Article Text

Abstract
Background Despite several retrospective studies analyzing the safety and efficacy of transradial access (TRA) versus transfemoral access (TFA) for cerebral angiography, this transition for neurointerventional procedures has been gradual. Nonetheless, based on our positive initial institutional experience with TRA for mechanical thrombectomy in acute ischemic stroke patients, we have started transitioning more of our cerebral angiography cases to TRA. Here we present our single institution experience.
Methods We performed a retrospective review of patients receiving TRA cerebral angiography at our institution between January 2016 and February 2017. We present our experience transitioning from TFA to TRA, including our criteria for patient selection, technical nuances, patient experience, complications, and operator learning curve.
Results We included 148 angiograms performed in 141 people by one of four operators. No major complications were observed, and the technical success of the procedures was consistent with those of TFA. Marked improvement in operator efficiency was achieved in a short number of cases during this transition when looking at operator proficiency as a function of angiograms performed and days of exposure to TRA (4.3 vs 3.6 min/vessel, P<0.05).
Conclusions Safety and efficiency can be preserved while transitioning to TRA. While further investigation is necessary to support transition to TRA, these findings should call for a re-evaluation of the role of TRA in catheter cerebral angiography.
- angiography
- endovascular
- radial
- stroke
- transradial
- thrombectomy
Statistics from Altmetric.com
Introduction
The past two decades have seen a shift from transfemoral access (TFA) to transradial access (TRA) in the field of interventional cardiology.1 This is largely due to data demonstrating a reduction in access site complications; however, other benefits such as decreased length of stay, reduced hospital costs, and improved patient satisfaction have also been shown.2 3 In the US, this has resulted in approximately 40% of cardiology procedures being performed via TRA, a number that continues to increase every year. The transition is even more pronounced in Europe and Japan, where transradial adoption is in excess of 80%.1 In 2013, three of the largest societies for interventional cardiology in Europe issued a joint guideline formally recommending radial access as the first choice for cardiac procedures, especially percutaneous coronary intervention for ST elevation myocardial infarction, after multiple large trials (ie, Radial vs Femoral Access for Coronary Intervention (RIVAL), Radial Versus Femoral Randomized Investigation in ST Elevation Acute Coronary Syndrome (RIFLE), etc) showed not just decreased access site morbidity but actually a mortality benefit to TRA over TFA.4
TRA for cerebral angiography has seen slower adoption, despite several prior retrospective studies demonstrating both the technical feasibility and safety of this approach.5–9 In fact, a large single institution study of 154 patients from Matsumoto et al 7 found that TRA was less invasive and a safer procedure for selective cerebral angiography compared with TFA or transbrachial techniques. The overall hesitance in implementing TRA for cerebral angiography may be due to a variety of factors: TFA dominates much of the current neurointerventional training, and there is a perceived difficulty in navigating the cerebrovasculature from the radial artery. Nonetheless, centers across the country have begun utilizing TRA to access the cerebral vasculature. One multicenter trial, which included our institution, found that between 0.3% and 4.5% of patients underwent TRA for mechanical thrombectomy for acute ischemic stroke depending on hospital.10 Based on our positive initial experience with TRA for thrombectomy as previously described, we have begun transitioning more of our cerebral angiography cases to TRA.10 11
Here we present our initial experience transitioning from the traditional TFA to a ‘radial first’ approach for diagnostic angiography, including our criteria for patient selection, technical nuances, learning curve, patient experience, and complications. Furthermore, we sought to provide a unique step by step guide for neurointerventionalists by outlining our transradial practice: from room set-up to hemostatic technique.
Methods
Study design
After receiving institutional review board approval, we retrospectively analyzed our institutional database of consecutive catheter cerebral angiograms performed via TRA between January 2016 and February 2017. Patient demographics, procedural and radiographic metrics, and clinical data were recorded.
