Article Text

Abstract
Objective This study retrospectively compared the clinical and angiographic outcomes of treating cerebral aneurysms with Neuroform (NEU), Enterprise (EP), and Low-profile Visualized Intraluminal Support (LVIS/LVIS Jr) stents.
Materials and methods We conducted a retrospective analysis of a procedural database. All aneurysm procedures using any of the three types of self-expanding nitinol stents (NEU, EP and LVIS/LVIS Jr) were included. Intra-procedure complications, post-procedure complications, and angiographic results (Raymond–Roy grade scale, RRGS) were analyzed retrospectively. A multivariate logistic regression analysis was conducted to identify predictors of intra-procedure and post-procedure complications.
Results Two hundred and forty-three aneurysms in 229 patients treated with stent-assisted coiling were included (NEU group: 109 aneurysms; EP group: 61 aneurysms; LVIS/LVIS Jr: 73 aneurysms). The LVIS/LVIS Jr group was associated with the lowest rate of initial complete occlusion (RRGS I: 47.9%; 35/73). Follow-up showed the proportion of RRGS I increased for all stent groups but was greatest in the LVIS/LVIS Jr group. Overall, 17 intra-procedural complications were seen in 229 patients (7.4%) and 15 post-procedural complications were found in 198 patients at follow-up (7.6%), with no differences between stent groups. Thrombotic events were the most common complications and occurred in 13 patients (13/229, 5.7%).
Conclusions All three types of stents used to treat cerebral aneurysms with unfavorable neck were safe and effective, providing suitable support for the coil mass. LVIS/LVIS Jr promotes better progressive aneurysm complete occlusion than the other two stents but seems to cause more common intra-procedural stent-related thrombotic events and fewer post-procedural complications.
- aneurysm
Statistics from Altmetric.com
Introduction
Endovascular coiling for cerebral aneurysms has continued to evolve since the publication of the results of the International Subarachnoid Aneurysm Trial (ISAT) in 2002.1 However, many aneurysms with unfavorable anatomic neck are not appropriate for simple coil embolization alone. Advanced adjunctive techniques for endovascular treatment of wide-necked and complex aneurysms have been introduced, such as stent-assisted coiling,2 which has the theoretical advantage of providing an anatomic barrier and blood flow remodeling for endothelial growth and vessel wall healing.3–8
Despite the recent development of flow-diverting stents,9 10 stent-assisted coiling remains a viable treatment strategy with good rates of aneurysm occlusion, especially for wide-necked cerebral aneurysms.11 12 Neuroform (NEU; Stryker, Kalamazoo, Michigan, USA) and Enterprise (EP, Enterprise EP; Codman & Shurtleff, Raynham, Massachusetts, USA) are laser cut technology stents manufactured from nitinol that can be delivered through standard microcatheters and used for stent-assisted coiling procedures. A new generation of self-expanding braided microstents, the Low-profile Visualized Intraluminal Support stent (LVIS/LVIS Jr; MicroVention, Tustin, California, USA) has been developed.13 14
To date, there have been no direct comparative data on procedure-related complications and the aneurysm occlusion rate between stent types. This study retrospectively compared the clinical and angiographic outcomes of treating cerebral aneurysms with NEU, EP, and LVIS/LVIS Jr stents.
Materials and methods
Patient and aneurysm characteristics
An IRB-approved retrospective analysis of a prospectively collected procedural database was performed. All aneurysm procedures using any of the three types of stents (NEU, EP, and LVIS/LVIS Jr) between March 2009 and February 2016 were included. Inpatient and outpatient clinical data, procedural reports, and angiographic and non-invasive radiological images were analyzed to determine the anatomical and procedural details and adverse events.
Informed consent was obtained for patients to have endovascular stent-assisted coiling of their intracranial aneurysms. The individual operators had free will but not random principle in the choice of stents used for the treatment among the three types. Aneurysm sizes were classified as small (≤5 mm), medium (>5–<15 mm), large (≥15–<25 mm), and giant aneurysms (≥25 mm). An aneurysm was considered to have a wide neck if the size of the neck was >4 mm and/or if the dome-to-neck ratio was <2.
