technique for Sofia advancement into the intracranial circulation. Sofia is a highly effective and safe intermediate catheter during a variety of NIS.
Supplementary video 1
Supplementary video 1
Supplementary video 2
Supplementary video 2
Supplementary video 3
Supplementary video 3
Footnotes
Contributors All authors made substantial contributions to the conception and design of the study, acquisition of data, or analysis and interpretation of data.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests JJH and HMD are consultants for MicroVention, Inc.
Ethics approval Institutional review board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Published and unpublished data may be shared for additional publications pending the authors’ agreement to a research collaboration when appropriate.