Patient selection
All patients underwent pre-procedure assessment of collateral palmar circulation via Barbeau testing.12Patients with no return of pulse tracing following 2 min of radial artery compression (‘Barbeau D’) were excluded from TRA, and instead received TFA. Although we did not track patients who tested Barbeau D, we know from the cardiology literature that historically 4% of patients are classified in this way.12 13 Any patients requiring additional intervention past angiography were excluded from this study. Furthermore, patients <18 years of age, those with a history of trauma or surgery to the ipsilateral arm, and those with known anatomic variants or arterial occlusion or stenosis in the ipsilateral arm were also excluded.
Room setup
The right arm is placed at the patient’s side with the distal forearm and hand in a slightly supinated position (approximately 45o). Full supination of the wrist is not necessary and often causes the wrist to be positioned farther away from the hip, which can be problematic in two ways. The lateral plane may hit the radial arm board once it is brought into position. Additionally, if the wrist separates significantly from the hip, a space is created and any equipment in the proximity can slide down off the patient. For these reasons, it is imperative to keep the wrist tight against the hip of the patient, and slight pronation of the wrist, rather than a full supination, allows this position (figure 1). We also place several towels under the forearm to elevate it to the level of the hip so the catheters can rest on the thigh rather than falling down to the side (figure 1). The puncture site just proximal to the wrist crease is therefore held in close proximity to the standard location of transarterial access, the common femoral artery. The standard transfemoral room setup, patient orientation, and catheter work are thus preserved. We also use a wrist splint to hold the wrist in slight extension, which brings the radial artery to the surface and provides gentle tension in the overlying skin and connective tissue, facilitating needle puncture.

Graphic of the room setup, with wrist positioning, in order to perform radial/brachial bifurcation angiography. The table is rotated clockwise 15° to enable visualization of the right forearm with a monoplane setup to take anteroposterior fluoroscopic images.
Similar to TFA, access is obtained with only the anteroposterior (AP) plane in position and the lateral plane not yet in place. In order to perform angiography of the radial/brachial bifurcation and confirm access, the angiography table is rotated clockwise approximately 15° to enable visualization of the right forearm with a monoplane setup to take AP fluoroscopic images (figure 1). After the sheath has been placed and the guide system has been advanced to the subclavian artery, the angiography table is returned to the neutral position, and the lateral collimator is brought into position.
Transradial access technique
The right radial artery was used for all cases, except in cases where the left vertebral artery (LVA) was the only vessel to be catheterized, in which case left-sided radial access was used. In the preoperative holding area, topical 2.5% lidocaine/prilocaine cream is applied to the radial artery area in the wrist and forearm, and covered with an adhesive dressing to keep it in place for 15–30 min prior to the start of the procedure.
The radial artery area is then sterilized and draped with a radial catheter drape. The peri-arterial tissue is infiltrated with lidocaine, and the radial artery is cannulated using a 20 g needle via an anterior or counterpuncture technique according to operator preference.14 Ultrasound guidance for radial access has been shown to improve the success and speed of cannulation, is also employed according to operator preference.15 We tend to use ultrasound from the outset if the radial pulse is faint or absent or after two unsuccessful attempts at accessing the radial artery. A 5 F or 6 F Glidesheath introducer sheath is then placed over an 0.025 inch hydrophilic guidewire (Terumo Medical, Somerset, New Jersey, USA). A radial artery angiogram is performed through the sheath to include a view of the brachial bifurcation, and antispasmodic agents (verapamil 2.5 mg and nitroglycerine 200 ug) are administered through the sheath prior to introducing the guide catheter. The agents are diluted in 20 mL of blood lavaged from the sheath to prevent discomfort during injection. The patient is then systemically heparinized with 70 units/kg administered intravenously.