Pharmacologic therapy protocol
Patients with unruptured aneurysms were medicated with dual antiplatelet therapy (aspirin 650 mg and clopidogrel 600 mg) the night before the procedure. Platelet inhibition studies were performed periprocedurally to ensure that the patient was an aspirin and clopidigrel responder; if he or she was not, the patient was loaded with an appropriate weight-based dose of abciximab (0.25 mg/kg) and ticagrelor. This protocol ensured that patients were appropriately inhibited prior to stent deployment.
Patients with ruptured aneurysms were loaded with an appropriate weight-based dose of abciximab (0.25 mg/kg) at the time of stent deployment followed by 325 mg aspirin and 600 mg clopidogrel immediately after the procedure. All patients were subsequently treated with clopidogrel 75 mg and aspirin 325 mg daily for at least 3 months followed by aspirin indefinitely. All patients received heparin intra-procedurally to maintain an activated clotting time level elevated to 2–3 times the baseline value.
Stent techniques and configurations
We used four main techniques at our institution: ‘jailing’, ‘coil-through’, ‘coil-stent’, and ‘balloon-stent’.7 In the ‘jailing’ technique, the microcatheter is placed into the aneurysm sac before stent deployment and jailed between the stent and the vessel intima. In the ‘coil-through’ technique, the microcatheter is advanced through the tines of the stent after stent deployment. For ‘coil-stenting’, unassisted coil embolization is performed followed by stent deployment to obtain the benefit of vascular remodeling or to constrain prolapsed coil loops. Lastly, the ‘balloon-stent’ technique involves balloon-assisted embolization followed by stent deployment. The majority of aneurysms treated by stent-assisted coiling used a single stent configuration. Other stent configurations, including the Y configuration15 16 and telescope configuration,17 were used to treat unusual aneurysms.
The choice of stent techniques and configurations was determined by the operator, taking into account the angiographic architecture of the aneurysm and the advantages and challenges of each available stent.
Complications and follow-up
Procedure-related complications included intra-procedural rupture of the aneurysm or parent artery and stent-related thrombosis (stent-unrelated thrombosis is discussed separately). All complications were analyzed for association with aneurysm size and morphology, aneurysm location, stent type, stent techniques, and stent configuration.
The immediate post-embolization angiogram and follow-up image were studied to assess the degree of aneurysm occlusion by the Raymond–Roy Grade Scale (RRGS)18 (I: complete occlusion; II: neck remnant; III: residual sac). Any further filling of the aneurysm neck or sac over time was referred to as ‘recurrence’.
Post-procedural clinical outcomes at discharge and follow-up at least 6 months later were evaluated using the modified Rankin Scale (mRS). Stroke complications were categorized as major if the mRS score was ≥2 and minor if the mRS score was <2.
Statistical analysis
Descriptive statistics were produced and variables by stent type are presented as N (%) and mean (SD) and tested using the Fisher exact test and analysis of variance for categorical and continuous data, respectively. To formally compare the association of stent type with intra-procedural and post-procedural outcomes, repeated measures mixed-effects logistic regression models were constructed. Covariates were evaluated individually and all covariates identified as being independently associated with procedural or post-procedural outcomes were entered into a full model. A backwards stepwise approach was taken to identify a final model and formally compare stent types. Statistical significance was assessed at alpha=0.05. All analyses were performed using SAS V.9.4.
We checked the effect of potential covariates including sex, age, ruptured aneurysm, lesion location, aneurysm size, aneurysm with wide neck, configuration of stent, method of stent deployment, and preoperative RRGS index which may have an impact on the effect size of stent types on post-procedural complications.
Results
Baseline characteristics
There were 243 aneurysms in 229 patients in our dataset (NEU group: 109 aneurysms in 102 patients; EP group: 61 aneurysms in 58 patients; LVIS/LVIS Jr group: 73 aneurysms in 69 patients). The average age of the participants was 57.97 (range 28–80 years; SD 11.81) and 60 (26.2%) were male. Of the 243 aneurysms (203 wide-necked), 180 (74.1%) were located in the anterior circulation, 107 aneurysms were small (44.0%), 127 were medium (52.3%), 7 aneurysms were large (2.9%), and 2 aneurysms were giant (0.8%). The baseline characteristics of the aneurysms are shown in table 1.
