Article Text

Abstract
Innovations in interventional cardiology historically predate those in neuro-intervention. As such, studying trends in interventional cardiology can be useful in exploring avenues to optimise neuro-interventional techniques. One such cardiology innovation has been the steady conversion of arterial puncture sites from transfemoral access (TFA) to transradial access (TRA), a paradigm shift supported by safety benefits for patients. While neuro-intervention has unique anatomical challenges, the access itself is identical. As such, examining the extensive cardiology literature on the radial approach has the potential to offer valuable lessons for the neuro-interventionalist audience who may be unfamiliar with this body of work. Therefore, we present here a report, particularly for neuro-interventionalists, regarding the best practices for TRA by reviewing the relevant cardiology literature. We focused our review on the data most relevant to our audience, namely that surrounding the access itself. By reviewing the cardiology literature on metrics such as safety profiles, cost and patient satisfaction differences between TFA and TRA, as well as examining the technical nuances of the procedure and post-procedural care, we hope to give physicians treating complex cerebrovascular disease a broader data-driven understanding of TRA.
- cardiology
- neuro-intervention
- transradial access
- review
Statistics from Altmetric.com
Introduction
Due to the larger patient population and less tortuous vasculature, interventional innovations have often been developed in interventional cardiology before being adopted for neuro-intervention. As a result, studying current trends in interventional cardiology is often quite instructive for learning how to optimise our neuro-interventional techniques. One particularly interesting aspect of the interventional cardiology journey is their remarkable conversion from transfemoral access (TFA) to transradial access (TRA). Over the past decade, there have been numerous large prospective randomised controlled trials documenting a clear safety benefit of the transradial approach over transfemoral access. Furthermore, multiple individual technique permutations have also been studied in a prospective, randomised fashion. This has yielded a detailed picture of not only the argument for conversion to the transradial approach, but also an evidence-based understanding of how to optimally perform TRA.
The majority of the argument favoring transradial over transfemoral centers on access, and so we felt it prudent to review the cardiology data on the radial approach and interpret it for a neuro-interventional audience. Many neuro-interventionalists may not be comfortable with TRA and are not familiar with the cardiology literature documenting the best practices for TRA, but we believe there is a growing need for neuro-interventionalists to master TRA techniques. Therefore, we sought to perform a review in order to analyze certain relevant TRA perimeters including procedure-related metrics (patient safety, satisfaction, cost) as well as technical nuances (heparin use, anti-spasmodics, sheath size and characteristics, etc.).
Methods
Using the MeSH database system through PubMed, a literature search was completed between the years 1999 and 2017 for all articles that included the terms radial artery and cardiology or interventional radiology (ex. ‘Radial Artery’ (MeSH) AND ‘Cardiology’(MeSH); ‘Radial Artery’ (MeSH) AND ‘Radiology, Interventional’ (MeSH)). The articles were limited to English with human subjects who underwent interventional cardiac procedures. Additionally, the article types were limited to randomized controlled trials, while reviews, editorials and commentaries were excluded. The initial inclusion criteria focused on patients who underwent procedures using transradial vascular access or studies that compared transradial and transfemoral approaches. All articles that met these criteria underwent an abstract review to determine the validity of each paper. Duplicates or papers that failed to meet our study standards were discarded. The papers were then screened an additional time based on the full text, and the final studies included in this study were discerned.
A search was also conducted on other Internet databases, including a PubMed search excluding the MeSH system. Key search terms included ‘Cardiology’ and ‘Transradial Access’ or ‘Transradial AND Transfemoral Access’.
Full text review
The papers that underwent full-text screening were included if they discussed procedure-related considerations of radial access or specific technique descriptions. These interventional considerations included patient safety, patient satisfaction (ex. reduced pain, faster time to ambulation, etc.), procedure cost and appropriate patient selection. Technical nuances that were examined encompassed the use of heparin and anti-spasmolytic medications, methods for improving puncture technique, sheath size and characteristics, and haemostasis. Articles that did not discuss the aforementioned information were discarded.
A total of 28 papers were found using these literature search criteria. The last search was performed on 27 March 2017.
Results
Study selection
The initial search collectively resulted in 193 papers, of which 13 came from the MeSH PubMed search and 180 came from the additional online database search. There were 85 duplicate studies. Through title and abstract review, we narrowed the search to 88 articles, which were assessed using the previously mentioned selection criteria. Articles were included in the analysis if there was discussion of information regarding procedure-related information and interventional technique. Sixty articles were eliminated after full-text review, leaving 28 studies fitting our inclusion standards, with two of the 28 analysing multiple endpoints simultaneously (ie, patient satisfaction and cost; patient safety and satisfaction). The results of our literature screening are summarised in figure 1.