Navigating to the subclavian
Depending on the anatomy seen with the radial artery angiogram, a 5 F Simmons 2 Glidecath catheter is then navigated over an 0.035 inch soft Glidewire into the ipsilateral subclavian artery, taking care to avoid aberrant anastomotic connections between the major arteries of the forearm and brachium. The navigation of the forearm and brachium is done under live AP fluoroscopy, with the bed at a 15° counterclockwise rotation. As the catheter and wire are navigated into the brachium, the angiography table is moved towards the operator, bringing the brachium into view. If the initial radial artery angiogram demonstrates tortuosity or a loop, roadmap guidance is employed to facilitate safe navigation and avoid radial artery spasm (RAS). Loops that are felt to be difficult to pass with an 0.035 inch wire are navigated with a microcatheter system, usually with an 0.018 inch wire that will often straighten out the loop. Once subclavian access has been obtained with the micro system, the guide catheter is navigated into position. Once in the subclavian artery with the diagnostic catheter, the table is returned to its neutral position and the lateral plane can be brought into its standard cerebral angiography position.
Reforming the Simmons 2 from the arm
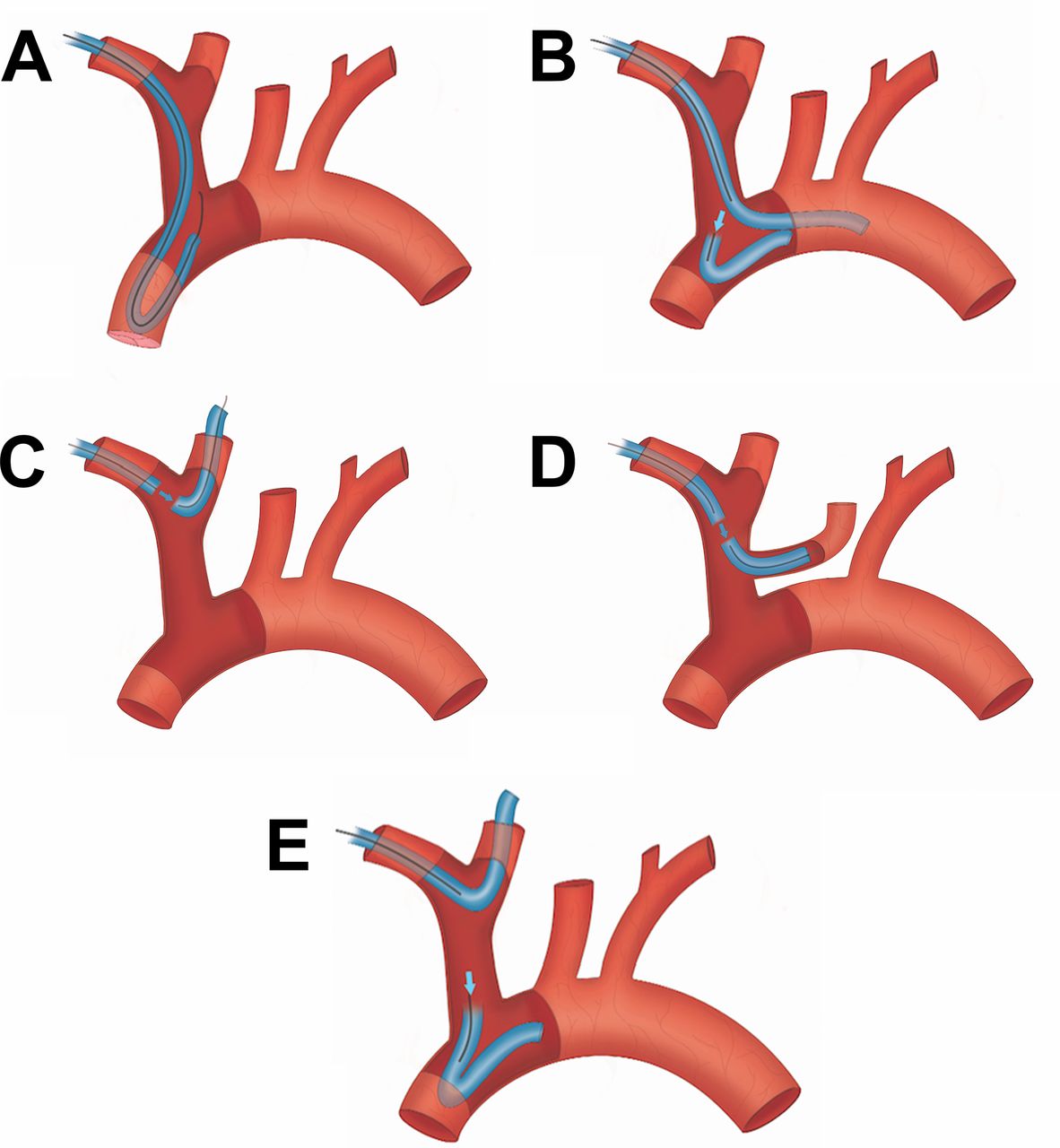
We have found that the Simmons 2 catheter offers the broadest ability to catheterize almost any anatomy, and so we use it for the vast majority of our cases to access the great vessels. There are multiple ways to reform the Simmons curve prior to vessel selection. The most reliable way is simply to form it off of the aortic valve in an identical fashion to forming it off of the valve from the TFA approach (figure 2A).
