Article Text

Abstract
Introduction Non-saccular aneurysms of the posterior circulation are uncommon but highly dangerous lesions. Flow diverter stents have been demonstrated to be effective treatments of various anterior circulation aneurysms, particularly large and giant proximal internal carotid artery aneurysms. However, evidence regarding the treatment of non-saccular posterior circulation aneurysms with flow diverters is lacking.
Methods A systematic literature review of the English language literature since 2007 was conducted using PubMed, MEDLINE, and Embase. Keywords and MeSH terms included flow diversion, flow diverter, pipeline, surpass, intracranial aneurysm, vertebrobasilar, and non-saccular. Case reports were excluded. Angiographic and clinical outcomes were pooled using a random effects meta-analysis.
Results 13 retrospective non-comparative studies reporting 129 patients and 131 aneurysm treatments were included. The average number of flow diverters per aneurysm was 4.33. Immediate complete or near complete occlusion of the aneurysm occurred in 25% (95% CI 1% to 60%), and long term occlusion in 52% (29–76%). Periprocedural stroke occurred in 23% of cases. Good long term neurologic outcome (modified Rankin Scale score ≤2) was achieved in 51% (95% CI 31% to 71%). Overall mortality was 21% (95% CI 7% to 38%) and morbidity was 26% (12%–42%). Retreatment was required in 5% (95% CI 0% to 14%). Good neurologic outcome rate was higher in vertebral artery aneurysms (83%) than other locations (18–33%).
Conclusions Flow diversion is a feasible and efficacious treatment for non-saccular aneurysms in the posterior circulation. However, the intervention carries a significant risk of periprocedural stroke, and is still associated with high overall mortality. Further studies are needed to identify significant treatment risk factors and optimize patient selection.
Statistics from Altmetric.com
Introduction
Endovascular treatment for intracranial aneurysms is a rapidly evolving field, within which new, innovative devices routinely reshape the treatment landscape. Among the most significant recent advances, flow diverters have had a tremendous impact, and their indications and clinical use continue to expand. Flow diversion is mechanistically unique in that it changes the interface of the parent artery and aneurysm sac, facilitating endoluminal reconstruction and aneurysm thrombosis rather than reducing endosaccular filling via direct coil occlusion. Subsequent intrasaccular thrombosis and further neointimal growth over the stent diverter reconstructs the parent artery, eliminating the aneurysm/parent artery interface.1
Non-saccular aneurysms in the posterior circulation are rare but associated with substantial morbidity and mortality. Presentation is highly variable: aneurysm rupture causing subarachnoid hemorrhage, dissection causing headache, ischemic stroke, or transient ischemic attack due to thrombosed aneurysm, mass effect causing cranial nerve palsies, brainstem or cerebellar compression causing ataxia, or asymptomatic incidental finding. Evidence regarding the natural history of these aneurysms is limited; however, overall prognosis appears to be unfavorable, with high rupture and rebleeding rates, and 24–33% mortality independent of treatment.2–4
Application of flow diversion to non-saccular posterior circulation aneurysms is not straightforward, and initial studies have demonstrated high morbidity and mortality associated with treatment.5–7 However, as experience has expanded, recent studies have suggested more optimistic outcomes.8 9 Ultimately, the evidence surrounding treatment outcome of flow diversions in posterior circulation non-saccular aneurysms requires further evaluation. Thus we performed a systematic review and meta-analysis of outcomes of flow diversion for treatment of posterior circulation non-saccular aneurysms.
Materials and methods
Literature search and study selection
Studies were identified by a search of PubMed, MEDLINE, and Embase for studies on non-saccular aneurysms in the posterior circulation treated with flow diverters published as of November 2016. The search was performed by a medical librarian using keywords including flow diversion, flow diverter pipeline, surpass, intracranial aneurysm, vertebrobasilar, and non-saccular, in both AND and OR combinations. Consecutive case series studying non-saccular aneurysms in the posterior circulation treated with flow diverters were included. Studies addressing saccular aneurysms were excluded, as these lesions have distinct natural histories and pathologic characteristics. Posterior cerebral artery aneurysms were excluded. Dissecting aneurysms were included. Single case reports were excluded. The eligibility assessment of the articles was initially performed by three reviewers. The senior reviewer resolved disagreements. Reference lists of included articles were scanned as an additional means of identifying articles.
