Article Text

Abstract
Background Endovascular thrombectomy has demonstrated benefit for patients with acute ischemic stroke from proximal large vessel occlusion. However, limited evidence is available from recent randomized trials on the role of thrombectomy for M2 segment occlusions of the middle cerebral artery (MCA).
Methods We conducted a systematic review and meta-analysis to investigate clinical and radiographic outcomes, rates of hemorrhagic complications, and mortality after M2 occlusion thrombectomy using modern devices, and compared these outcomes against patients with M1 occlusions. Recanalization was defined as Thrombolysis in Cerebral Infarction (TICI) 2b/3 or modified TICI 2b/3.
Results A total of 12 studies with 1080 patients with M2 thrombectomy were included in our analysis. Functional independence (modified Rankin Scale 0–2) rate was 59% (95% CI 54% to 64%). Mortality and symptomatic intracranial hemorrhage rates were 16% (95% CI 11% to 23%) and 10% (95% CI 6% to 16%), respectively. Recanalization rates were 81% (95% CI 79% to 84%), and were equally comparable for stent-retriever versus aspiration (OR 1.05; 95% CI 0.91 to 1.21). Successful M2 recanalization was associated with greater rates of favorable outcome (OR 4.22; 95% CI 1.96 to 9.1) compared with poor M2 recanalization (TICI 0–2a). There was no significant difference in recanalization rates for M2 versus M1 thrombectomy (OR 1.05; 95% CI 0.77 to 1.42).
Conclusions This meta-analysis suggests that mechanical thrombectomy for M2 occlusions that can be safely accessed is associated with high functional independence and recanalization rates, but may be associated with an increased risk of hemorrhage.
- thrombectomy
- stroke
Statistics from Altmetric.com
Introduction
Recent trials have established the benefit of mechanical thrombectomy (MT) over medical management alone in patients with acute ischemic stroke from large vessel occlusion (LVO) of the anterior circulation.1–5 However, evidence from these trials for benefit from treatment of more distal occlusions including the M2 segment of the middle cerebral artery (MCA) is limited, as these trials were underpowered to address this question. Therefore, the efficacy and safety of MT in M2 occlusions remain unproven.
The natural history of M2 occlusions can be one of severe disability, with 6-month mortality rates comparable to those of M1 occlusions.6 Whereas data on the efficacy of M2 thrombectomy using older reperfusion devices were inconclusive,7–9 several recent single- and double-arm studies have demonstrated acceptable rates of functional outcome, morbidity, and mortality for M2 occlusions treated with MT using second-generation devices.10–22
Conducting a randomized trial that includes a non-intervention arm to better characterize the effect of MT in patients with M2 occlusions may not be feasible due to the lack of clinical equipoise, highlighted by the fact that MT is performed for patients with M2 occlusion in many institutions, drawing from the evidence of the few randomized trials that did include patients with M2 occlusions. As such, prospective registries and meta-analyses may provide the best data to address this question and to identify factors associated with improved clinical outcomes following MT in patients with M2 occlusion.
We performed a meta-analysis to investigate clinical and radiologic outcomes of MT in M2 occlusion using modern devices, and to compare these outcomes relative to M1 thrombectomy. The safety and effectiveness of MT in M2 occlusions were also compared by device type (aspiration vs stent-retrievers) used for thrombectomy.
Methods
Literature search
This review was conducted in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. A search was performed in July 2017 using Medline, Embase, and Cochrane databases. The literature search was performed by two of the authors (HS and SAS) with extensive experience in the field and a sufficient fund of knowledge to assess each article on its suitability. The search terms included stroke AND (‘middle cerebral artery’ OR ‘M2’) AND (‘thrombectomy’ OR ‘endovascular’). Duplicates were removed from records identified in the database search. Articles were then screened based on title and abstract, and the remaining papers underwent full-text review (see online supplementary figure 1). The Newcastle–Ottawa Scale was used to estimate the methodological quality of studies included in the final analysis (see online supplementary table 1). M2 branch was defined according to anatomic boundaries, in which the M2 segment begins at the genu of the MCA as it takes a vertical turn in the Sylvian fissure, or by branching pattern, in which post-bifurcation branches of the M1 are defined as M2 vessels. The inclusion criteria were as follows: (1) at least 10 patients treated with MT for acute ischemic stroke due to M2 occlusion; (2) reporting a measure of treatment time and a measure of clinical outcome for patients treated with M2 thrombectomy; and (3) the use of primarily modern second-generation thrombectomy devices (eg, Trevo, Solitaire, Penumbra aspiration system) in >80% of cases. Aspiration was defined as aspiration thrombectomy as the only approach for recanalization.