Aneurysm characteristics shown as N (%)
Stent configuration and deployment technique
A single stent configuration was used to treat 218 (89.7%) aneurysms. The ‘jailing’ technique was employed in 39/243 (16.0%), the ‘coil-through’ technique in 116/243 (47.7%), the ‘coil-stent’ technique in 36/243 (14.8%), and the ‘balloon-stent’ in 52/243 (21.5%) (table 1). ‘Coil-through’ was the most commonly employed technique, and ‘jailing’ was used more frequently in the LVIS/LVIS Jr group (21/73, 28.8%) than in the other two groups (EP: 12/61, 19.7%; NEU: 6/109, 5.5%).
Immediate and follow-up angiographic outcomes
The RRGS results for different stent groups are shown in table 2. Digital subtraction angiography (DSA) follow-up was available in 189 patients with 208 aneurysms, giving a follow-up rate of 82.5% (189/229) of patients and 85.6% (208/243) of aneurysms. The mean duration of imaging follow-up was 15.9 months (range 6 months to 6 years); 143 aneurysms and 42 aneurysms had at least 1 year and 2 years of DSA follow-up, respectively.
Distribution of Raymond–Roy Grade Scale (RRGS) index at baseline (BL) and follow-up (FU), shown as N (%)
Immediate post-embolization angiograms showed that complete occlusion (RRGS I) was achieved in 141 of 243 aneurysms (58.0%) while a neck remnant (RRGS II) persisted in 53 (21.8%) and residual sac (RRGS III) was observed in 51 (21.0%). The LVIS/LVIS Jr group was associated with the lowest rate of complete occlusion (RRGS I: 47.9%; 35/73) but the highest rate of neck remnant (RRGS II: 27.4%; 20/73).
DSA imaging follow-up of the 208 aneurysms showed RRGS I in 166 (79.8%), RRGS II in 15 (7.2%), and RRGS III in 27 (13.0%). From procedure to baseline, the proportion of RRGS I increased for all stent groups compared with initial angiographic occlusion. The variation trend of RRGS I is shown in figure 1, with the greatest increase from 47.9% to 81.7% in the LVIS/LVIS Jr group. Figure 2 depicts an illustrated case. The EP group had the lowest rate of complete occlusion on follow-up DSA imaging (RRGS I: 72.9%; 35/48).