The PRISMA diagram summarises the systematic process used to identify, screen and include articles we analysed for this review.
Study characteristics
Each of the 28 papers found through our review methodology was a prospective, randomized controlled trial. Twelve studies analysed the safety of the transradial compared with the transfemoral approach using markers such as minor intra-/post-operative bleeding to major complications (myocardial infarction) or mortality. Three papers studied patient satisfaction, and found that TRA may be associated with higher quality of life, faster time to ambulation and less pain. One paper looked at costs associated with TRA, and found that radial approaches may lead to reductions in pharmacy, bed and total hospital costs. One paper discussed pertinent considerations when selecting patients for TRA.
Three papers discussed the use of administration of spasmolytic medications, such as verapamil or nitroglycerin, to combat complications of TRA-like radial artery spasm (RAS), while one paper discussed the role of heparin in preventing radial artery occlusions (RAO). Seven papers discussed technical information regarding puncture technique, optimal sheath size and vessel selection (right versus left radial artery). Finally, two papers analysed post-procedural haemostasis techniques and devices.
Discussion
There has been increased data published in the past decade on TRA in the interventional cardiology literature. The results have driven a steady conversion to the radial approach in the USA, with more than 30% of cases performed radially annually, a number that has increased 3%–4% every year of the past decade. In Europe, adoption has been even more dramatic, with a remarkable 85% of cardiology cases being done via the radial approach. Based on the compelling safety data of the TRA over TFA, three of the largest societies of interventional cardiologists in Europe issued joint guidelines in 2013 formally recommending radial access as the first choice for all cardiac procedures in Europe. We focused on two core areas of the cardiac literature that are directly transferable to neuro-intervention. The first area was the literature comparing TRA to TFA as it related to the access itself — complication rates, patient satisfaction and cost. The second area was the literature exploring the optimal technique to perform radial access.
Safety of transradial compared with transfemoral approach
Much of the interest in the cardiology literature surrounding radial access is driven by multiple large, prospective trials that have consistently demonstrated a safety benefit of the radial approach over the femoral approach. This is primarily related to reduction in access site complications. Access site complications from a femoral approach (bleeding, retroperitoneal haematoma, pseudoaneurysm and arteriovenous fistula) in the cardiology literature compare similarly to those reported in the neuro-interventional literature, occurring in between 2%–8% of procedures.1–4
Multiple prospective studies have revealed that the radial approach is associated with a significant reduction in access site complications compared with the femoral approach.5–13 A prospective, randomized study of 7000 patients comparing TRA to TFA showed an absolute risk reduction of 2.3% in major access site complications, and the MORTAL trial actually found a 17% reduction in 1-year mortality with TRA in coronary angioplasty.14 Furthermore, a recent meta-analysis of more than 7 60 000 patients showed a 78% risk reduction in bleeding patients undergoing TRA versus TFA.15
There are two reasons behind this difference in access site complications. The first relates to the space in the distal wrist being significantly smaller than that of the proximal thigh, limiting the risk of high-volume haemorrhage. Even if the patient has poor hemostasis and bleeds, there simply is not enough space to accommodate significant bleeding. Unlike the thigh or peritoneum, the soft tissue in the distal wrist is also an easily compressible location. In addition, when you remove the relatively rare but devastating complication of retroperitoneal haematoma, the rare but ever-present mortality risk just from the access alone drops to zero.
The second reason for the lower rate of complication is that unlike the common femoral artery, which is an end artery, the robust collateral circulation in the hand from the ulnar artery makes ischaemic complications extraordinarily rare. In fact, cardiac radialists no longer even confirm collateral circulation to the hand with an Allen test or Barbeau test, as it does not predict hand ischaemia. The position is that patients should not be denied a radial approach simply because of a ‘failed’ Allen test.
Complications specific to TRA include RAO and RAS. RAO occurs in less than 5% of patients with current prevention strategies (detailed below), and is almost always clinically silent due to collateral circulation from the palmar arch via the ulnar artery.5 Nonetheless, patients often need repeat angiographic procedures and thus efforts at minimising RAO rates are prudent.