Supplementary file 1
Data extraction and outcomes
Demographic and baseline information (number of patients, age, sex, initial National Institutes of Health Stroke Scale (NIHSS) and Alberta Stroke ProgramEarly CT (ASPECT) scores), treatment (MT device type, proportion of patients who received intravenous tissue plasminogen activator (tPA) before thrombectomy, MT attempts, onset to recanalization times), and clinical and safety outcomes were extracted from eligible studies.
Clinical outcomes included successful recanalization (Thrombolysis in Cerebral Infarction (TICI) 2b/3 or modified TICI 2b/3 recanalization rate) and 90-day functional independence (modified Rankin Scale (mRS) 0–2 rate at 90 days). Clinical safety outcomes included 90-day mortality rate and symptomatic intracerebral hemorrhage (sICH) rate defined as any type of hemorrhage with an increase of ≥4 in NIHSS score.
Statistical analysis
Clinical outcomes and recanalization rates for M2 thrombectomy were assessed by meta-analysis using the R for Statistical Programming. Comparisons of outcomes for M1 versus M2 thrombectomy were performed using the Review Manager (RevMan) Version 5.3 (Nordic Cochrane Centre, The Cochrane Collaboration, 2012, Copenhagen, Denmark). Random effects model was used for meta-analysis. Cochran Q test and I2 test were used to detect heterogeneity. Significant heterogeneity was defined as either Q values greater than the χ2 critical value at alpha=0.1 level, or an I2 value greater than 50%. A funnel plot for the primary efficacy outcome was not suggestive of publications bias (see online supplementary figure 2). A sensitivity analysis was performed confined only to studies defining the M2 segment as originating post-vertical turn of the MCA.
Results
MCA-M2 thrombectomy outcomes
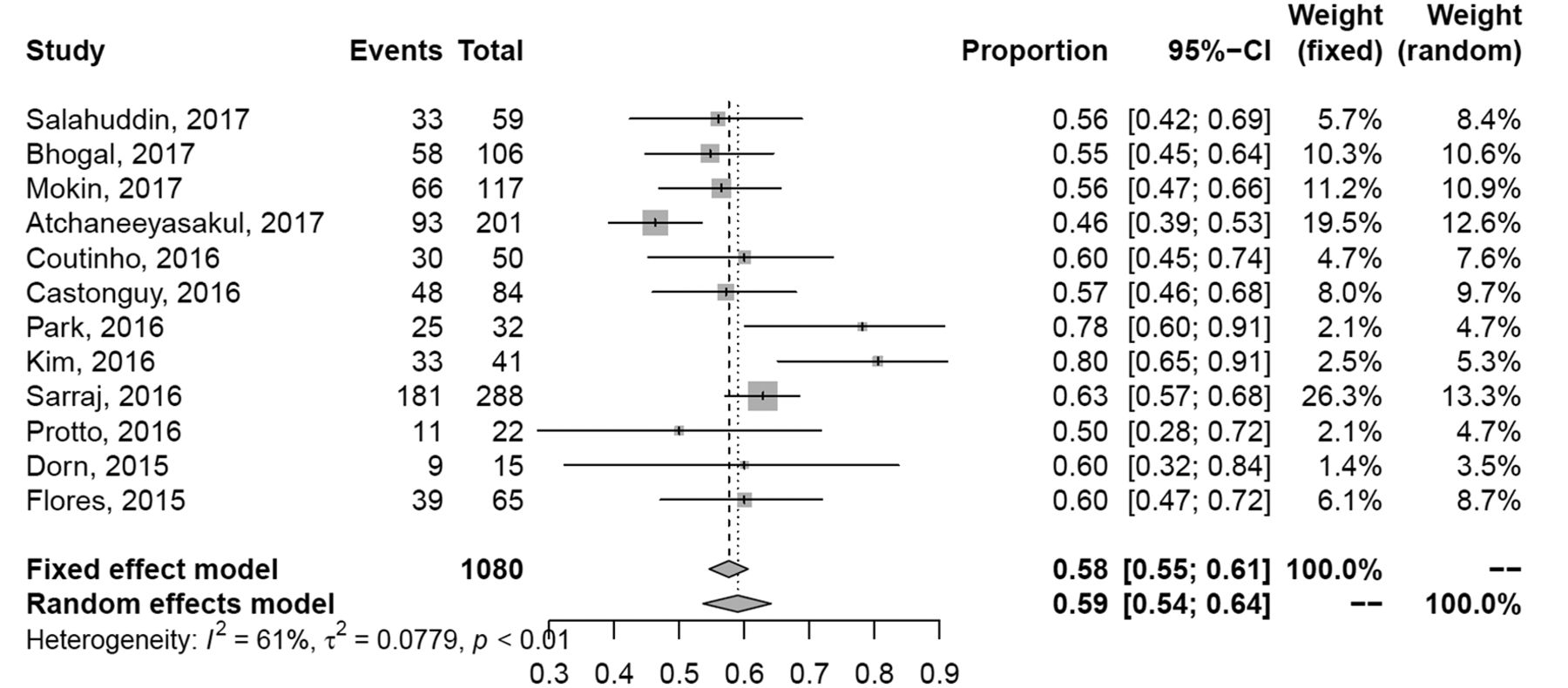
A total of 12 studies comprising 1080 patients with M2 thrombectomy were included in this analysis (table 1). The functional independence rate was 59% (95% CI 54% to 64%) (figure 1). The recanalization rate was 81% (95% CI 79% to 84%) and mortality and sICH rates were 16% (95% CI 11% to 23%) and 10% (95% CI 6% to 16%), respectively (table 2 and online supplementary figure 3A–C).
Demographic and baseline characteristics
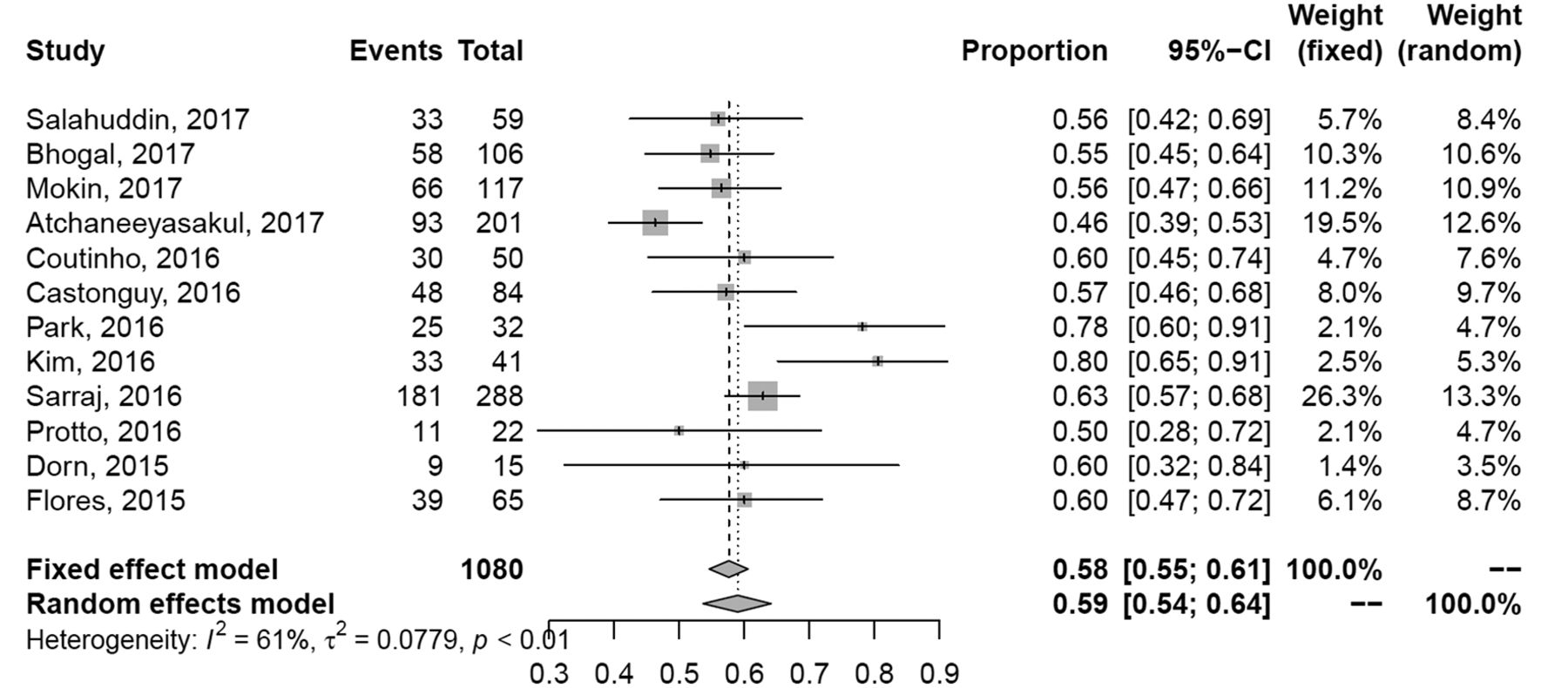
Forest plot of M2 thrombectomy modified Rankin Scale (mRS) 0–2 by study.