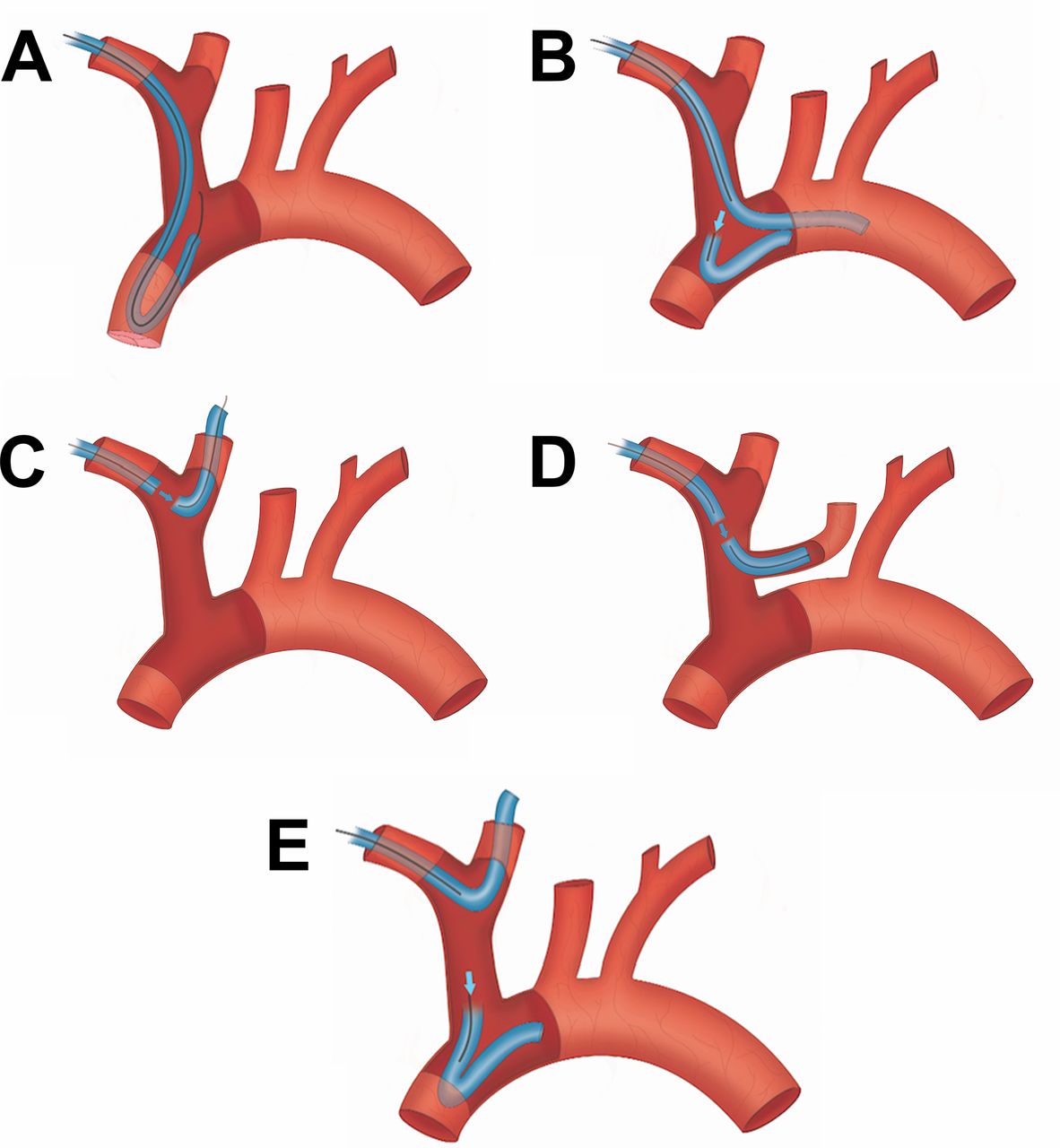
Catheter configurations for navigating the aortic arch vasculature. We find the Simmons 2 catheter to be preferable, and it can be formed (A) off the aortic valve or (B) in the arch itself (see technique discussion). Often times the right common carotid artery (RCCA) or left common carotid artery, if bovine arch variant, can be catheterized directly (C, D). Finally, if the Simmons 2 is desired in the formed state in the aortic arch after catheterization of the RCCA, it can be reformed by positioning the catheter over the ostia of the RCCA. As the system is pushed forward, the catheter is formed (E).
However, we prefer a more nuanced way of reforming the reverse curve by accessing the descending aorta from the innominate artery when possible. By combining the curve of the glidewire with the distal curve of the catheter, the wire can often be directed over the arch into the descending aorta. The catheter is then tracked partially over the wire into the descending aorta until the secondary curve is positioned over the ascending aorta. The wire is then retracted to a position proximal to the secondary curve to allow for more support, and the entire system is pushed forward. With the distal catheter positioned in the descending aorta, forward advancement causes the secondary curve to herniate into the ascending aorta, thus reforming the reverse curve of the Simmons catheter (figure 2B). We attempt to reform the catheter using this technique first, and if the aorta is too capacious or too unfolded to access the descending aorta with the glidewire, we then reform it off the aortic valve.
Lastly, often the right common carotid artery (RCCA), and even sometimes the left common carotid artery (LCCA) depending on the vascular anatomy, can be cannulated directly without the need for a Simmons curve (figure 2C and figure 2D). If the Simmons is then desired in its formed configuration, the secondary curve can be positioned over the ostia of the RCCA, and the system can be pushed forward. The secondary curve will then herniate into the innominate and subsequently the aortic arch, allowing for the placement of a formed Simmons catheter in the aorta to select the LCCA (figure 2E).