RAS occurs in 6%–10% with appropriate prevention with a spasmolytic cocktail (usually a calcium channel blocker associated with nitroglycerin) through the sideport of the sheath.16 If no cocktail is administered, RAS approaches 15%–30%.
The safety argument for TRA is particularly compelling in two patient groups: those who carry a relatively high risk of complication from a transfemoral approach; and those in whom specific anatomical features lend themselves to easier catheter navigation via the right subclavian artery. Such patients include obese patients, female patients, patients with a bleeding diathesis, orally anticoagulated patients and the elderly.17–19 A multicentre study of more than 500 obese patients (Body Mass Index 35 or greater) compared TRA to TFA and found significantly decreased access site complications, length of hospital stay and procedure time in patients undergoing TRA versus TFA.20
Individual patient anatomy is an important factor in selecting the TRA technique as well. Patients with distal aortic or common femoral pathology may be precluded from a TFA and require alternative vascular access. Alternatively, many patients are ideal candidates for TRA due to favourable arch anatomy. A study of TRA in carotid stenting in patients with bovine and Type III aortic arches found a 100% procedural success and no major cardiac, cerebrovascular or access site complications.21
Patient satisfaction
We found several studies that compared preference for TRA versus TFA from a patient’s perspective. A prospective randomized trial of 200 patients comparing TRA to TFA found a significant association between the radial approach and lower rates of overall discomfort, back pain and difficulty walking.22 In 2006, a large multicentre trial randomized 7021 patients to TRA versus TFA for coronary interventions. The study showed that 90% of patients who underwent TRA and 50% who underwent TFA said they would prefer TRA for their next procedure.23 Of patients who had undergone both TRA and TFA previously, 75% preferred a radial approach for their next procedure.24 The principal reason for this seems to be the increased sensitivity of the inguinal region compared with the wrist. In addition, because patients can ambulate immediately after the procedure and the observation period is significantly shorter (90 min in our centre for diagnostic angiography), the overall patient experience is much improved.25 26
Cost
Technical improvements are often associated with higher costs, but in the case of the radial approach, it has been shown to actually lower costs. A cost-benefit analysis of 14 randomized controlled trials found a $275 decrease in hospital costs in patients undergoing TRA compared with TFA.24 These cost savings were attributed to a significant reduction in access site complications associated with TRA. However, there are several other areas where cost savings occur. A prospective trial of 152 patients that randomized patients undergoing coronary angioplasty to TRA versus TFA, found reduced hospital charges, shorter length of post-procedure monitoring and total hospital stay with TRA.27
Nursing workload has been shown to be reduced with TRA when compared with TFA. A trial of 260 consecutive patients found a 50% reduction in workload for nurses, both in the angiography suite and in the recovery ward.28 These reductions were attributed to a decrease in time of recovery, a simplification of nursing tasks in the angiography suite and in the recovery area, and a decrease in hospital stays and ICU admissions due to reduced access site complications.
Technical nuances
With the clear benefit of the radial approach over femoral, the cardiology literature has gone even further, performing multiple prospective trials comparing different techniques of the radial approach to scientifically validate how to optimally perform the access itself. For the neuro-interventional audience, studying the results of these technique trials prevents us from re-creating the wheel in our patients. The use of these techniques not only reduces complications and the likelihood of crossover to transfemoral access, but also reduces the ‘learning curve’ associated with TRA proficiency. What emerges is an evidence-based understanding of how to optimally perform radial access.
Preprocedure assessment of collateral circulation
Significant controversy in the literature exists regarding the need for preprocedure collateral circulation testing, via Allen’s test (AT) or Barbeau test, and the need for subsequent exclusion from the radial approach for patients who fail such testing.17 29 The RADAR trial found no evidence of hand ischaemia in patients undergoing TRA, even in patients with abnormal AT results. The study concluded that AT and oximetry-plethysmography (OP) results did not correlate with hand strength, post-procedure arm discomfort or hand ischaemia. An associated editorial stated that patients should not be denied TRA based on abnormal AT or OP.29 30 Furthermore, reports of hand ischaemia following TRA are remarkably few despite the dramatic increase in TRA procedures performed worldwide, and of those cases reported, none had demonstrated inadequate collateral circulation. Most research into hand ischaemia is in the setting of invasive transradial arterial pressure monitoring in the critical care literature, and reports of hand ischaemia do not correlate with evidence of inadequate collateral circulation on pre-procedure testing.31 32 These findings support a robust and dynamic collateral circulation present in all patients regardless of pre-procedure testing results. Experts currently recommend that transradial access should not be avoided because of abnormal Allen’s test results, and, in fact, there has been a call to stop performing this test.