Data abstraction
Information was extracted through a prespecified data extraction protocol. From each included study, we collected the following data: (1) immediate and long term angiographic occlusion, (2) antiplatelet regimen, (3) retreatment rate, (4) morbidity and mortality related to the procedure, (5) procedure related rupture, (6) procedure related thromboembolism, and (7) long term neurologic outcome.
The angiographic outcome data were divided into two groups: complete or near complete angiographic occlusion, and incomplete occlusion. Results reporting the angiographic findings by using the Raymond grading system (class 1, complete obliteration; class 2, neck remnant; class 3, aneurysm remnant) were translated to our methods as follows: classes 1 and 2 were considered complete or near complete angiographic occlusion, and class 3 was included in the incomplete occlusion group. Angiograms documented as follow-up at 3 months at least were regarded as long term outcome.
Good neurologic outcome was defined as Glasgow Outcome Scale grades 4 and 5, or modified Rankin Scale scores of 0–2. Morbidity related to the procedure included any events documented in the periprocedural period which resulted in permanent poor neurologic outcome.
Subgroup analyses were performed for the following patient groups: (1) unruptured aneurysm, (2) small aneurysm (maximal axial section diameter <10 mm), and (3) aneurysm location.
Risk of bias assessment
Risk of bias assessment was performed using a modified Newcastle Ottawa Scale.10 This is a tool used for assessing the quality of non-randomized studies included in systematic reviews and/or meta-analyses. Each study is judged based on the domains of selection of the study groups and ascertainment of the outcome of interest.11 Factors that would make a study at low risk of bias would include: (1) well defined selection criteria, (2) well defined treatment regimen, including antiplatelet regimen, (3) rates of long term follow-up >90% for surviving patients, and (4) stratification of outcomes by rupture status.
Statistical analysis
All included studies were non-comparative. We estimated from each cohort the cumulative incidence (event rate) and 95% CI for each outcome. Event rates for each intervention were pooled in a meta-analysis across studies by using the random effects model.12 Anticipating heterogeneity among studies, we chose this model a priori because it incorporates within study variance and between study variance. Heterogeneity of the treatment effect across studies was evaluated using the I2 statistic.13 We considered I2 statistic >50% to indicate substantial heterogeneity. We were unable to test for publication bias due to the non-comparative nature of the studies. The meta-analysis was performed using the statistical software package StataCorp 2015 (Stata Statistical Software: Release 14. College Station, Texas, USA: StataCorp LP).