Summary rates for M2 thrombectomy outcomes
Data on functional outcomes by recanalization status (2b/3 vs 0–2a) were available for 229 patients with M2 thrombectomy from four studies. Overall, successful M2 recanalization was associated with greater rates of functional independence (OR 4.22, 95% CI 1.96 to 9.1) compared with those with poor recanalization (TICI 0–2a) following M2 thrombectomy.
A sensitivity analysis of TICI2b/3 recanalization and 90-day mRS 0–2 outcomes, restricted to those with M2 segment defined as vertical MCA branches in the Sylvian fissure, did not significantly alter these estimates (80% (95% CI 76% to 84%) and 61% (95% CI 56% to 65%), respectively) (see online supplementary figure 4A–C).
MCA-M1 versus MCA-M2 thrombectomy outcomes
A total of six studies were included in an analysis comparing M1 (n=1375, mean (SD) age 69.1 (13.8) years, 47% men) versus M2 (n=337, mean (SD) age 68 (11.4) years, 45% men) thrombectomy (see online supplementary table 2). Baseline NIHSS scores were relatively lower in patients with M2 occlusion compared with those with M1 occlusion (13.5 vs 16.7). Time of onset to recanalization (339.2±40 min and 327.34±82 min, P=0.63) and total number of passes (2.1 and 1.6, P=0.4), as well as use of intravenous tPA (57% vs 59%, P=0.03) were similar between the M1 and M2 occlusion intervention arms across studies.
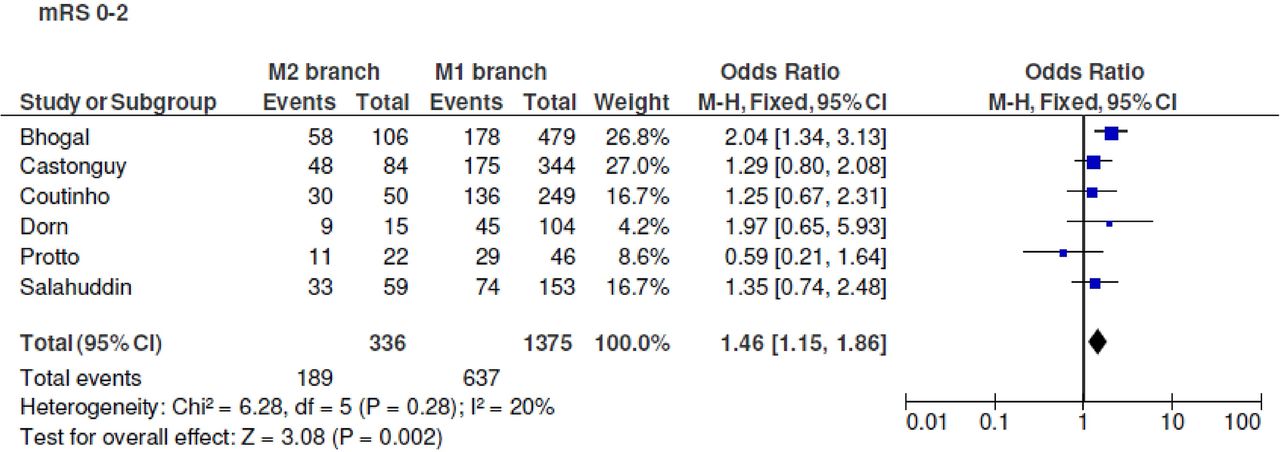
Functional independence 90 days after stroke was seen in 56.2% (189) of patients with M2 intervention and 46.3% (637) of patients with M1 intervention. The proportion of patients with mRS 0–2 was significantly higher in the M2 intervention group than in the M1 intervention group (OR 1.46, 95% CI 1.15 to 1.86; P=0.002; I2=20%). No significant heterogeneity was seen across the studies (figure 2).