Use of heparin
Intraprocedural administration of unfractionated heparin at therapeutic levels (50 U/kg or 5000U) has been shown to significantly reduce the incidence of radial artery occlusion without increasing access site complications.33–35 A prospective trial of more than 400 patients found a 4.3% RAO rate when 5000U of unfractionated heparin was administered, compared with 24% when 2000–3000U was given and 71% when no heparin was administered.33 Heparin can be either given intravenously or intra-arterially through the sheath. A prospective randomized trial of 500 patients found no difference in RAO rates between intravenous versus intra-arterial administration.34 From our institution experience, we favour administration of unfractionated heparin at a dose of 70 U/kg intravenously after vascular access has been established.
Use of anti-spasmodic and vasodilatory medications
Intra-arterial anti-spasmodic medications are routinely used to prevent spasm, though no consensus currently exists on the combination, dose or timing of drugs to be administered. Rosencher et al randomized 731 patients to verapamil, diltiazem or isosorbide dinitrate after TRA had been established. The use of verapamil was associated with a 3% risk reduction in RAS and less pain post procedure.36 Keimeneij et al found a 14% reduction in radial artery spasm (RAS) when 5 mg of verapamil and 200mcg of nitroglycerin were used intra-arterially when compared with placebo in a study of 100 patients.37 Chen et al similarly found a 16% reduction in RAS with the use of nitroglycerin and verapamil in a study of 406 patients.38 Most convincingly, a pooled analysis of 22 randomized studies revealed the lowest rates of RAS occurred with the administration of verapamil 5 mg andnitroglycerin.39 Prior to administration of heparin and prior to introducing the guidewire catheter, we injected 2.5 mg of verapamil and 200 µg of nitroglycerin at our institution. These agents were diluted in 20 ml of blood aspirated from the sheath to prevent discomfort during the injection.
The use of topical or subcutaneous medications prior to establishing TRA has also been evaluated. Beyer et al evaluated radial artery diameter pre- and post-procedure in 86 patients randomized to topical lidocaine and nitroglycerin versus placebo.40 They found a 16.5% increase in radial artery diameter with the use of topical medications. Multiple similar prospective studies found the use of subcutaneous nitroglycerin to be associated with increased radial artery diameter and improved time to achieve access.41–44
Puncture technique
Several studies have been conducted to assess the fastest and safest way to perform the puncture itself. Pancholy et al conducted a prospective randomized trial comparing the counterpuncture technique to the anterior puncture technique (figure 2).45 The counterpuncture technique has proven to be superior compared with the anterior puncture technique with fewer attempts needed to achieve access and reduced access and procedure times, with similarly low complication and RAO rates.45 The ReAl-time UltraSound facilitates transradial access (RAUST) Trial prospectively compared ultrasound guided access to access with palpation alone in 698 patients. The RAUST trial found ultrasound guidance increases the speed and efficacy of TRA, decreasing time to access and number of attempts, while increasing the first-attempt success rate.46 Familiarity with the use of real-time ultrasound for vascular access is expected to shorten the ‘learning curve’ associated with a transition from TFA to TRA and minimise the need for access crossover in patients with weak radial pulse.

Counterpuncture technique for TRA. (A) Starting position with the patient’s wrist hyperextended. (B–C) The needle is inserted into the radial artery until a ‘flash’ is observed, after which the needle is advanced through the posterior arterial wall (‘counterpuncture’). (D) After removing the needle, the cannula is steadily withdrawn, as shown, to reduce the angle between the cannula and artery until blood is encountered. (E) Introduce the guidewire into the cannula quickly.