Variation trend of Raymond–Roy Grade Scale (RRGS) I of stent groups. EP, Enterprise; LVIS, Low-profile Visualized Intraluminal Support; NEU, Neuroform.

{kind=link}
{kind=link}
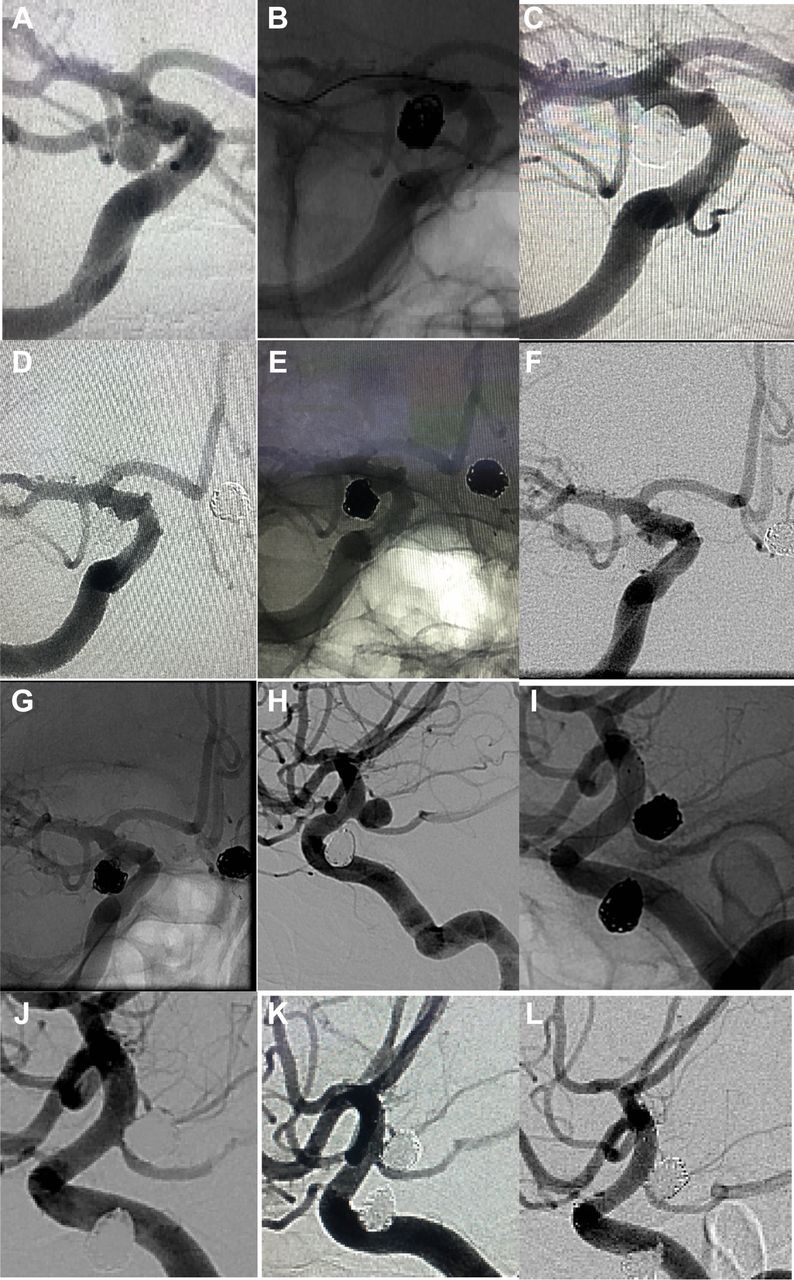
A middle-aged patient presented with incidental bilateral posterior communicating artery aneurysms. (A) Angiogram of right internal carotid artery shows a right posterior communicating artery aneurysm measuring 5.1 mm x 4.2 mm with a 1.9 mm neck. (B) Native angiogram of the right internal carotid artery obtained during coiling treatment with the balloon-assisted technique by use of a Scepter SC 4×10 mm to avoid coil protrusion. (C) Post-treatment lateral subtracted right internal carotid angiogram showing neck remnant (Raymond–Roy Grade Scale (RRGS) II). (D) Angiogram of right internal carotid artery performed 6 months after coiling, showing the neck filling. (E) Control native angiogram showing the coils compressed mildly. (F) Follow-up imaging at 36 months after coiling shows recurrence of the right posterior communicating artery aneurysm (RRGS III). (G) Control native angiogram of the right internal carotid artery shows coils compressed obviously. (H) One week after the right posterior communicating artery aneurysm coiling (A–C), left posterior communicating artery aneurysm, measuring on lateral angiogram 5.6 mm x 5.5 mm with a 2.9 mm neck, was scheduled for treatment with stent-assisted coiling. (I) Post-treatment native view in the working projection showing a compact coil mass within the aneurysm and the LVIS Jr stent (4.5 mm x 16 mm) is well-opposed to the parent vessel with no in-stent thrombosis or flow limitations. (J) Subtracted view in the working projection shows there is still filling around the margin of the aneurysm sac (RRGS III). (K) Angiogram of left internal carotid artery performed 6 months after coiling showing complete aneurysm occlusion (RRGS I). (L) Subtracted view after 36 months confirms complete occlusion.