Results
Characteristics of included studies
The literature search yielded 311 articles, of which 13 met the inclusion criteria (figure 1). Twelve studies were single center case series; one study was a four institution study (table 1).
Summary of included studies
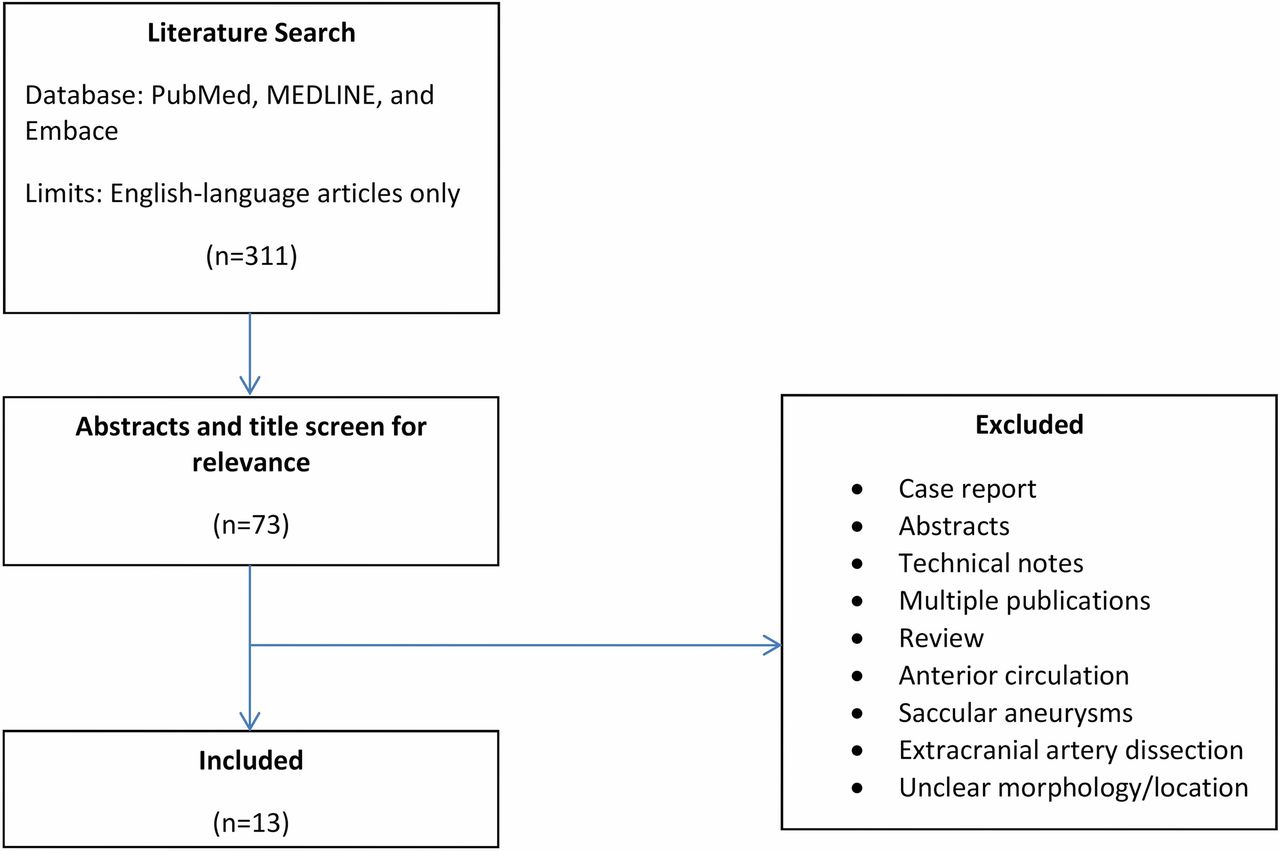
Flow diagram of the search strategy and study selection.
All studies were retrospective, and selection criteria were clearly documented. Seven provided data on only unruptured aneurysms, two only on ruptured aneurysms, and four included both ruptured and unruptured aneurysms. A total of 131 non-saccular posterior circulation aneurysms treated with flow diverters (15 ruptured, 116 unruptured) were included in this meta-analysis. Median follow-up was 11.25 months. The number of symptomatic aneurysms was 74. A total of 567 flow diverters were used, and the average number of flow diverters used per aneurysm was 3.41. In 119 cases dual antiplatelet therapy was documented (91%).
Overall outcomes
The immediate angiographic occlusion/near occlusion rate was 25% (95% CI 1% to 60%) (table 2).
Overall outcomes
The rate of long term complete/near complete occlusion was 52% (95% CI 29% to 76%). Rate of intraoperative rupture was 0% (95% CI 0% to 0%). Thromboembolic complications occurred in 23% (95% CI 10% to 39%). The all-cause morbidity was 26% (95% CI 12% to 42%), most of which was related to thromboembolic complications, while all-cause mortality was 21% (95% CI 7% to 38%). Fifty-one per cent (95% CI 31% to 71%) of patients were in good neurologic condition at the last follow-up at a median of 11.25 months (figure 2). Retreatment was performed in 5% (95% CI 0% to 14%).

Forest plot for good neurologic outcome.
Outcomes of unruptured aneurysms
Immediate angiographic occlusion/near occlusion rate was 11% (95% CI 0% to 34%) (table 3).
Outcome of unruptured aneurysms
The long term angiographic complete/near complete occlusion rate was 43% (95% CI 24% to 64%). Periprocedural rupture occurred in 0% (95% CI 0% to 0%); thromboembolic complications occurred in 24% (95% CI 8% to 44%). All-cause morbidity was 26% (95% CI 7% to 50%), and all-cause mortality was 27% (95% CI 10% to 48%). Forty-nine per cent (95% CI 26% to 71%) of patients had good neurologic condition at the last follow-up. Retreatment was required in 2% (95% CI 0% to 12%).
Outcomes by aneurysm size
Immediate angiographic occlusion/near occlusion rate was 79% (95% CI 46% to 100%) (table 4) in small aneurysms and 3% (95% CI 0% to 26%) in large aneurysms.