Sheath size
Several studies have shown that there is a difference between what size sheath the radial artery can physically accommodate and what size sheath will result in the radial artery remaining patent after the procedure. Although as discussed above, radial artery occlusion carries almost no clinical consequence, it is clearly optimal to attempt to maintain radial artery patency if possible for future interventions. Saito et al noted that 14% of men and 27% of women have a radial artery diameter smaller than a 6 French (F) sheath, and that sheath size greater than artery diameter was associated with a threefold increase in severe reduction in blood flow to the hand.47 Interestingly, the radial artery could be cannulated with the 6F sheath in all patients, demonstrating the elastic properties of the radial artery. None of the 250 patients sustained RAO or hand ischaemia following the procedure. A prospective trial found that patients randomized to a 5F sheath had a significantly lower incidence of RAO (1.1% vs 5.9%) than the 6F sheath group.48 Furthermore, a randomized trial of 160 patients demonstrated a lower incidence of RAO and complications with the use of a 4F sheath versus a 6F sheath.49 Hydrophilic coating of the sheath, but not the length of the sheath, has also been shown to reduce RAS incidence.50 In addition, the use of sheathless guide catheters has been described and has shown promise as a mechanism to maximise the inner diameter of the catheter while minimising the outer diameter.51 52
Haemostasis technique
In addition to sheath size, the actual technique for achieving and maintaining haemostasis after the procedure strongly affects the radial artery patency rates. The ‘patent haemostasis technique’ refers to the maintenance of anterograde flow through the radial artery while obtaining haemostasis of the puncture site (figure 3). The PROPHET study randomized 436 patients to conventional versus patent haemostasis. They found a 75% reduction in RAO at 30 days with the use of patent haemostasis, with an overall rate of RAO of 1.8% in the patent haemostasis group.53 Sanmartin et al found that the absence of anterograde radial artery flow during ahemostasis has been shown to be an independent factor associated with RAO.54 Pancholy et al, in a randomised trial of 400 patients, found patent haemostasis to be the most important tool to prevent RAO.55
{kind=link}
{kind=link}
{kind=link}
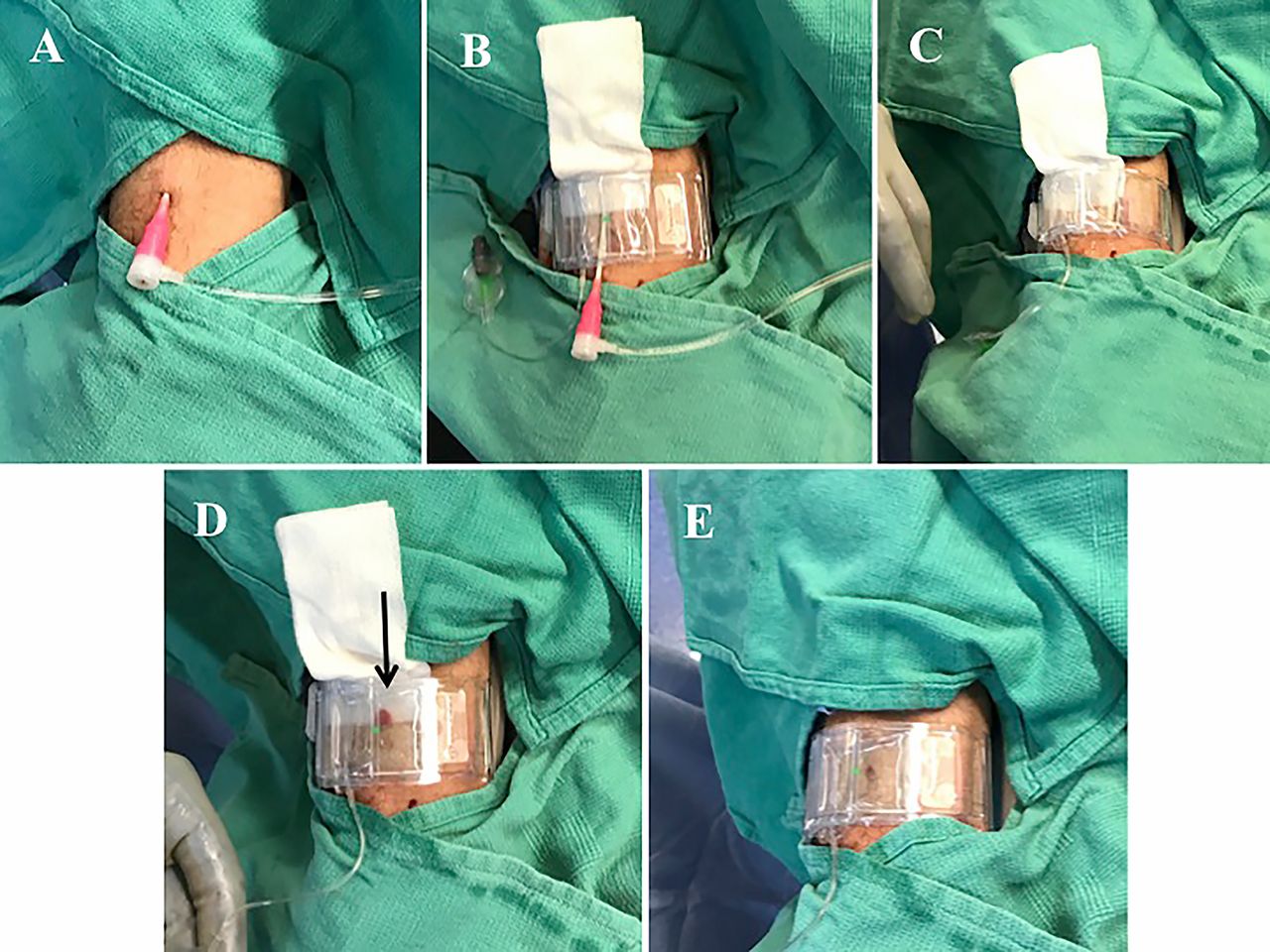
Patent haemostasis technique. (A) Radial access with sheath before haemostasis technique.(B) Patent haemostasis first involves the placement of the haemostatic wristband, which is secured 1–2 cm proximal to the point of arteriotomy and inflated. (C) The sheath is then removed with the band inflated. (D) The band is then deflated until oozing (arrow) is seen from the puncture site. At this point, a small amount of air is introduced to the band to re-achieve haemostasis (thus with the minimal amount of pressure required). With a pulse oximeter attached to the patient’s index finger, the ulnar artery is compressed manually (‘reverse Barbeau test’). (E) If RA patency is confirmed, the patient can be transitioned to the recovery area with frequent assessment of both RA patency and haemostasis.