Recurrence
Nineteen aneurysms showed recurrence on follow-up angiograms of 208 aneurysms, of which 3/60 (5.0%) were in the LVIS/LVIS Jr group, 9/100 (9.0%) were in the NEU group, and 7/48 (14.6%) were in the EP group. During subsequent follow-up, 15 were stable while 4 showed coil compaction or sac enlargement and were retreated (table 3). This resulted in an overall retreatment rate of 1.9% (4/208 aneurysms).
Distribution of recurrence at follow-up, represented as N
Complications
Seventeen intra-procedural complications were seen in 229 patients (7.4%) and 15 post-procedural complications were found in 198 patients at follow-up (7.6%). There was an association between stent type and procedure-related complications as well as between stent type and post-procedural complications (table 4), which was not statistically significant. A higher proportion of intra-procedural complications was found in the LVIS/LVIS Jr stent group while a higher proportion of post-procedural complications was found in the EP stent group.
Relationship between patient characteristics and stent type and procedure-related or post-procedural complications
Complications are shown in table 5. Intra-procedural rupture occurred in four patients, two from wire perforation (4/229, 1.7%). The rupture was from the aneurysm in four patients and wire perforation in two patients Two patients had permanent disabling neurologic deficit (mRS ≥2). The other two recovered with minor residual neurologic defects (mRS <2).
Distribution of complications at baseline and follow-up, represented as N (%)
Thrombosis complications (stent-related events) occurred in 13 patients (13/229, 5.7%). The rate of stent-related thrombosis events (major in 3 patients, minor in 10 patients) was higher in the LVIS/LVIS Jr group (7/69, 10.1%) than in the EP and NEU groups. There were eight thrombosis events not related to the stent (minor in all patients), seven in the NEU group and one in the EP group. These stent-unrelated thrombosis events were caused by coil protrusion into the parent artery during bare or balloon-assisted coiling, which were considered unrelated to stent deployment as the stent was used in a rescue fashion. Overall, complications occurred in 15 patients during clinical follow-up which included three major strokes (3/198, 1.5%), five minor strokes (5/198, 2.5%), and seven in-stent stenosis (7/198, 3.5%), of which only three (3/198, 1.5%) displayed evidence of ≥50% stenosis.
Among intra-procedural complications, there were no significant differences between the stent groups (p=0.088) (table 6). Logistic regression analysis showed that EP was associated with an increased risk of postoperative complications with an OR of 6.153 relative to LVIS/LVIS Jr and 3.563 relative to NEU. LVIS/LVIS Jr was assoicated with fewer postoperative complications than NEU, although the difference was not statistically significant (table 7).
Results of multivariable repeated measures mixed-effects logistic regression for intra-procedure related complications
Results of multivariable repeated measures mixed-effects logistic regression for post-procedure related complications
Discussion
Stent-assisted coiling has been shown to be safe and effective in the treatment of complex cerebral aneurysms with an unfavorable neck.2–8 11 12 Intracranial stents have undergone several generations of improvements since the first description by Higashida et al 3 regarding their use in 1997; however, there are limited data on long-term efficacy and safety. A comparative analysis among the three generations of stents does not exist. We studied these three generations of devices with respect to technical and neurological complications and aneurysm occlusion rates on initial and follow-up imaging.
Neuroform (NEU)
NEU, the first generation self-expanding coil-assist stent with an open-cell design, received FDA approval in 2002. Since then, it has undergone multiple iterations including NEU 2, Treo, NEU 3, NEU EZ, and NEU Atlas.
In this study the NEU group showed lower rates of intra-procedural complications with a rate of rupture events (2/102) and stent-related thrombotic events (4/102), in contrast to reports in the literature.19 20 The literature includes studies across older NEU generations so the existing data may not necessarily represent the performance of the most recent iteration such as NEU EZ or NEU Atlas. In our study, only 20 aneurysms were treated with NEU 3 stents before July 2010, after which all aneurysms were treated with NEU EZ or NEU Atlas which adopted the newest delivery system. There were another seven instances where NEU stents were used in a ‘rescue’ fashion after coils prolapsed out of an aneurysm being treated without a stent (stent-unrelated). All seven patients were discharged without functional impairment (mRS <2).