Outcomes by aneurysm size
The long term angiographic occlusion/near rate was 100% (95% CI 84% to 100%) in small aneurysms, and 28% (95% CI 8% to 53%) in large aneurysms. Periprocedural rupture occurred in 0% in both groups (95% CI 0% to 0% in small aneurysms and 0% to 2% in large aneurysms). Thromboembolic complications occurred in 12% (95% CI 0% to 51%) of small aneurysms and in 22% (95% CI 7% to 41%) of large aneurysms. All-cause morbidity was 18% (95% CI 0% to 56%) in small aneurysms and 29% (95% CI 13% to 48%) in large aneurysms. All-cause mortality was 5% (95% CI 0% to 41%) in small aneurysms and 27% (95% CI 6% to 53%) in large aneurysms. Seventy per cent (95% CI 34% to 91%) of patients with small aneurysms were in good neurologic condition at the last follow-up compared with 44% (95% CI 19% to 70%) in the large aneurysm group. Retreatment was required in 0% (95% CI 0% to 2%) of small aneurysms and 2% (95% CI 0% to 9%) of large aneurysms.
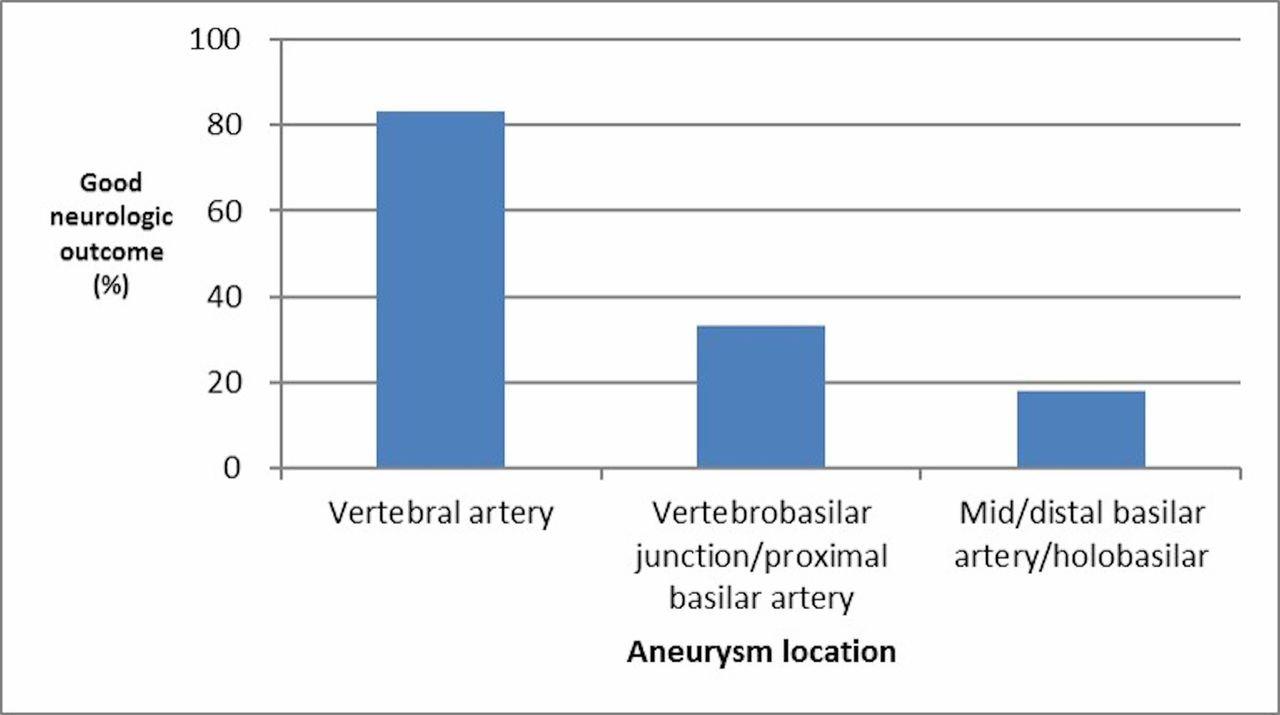
Neurologic outcomes by aneurysm location
Each study used a different classification in location of the aneurysms. In studies where we were able to specify the location by the vertebral artery, vertebra-basilar junction and proximal basilar artery, mid/distal basilar artery and holobasilar artery, the rates of good neurologic outcome in each group were as follows: vertebral artery (10/12, 83%), vertebra-basilar junction and proximal basilar artery (4/12, 33%), and mid/distal basilar artery and holobasilar artery (2/11, 18%) (figure 3).