If RA patency is not confirmed, continued attempts can be made to decrease the band pressure while maintaining haemostasis, re-establishing patency on subsequent attempts. If the radial artery remains occluded, compression of the ipsilateral ulnar artery has been shown to decrease RAO rate. Bernat et al, in a prospective trial of 243 patients, found that compression of the ulnar artery for 1 hour decreased RAO from 2.9% to 0.8%.56 Furthermore, the PROPHET-II study, a randomized prospective trial of 3000 patients, demonstrated a RAO reduction from 3.0% to 0.9% with prophylactic ipsilateral ulnar artery compression when compared with standard patent haemostasis techniques.57 No significant hand ischaemia was demonstrated in either trial.
Learning curve in adopting TRA
Several studies have evaluated the learning curve itself for transradial access. Ball et al. studied procedural metrics of 1672 transradial coronary interventions among 28 operators, and found that case volumes of at least 50 cases has been shown necessary to achieve outcomes comparable to experienced operators with regards to crossover and other measures of proficiency, including fluoroscopy time and contrast use.58 Furthermore, the odds of procedural failure decreased 32% with every 50 cases performed. A similar study compared more than 54 000 transradial procedures among 942 operators in a national data registry.59 They found that a threshold of 30 to 50 cases needed to achieve the proficiency of operators experienced with TRA. In addition, they found that operators continued to improve despite taking on more difficult procedures and patients. This is unsurprising given that the radial artery is smaller than the femoral artery. Interestingly, given the transition of some practices almost exclusively to radial access, there has been concern expressed that fellows no longer have the requisite skills to perform femoral access.
Limitations
While there is a great degree of overlap between interventional c ardiology and neuro-intervention in regards to access techniques, catheter navigation and therapeutic goals, it is difficult to extrapolate clinical outcomes between TRA and TFA in interventional cardiology to neuro-intervention. For that reason, the importance of this article is to provide neuro-interventionalists with a comprehensive introduction to TRA, as told by cardiology, to allow for further dialogue and research into implementing TRA for specifically neuro-interventional procedures.
Conclusion
The breadth and depth of the cardiac literature supporting the radial approach over the femoral is impressive. However, whether the success of the radial approach, as seen in cardiology, can be achieved in neuro-intervention remains to be seen. Given the long history of neuro-intervention adopting innovations from interventional cardiology, consideration of the radial approach for neuro-intervention seems prudent. The anatomical differences between navigating inferiorly to the coronary circulation and navigating superiorly to the great vessels can likely be overcome with a combination of industry innovation and operator experience.
References
Footnotes
Contributors All authors contributed to the conception, literature review and drafting of the manuscript. MGC and ECP provided manuscript oversight and administrative support. All authors critically reviewed the manuscript and approved its final submission.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.