The NEU group achieved an initial RRGS I in 65.1% (71/109) of patients after stent-assisted coiling and 82.0% (82/100) on follow-up, and was associated with the highest initial and follow-up complete occlusion in the single stent group (figure 1). The open-cell architecture is engineered to enhance wall apposition and to facilitate coil packing density when deployed across an aneurysm arising on the outer convexity of a curved vessel. The open-cell design of the NEU stent has larger apertures through which to navigate than a closed-cell design stent such as the EP. These important nuances between open-cell and closed-cell designs affected the operator’s choice of technology to deploy.7 The ‘coil-through’ technique was adopted in 50.5% (55/109) of patients in the NEU group. One disadvantage of the open-cell design may be less protection against small coil loop protrusion. A telescope configuration was required as rescue in four patients; double NEU stents were used in three patients and in one patient the NEU was followed by an EP stent.
Enterprise (EP)
Since May 2007 when FDA approval was granted, the second generation EP stent has become a staple device for the stent-assisted coiling of wide-necked aneurysms. Our study suggests that EP is safe to use in the treatment of intracranial aneurysms in conjunction with coiling. The EP group showed the smallest proportion of intra-procedural adverse events (table 5). This may be explained by its closed-cell design, ease of delivery, deployment, recapture feature and conformability to tortuous anatomy navigation, which can provide the operator with excellent control and stability once in place. While other authors have reported migration of EP when deployed in vascular segments with significant diameter deviations, this was not observed in our study.21
We did not find any covariates to be independently associated with post-procedural complications after controlling for stent type although, at a mean angiographic follow-up of approximately 15.9 months, four patients (4/45, 8.9%) displayed evidence of in-stent stenosis and four patients (4/45, 8.9%) experienced a stroke during the follow-up period in the EP group, suggesting that the risk of in-stent stenosis or thrombotic events was greater with the EP than with the other stents. This finding has recently been attributed to poor wall apposition related to device design and deployment technique.22 23 Moreover, Kim et al 24 reported an in-stent thrombosis rate of 10.2% (4/39) after the deployment of EP stents. Chalouhi et al 25 reported no difference in the risk of in-stent stenosis between EP and NEU stents.
In this study, initial complete occlusion (RRGS I) was achieved in 35 of 61 aneurysms (57.4%) in the EP group. This was similar to the initial complete occlusion rate of 52.8% (1000/1893 aneurysms) found for EP-assisted coil embolization in a literature review.19 Jia et al 26 reported that deployment of EP stents resulted in complete occlusion in 101 of 179 aneurysms (56.4%) while Kim et al 27 showed 77.2% immediate complete occlusion after stent-assisted coiling with EP stents. Moreover, DSA imaging follow-up of 48 aneurysms showed RRGS I in 35 (72.9%) in the EP group, which is similar to the complete occlusion rate at last follow-up reported in a large series of aneurysms coiled with EP stent assistance.19 26 Our data suggest progressive favorable occlusion rates after stent-assisted coiling with the EP stent despite only 10% metal surface coverage. Recurrence occured in 7/48 aneursyms in the EP group (14.6%), which was higher than in other groups. This observation may be related to the higher initial RRGS III in the EP group.
LVIS/LVIS Jr
LVIS and LVIS Jr, the third generation of coil-assist devices, are flexible closed-cell braided microstents approved by the FDA in 2014 for stent-assisted coiling of wide-necked intracranial aneurysms. The braided design potentially permits greater conformability, stability, and apposition to the vessel wall. In addition, LVIS Jr can be delivered through lower profile 0.017 inch microcatheters.13 21 The ‘jailing’ technique was used in 21/73 (28.8%) LVIS/LVIS Jr cases, more than other groups, although the ‘coil-through’ technique was still the most frequently employed technique, being used in 29/73 cases (39.7%).