{kind=link}
{kind=link}
{kind=link}
Good neurologic outcome by aneurysm location.
Study heterogeneity
In the small aneurysm group, I2 statistics for all outcomes were <50%. In the large aneurysm group, I2 statistics were >50% for long term complete/near complete occlusion, mortality, and long term favorable neurologic outcome. In the unruptured aneurysm group, I2 statistics were >50% for long term angiographic occlusion/near occlusion, thromboembolic complication, morbidity, mortality, and long term neurologic outcomes. For all aneurysms, I2 statistics were >50% for initial and long term complete/near complete angiographic occlusion, thromboembolic complication, mortality, and long term favorable neurologic outcome (tables 2–4).
Discussion
This systematic review and meta-analysis found wide variability in outcomes after flow diversion for treatment of non-saccular posterior circulation aneurysms. Despite treatment, morbidity and mortality rates in these patients were quite high, with only 50% of patients reaching a good neurological outcome and nearly 25% suffering ischemic complications. However, our results also suggest that, in the context of the poor natural history inherent to these lesions, treatment of select cases may be safe and effective. 2-4, 24 2–4 14 Our subgroup analyses discovered that smaller aneurysms (<10 mm) had better outcomes compared with larger aneurysms. In addition, vertebral artery aneurysms were associated with higher rates of good neurological outcome than mid/holobasilar and vertebrobasilar junction aneurysms. These findings are important as they suggest that patients who undergo flow diversion treatment of non-saccular posterior circulation aneurysms should be carefully selected, so as not to worsen the natural history.
Non-saccular posterior circulation aneurysms have varying morphological and etiological characteristics that can influence both natural history and treatment options.8 Understanding the natural history of these lesions is essential to improving patient selection. Non-saccular dissecting aneurysms commonly present with subarachnoid hemorrhage and are associated with mortality rates as high as 20%.25 15 Meanwhile, fusiform aneurysms most frequently present with ischemic stroke symptoms (44%), or mass effect yielding cranial nerve palsies or hydrocephalus, and have a rupture rate of 1.7%/year.26 16 Transitional aneurysms appear to have the least favorable natural histories with frequent aneurysm growth (15.8%/year) and high rupture rates (3.5%/year).26 16 Among patients with aneurysms <10 mm, Nasr et al found that the annual rupture rate was just 0.6% per year compared with 6.8% per year for aneurysms 10 mm or larger. Data from our meta-analysis suggest that treatment of large and holobasilar aneurysms is associated with very high rates of morbidity and mortality, perhaps worse than the natural history of the lesion.26 16 Meanwhile, treatment of smaller fusiform aneurysms is associated with lower, but not negligible, complication rates which, in the context of the natural history of the lesion, may be acceptable in the right clinical setting.
While there is wide variability in reported outcomes after endovascular treatment of these lesions, the importance of proper patient selection has become increasingly clear. This point is best demonstrated by two back to back studies published by the Buffalo group in 2012 and 2016. All patients in both studies had symptomatic unruptured vertebrobasilar fusiform aneurysms, and were treated with the same flow diverters (Pipeline). In a study of seven patients undergoing flow diversion for treatment of non-saccular posterior circulation aneurysms, Siddiqui et al demonstrated remarkably high mortality (57%) and thromboembolic complications (72%) with correspondingly low rates of favorable neurologic outcomes (29%).22 17 However, in a subsequent study performed at the same institution, Natarajan et al used more refined selection criteria—namely, the avoidance of holobasilar aneurysms, or aneurysms with a large amount of thrombus—and reported 0% mortality, 8% thromboembolic complication rate, and 92% good neurologic outcomes.9 Indeed, in the present study, the rate of good neurologic outcome in the holobasilar aneurysm group (2/11, 13%) was lower than other locations (33–83%).
The next key distinction between these studies include the number of flow diverters used: in the first series, a mean of five flow diverters were used per aneurysm, compared with 1.67 in the second study. The authors suggest that, the more flow diverters used, the more pronounced the risk of perforator damage.