{kind=link}
{kind=link}
Forest plot of 90-day modified Rankin Scale (mRS) 0–2 outcome in M2 versus M1 occlusion thrombectomy.
TICI2b/3 was seen in 84.9% (344) of patients with M2 intervention and 84.2% (1311) of patients with M1 intervention. No significant difference in TICI2b/3 was seen between the patients with M2 intervention and those with M1 intervention (OR 1.05, 95% CI 0.77 to 1.42; P=0.78; I2=18%). No significant heterogeneity was seen across the studies (see online supplementary figure 5A).
Mortality occurred in 15.8% (53) of patients with M2 intervention and 18.5% (254) of patients with M1 intervention. No significant difference in mortality was seen between the patients with M2 intervention and those with M1 intervention (OR 0.85, 95% CI 0.61 to 1.17; P=0.31; I2=71%). Significant heterogeneity was seen between the studies (see online supplementary figure 5B). However, a sensitivity analysis showed that the study reported by Dorn et al was a significant contributor to heterogeneity. On exclusion of this study, meta-analysis showed a significant decrease in mortality in patients with M2 branch intervention and no significant heterogeneity across the studies (13.4% (43) vs 18.2% (232); OR 0.69, 95% CI 0.49 to 0.99; P=0.04; I2=0%).
sICH was significantly higher in patients with M2 intervention (15% (56)) compared with M1 intervention (4.7% (65)) (OR 3.39, 95% CI 2.31 to 4.98; P<0.001; I2=7%). No significant heterogeneity was seen across the studies (see online supplementary figure 5C).
Stent-retriever versus aspiration in M2 thrombectomy
TICI2b/3 was seen in 87% (200) of patients with stent-retriever and 80% (156) of patients with local aspiration. No significant difference in TICI2b/3 was seen by device type (OR 1.05, 95% CI 0.91 to 1.21; P=0.7). No significant heterogeneity was seen across the studies (see online supplementary figure 6A).
Functional independence 90 days after stroke was seen in 57.6% (113) of patients with stent-retriever and 48.6% (70) of patients with local aspiration. No significant difference in functional independence was seen by device type (OR 1.14, 95% CI 0.83 to 1.58; P=0.3). No significant heterogeneity was seen across the studies (see online supplementary figure 6B).
Discussion
In this meta-analysis of patients who underwent MT for isolated acute M2 occlusions with moderate to severe stroke severities, 81% of patients achieved successful recanalization along with high rates of functional independence at 3 months (58%) and low rates of mortality (16%). When compared with M1 occlusions, patients with isolated M2 occlusion achieved similar revascularization rates, with better 90-day functional independence and possibly lower mortality. We did not find any specific association between device type and recanalization outcome.
Current guidelines recommend endovascular therapy as the standard of care for acute ischemic stroke due to an occlusion of the distal internal carotid artery or proximal middle cerebral artery based on five recent landmark trials.23 Among these trials, MR CLEAN (39 patients, 7.8%) and EXTEND-IA (10 patients, 14%) explicitly allowed for M2 occlusions to be included.2 5 Patients with M2 occlusions were randomized in about 10% of the population within SWIFT PRIME (19 patients) and REVASCAT (18 patients) trials despite an exclusion criterion for M2 LVO.1 3 A subgroup meta-analysis of the five recent trials of endovascular stroke therapy, which included individual data for 94 patients with M2 occlusion, showed no significant improvement in 90-day mRS scores following MT compared with medical therapy (OR 1.28, 95% CI 0.51 to 3.21).24 However, these trials provide limited evidence for management of M2 occlusions, as the results could be underpowered due to the small sample size of patients pooled from the trials. Recently, in a large retrospective cohort study comprising 288 patients with M2 occlusion, thrombectomy using modern devices was shown to be associated with significantly higher rates of functional improvement compared with best medical management.22 In contrast, reperfusion was not associated with good functional outcome (mRS 0–2) in patients with M2 occlusions in a pooled individual patient analysis from four older endovascular trials; however, this analysis included treatment with older devices and intra-arterial alteplase7 (see online supplementary table 3).