A proposed advantage of the LVIS/LVIS Jr stent is that it has a mean metal coverage rate of 20–23% compared with 11% for NEU and 10% for EP, which can facilitate endothelial growth and improve flow diversion. Thrombotic events were more common in the LVIS/LVIS Jr group (7/69, 10.1%) and all cases were successfully treated with intravenous administration of abciximab. Four cases were asymptomatic and two experienced symptomatic thromboembolic complications (mRS ≥2). Telescoping stents have a theoretically higher chance of forming thrombus with more metal in the artery.26 Möhlenbruch et al 14 reported a procedural thrombosis rate of 9% after LVIS deployment and Cho et al 27 observed that 7.4% (4/54) of cases suffered procedural thrombotic events.
LVIS/LVIS Jr provides better flow diversion and may promote aneurysm delayed thrombosis, leading to a more complete rate of occlusion (figure 2). Although immediate angiographic results demonstrated relatively lower rates of initial RRGS I of 47.9% (35/73), progression to total occlusion was greatest with a high RRGS I rate of 81.7% (49/60) at follow-up imaging (figure 1). Fiorella et al 21 reported that the progression to complete occlusion with the LVIS device was particularly dramatic, with initial RRGS I in only 17% increasing to 75% at the 6-month follow-up. Cho et al 27 reported a complete obliteration rate of 92.6% at 6-month follow-up in a series of 55 patients treated with the LVIS device. The delayed thrombosis rate of aneurysm occlusion in our LVIS/LVIS Jr group was superior to that in the NEU and EP groups and the recurrence rate with LVIS/LVIS Jr was lower than with the other two stents; however, this is an association only. Although in our study only one case of in-stent stenosis was found, some studies have reported a higher rate of in-stent stenosis with LVIS than with EP or NEU.27 28
Y-stenting
The operators in our center often chose the open-cell design of the NEU as the first stent deployed during Y-stenting because its larger apertures enable it to expand more than a closed-cell design stent. Navigating through the first stent with a large bore microcatheter to deploy the second stent of the construct can be challenging and theoretically result in thrombosis or perforations. In this group, NEU followed by EP was used in all cases. The total complication rate of 33.3% (4/12) was the highest of all groups and was statistically significant in the univariate analysis (p=0.01) at the patient level. This is likely to be associated with a number of factors including the higher level of complexity of the treated aneurysm as well as more metal coverage.
Limitations of study
First, this study did not take into consideration the effect of coil packing density which may contribute to the rates of aneurysm occlusion and recurrence. Second, since thromboembolic events were the major intra-procedural complication, platelet function tests or thrombocyte inhibition levels should be used to adjust the protocol of antiplatelet therapy, although this area remains controversial. Platelet function studies were not part of our clinical practice during the study period.
Conclusions
All three types of stent were safe, feasible, effective, and reliable options for stent-assisted coiling of wide-necked or complex intracranial aneurysms. LVIS/LVIS Jr can achieve better progressive aneurysm complete occlusion but the rate of intra-procedure thrombosis was not negligible. The long-term efficacy and safety of the LVIS/LVIS Jr need to be evaluated in future studies.
References
Footnotes
Contributors Design and revising of the work: AT. Drafting the work and analysis, interpretation of data: JW. Acquisition of data: JV, AS, IC, RDT, JL. Final approval of the version to be published: AT. Agreement to be accountable for all aspects of the work: all authors.
Competing interests AS: Penumbra: Consulting, Honorarium, Speaker Bureau; Pulsar Vascular: Consulting, Honorarium, Speaker Bureau; Microvention: Consulting, Honorarium, Speaker Bureau, Research; Stryke:r Consulting, Honorarium, Speaker Bureau. RDT, AT, IC: Codman: Consulting, Honorarium, Speaker Bureau, Research funding; Covidien: Consulting, Honorarium, Speaker Bureau; Penumbra: Consulting, Honorarium, Speaker Bureau, Research grants; Microvention: Consulting, Honorarium, Speaker Bureau, Research grants; Blockade: Stock, Consulting, Honorarium, Speaker Bureau; Pulsar Vascular: Stock, Consulting, Honorarium, Speaker Bureau, Research; Medtronic: Consulting, Honorarium, Speaker Bureau.
Ethics approval Medical University of South Carolina IRB.
Provenance and peer review Not commissioned; externally peer reviewed.