Several other factors likely contributed to the differences observed between these temporaly adjacent studies from the same center. In the second study, the therapeutic effect of dual antiplatelet therapy was more rigorously confirmed prior to flow diversion. Adjunctive coiling was also more conscientiously employed as a scaffold, to prevent flow diverter induced collapse of the fusiform component. Finally, mean treated aneurysm size decreased from 20.83 mm to 13.25 mm, with fractional populations of large aneurysms similarly declining from 83% to 72%. Taken together with our finding that, in all subgroups, smaller aneurysm size predisposes to better outcome, these comparative data suggest that the risk curve may accelerate from a linear to an exponential pattern beyond the 10 mm threshold.
Location of the aneurysms should also be taken into consideration. Each study used a different classification in location of the aneurysms, which limited our analysis, but the rate of good neurologic outcome in vertebral artery non-saccular aneurysms was higher than other locations, and mid/distal basilar artery/holobasilar location was the worst. Munich et al also suggested that the flow diverter should be placed caudal to the anterior inferior cerebellar artery, and metal surface area coverage should be minimized rostral to the anterior inferior cerebellar artery to avoid important perforator injury.16 18 The findings from our meta-analysis corroborates this theory.
Positioning these findings in the broader context of intracranial aneurysm treatment, these outcomes must be considered in comparison with the traditional gold standard of neurosurgical intervention. In a landmark paper on open treatment of posterior circulation aneurysms, Drake et al demonstrated excellent results using a diverse armamentarium of surgical techniques, including clip reconstruction, proximal occlusion, wrapping, and trapping with 67% good neurologic and treatment outcomes.27 19 Conceptually, they emphasized the importance of maintaining two collateral circulations to avoid procedure related infarction in the proximal parent artery occlusion: one for the end vessels and another for the perforating vessels that arise from the aneurysm. As innovative bypass techniques have been refined, the former has become more readily accessible in the open treatment of posterior fossa aneurysms; however, perforator occlusion and consequent infarction remains the most feared and difficult to avoid complications—a risk that, as our study demonstrates, is shared with endovascular modalities in the treatment of these formidable lesions.28 20
Limitations
This study has limitations, chiefly its dependence on exclusively retrospective constituent studies in the meta-analysis. However, considering the rare nature of this pathology, it is potentially unrealistic to conduct prospective studies. Second, outcome reporting was heterogeneous, with various studies excluding data on angiographic outcome, detailed follow-up duration, and post-treatment morbidity. Similarly, long term angiographic and clinical outcomes were measured at different time points in each study. With respect to data quality, we found significant heterogeneity in our meta-analysis across almost all outcomes. Finally, each of the four principal aneurysm types included (dissection, fusiform, transitional, and dolichoectatic) has been shown previously to be characterized by a relatively unique clinical presentation and history; consequently, in order to best understand and optimize the treatment paradigms for each, more case accumulation and nuanced data recording is clearly required. Disparate results reported by the Buffalo group underline that there are fundamentally different patient populations in the posterior fossa non-saccular aneurysm population which should be treated in different ways. These issues might fundamentally plague this meta-analysis since there is an insufficient number of patients to do subgroup analyses and insufficient detail to assign to subgroups.
Conclusion
Treatment outcomes of non-saccular aneurysms of the posterior circulation are highly variable and are highly dependent on patient selection. Of particular interest, treatment of smaller aneurysms (<10 mm) appears to have the most favorable safety profile and overall neurologic and treatment outcomes. Notwithstanding, even with ideal treatment, mortality may be in excess of 21%, with thromboembolic complication occurring in 23%. Future studies of these rare entities should include multiple registries. Data collected should include clinical functional and quality of life outcomes with and without treatment. Complete radiographic characterization of these lesions should include the size, potential etiology, relationship to perforators, and whether the pathology extends beyond the widened segment. Detailed data on the procedure and post-procedure efficacy should be obtained. Ultimately with larger numbers, the risk factors for thromboembolic complications can be delineated to more definitively optimize a meaningful treatment algorithm.
References
Footnotes
Contributors SK collected studies, collected, cleaned, and analyzed the data, and drafted and revised the paper. CSG and AP collected studies, analyzed the data, and revised the draft paper. MHM monitored the data collection, analyzed the data, and revised the draft paper. KDF analyzed the data and revised the draft paper. GL and LR-C revised the draft paper. WB designed the study, monitored the data collection, analyzed the paper, and drafted and revised the paper. He is the guarantor.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.