A randomized trial of MT for M2 occlusions would best determine the effectiveness of endovascular therapy compared with medical therapy in these patients. However, this may not be feasible due to the lack of clinical equipoise, as MT is now routinely performed for M2 occlusions based on the evidence of randomized trials that did include patients with M2 occlusion (ie, MR CLEAN and EXTEND IA). Although this meta-analysis does not address the natural history of M2 occlusions, it provides more precise estimates of favorable outcome rates for M2 thrombectomy than any single study. Furthermore, this analysis method allows for measurement of heterogeneity between studies.
One challenge in evaluating the effect of MT for M2 occlusions is the absence of consensus on the definition of an M2 vessel. An abundance of naming conventions exists, and this variability can be seen as well across the inclusion and exclusion criteria of recent randomized MT trials. One of the more common classifications defines the M2 according to anatomic boundaries, in which the M2 segment begins at the genu of the MCA as it takes a vertical turn in the Sylvian fissure. Another common system defines the segments by branching pattern, in which post-bifurcation branches of the M1 are defined as M2 vessels. Given the high frequency of early bifurcation MCA anatomy, these two classifications often lead to conflicting definitions.9 25 Our sensitivity analysis, confined only to studies defining the M2 segment as originating after the vertical turn of the MCA, did not alter efficacy or safety outcome rates.
In this study we found that M2 occlusions can be associated with poor functional outcome after thrombectomy, with 90-day mortality rates as high as those associated with M1 occlusions. On the other hand, functional independence following M2 thrombectomy in our meta-analysis is comparable to the outcome in the intervention arm of the SWIFT PRIME trial (60%).1 Interestingly, these benefits were observed despite higher sICH rates following thrombectomy for M2 versus M1 occlusions. These increased rates may reflect the risk associated with intervention on smaller, more fragile vessels. However, our results highlight the favorable outcomes associated with endovascular therapy, particularly in patients with M2 occlusion and high NIHSS, regardless of a slight increased risk of hemorrhage. In addition, both primary stent-retriever thrombectomy and local aspiration for M2 thrombectomy showed similar recanalization and 90-day mortality rates. Therefore, both techniques may be viable approaches for M2 thrombectomy.
Our study has several limitations. First, most of the included studies had a retrospective design, and selection of patients for M2 thrombectomy or differences in treatment protocols likely vary between studies. For instance, recanalization was defined as modified TICI in two studies, whereas most other studies reported recanalization based on TICI scores. However, there was only minimal heterogeneity in outcomes across the studies, suggesting no significant variations between studies. Second, the observed high rate of morbidity in M2 occlusions may be explained by the fact that our cohort consists primarily of patients who underwent MT and, as such, will be over-represented with larger, more disabling M2 occlusions. Thus, our results can only be interpreted in the context of patients with M2 occlusions that can be safely accessed by MT, and who present with moderate to severe stroke. When comparing outcomes for M1 and M2 thrombectomy, patients with M1 occlusions had higher baseline NIHSS (16.7 vs 13.5). Although this difference was not statistically significant in an analysis of two studies that reported the mean (SD) for baseline NIHSS scores, higher rates of functional independence in patients with an M2 occlusion are likely due in part to a lower baseline NIHSS score in these individuals. Finally, subgroup analysis by M2 definition or device type only included three studies.
Conclusion
The findings from our meta-analysis demonstrate favorable safety and functional outcomes of MT for patients with M2 occlusions that can be safely accessed, with clinical outcomes that are comparable to guideline-based M1 thrombectomy. Future multicenter cohort studies are needed to investigate factors associated with a favorable outcome in acute ischemic stroke due to distal intracranial vessel occlusions.
Acknowledgments
We thank the participants and staff of all the included studies.
References
Footnotes
Contributors HS, SAS, and SN participated in the conception and design of the study. HS, SAS, and MP analyzed and interpreted the data. HS carried out the statistical analysis and wrote the article. RGN, AJY, and JLS revised the draft paper for intellectual content.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.