Selection of the great vessels
In TRA, selection of the great vessels—once the catheter has been navigated to the subclavian artery—proceeds in an order determined by the patient’s specific anatomy. Initially, it is prudent to gently advance the soft tip glidewire towards the innominate artery with the angled tip directed superiorly to select the RCCA. Often the wire will be seen to advance directly up into the RCCA. The catheter is then advanced into position in the RCCA. A roadmap of the cervical bifurcation can be performed, and the internal and external carotid arteries are accessed in the standard over the wire fashion. In approximately 15% of patients who have certain bovine-type configurations, the glidewire can be directed safely into the proximal LCCA directly from a catheter positioned in the proximal subclavian artery without the need to enter the aorta or reform the Simmons 2 catheter.
After the right internal carotid artery (RICA) angiogram has been performed, the catheter is then retracted in the manner described above such that the proximal curve of the Simmons 2 is positioned at the RCCA origin with the wire positioned at the proximal curve and the catheter is then pushed into the aorta in its formed state. Selection of the LCCA and LVA are then performed in the same way as with a Simmons catheter from a TFA approach.
In many cases, the glidewire cannot be navigated directly into the RCCA or LCCA from the subclavian artery. In these situations, vessel selection proceeds with formation of the Simmons curve in the aorta using one of the techniques described in the previous section. Once the Simmons shape has been formed, the catheter tip is directed superiorly and while intermittently ‘puffing’ contrast with a hand injection, a twisting of the catheter with retraction pulls the tip toward the origin of the great vessels and the ostia are engaged in a manner identical to that used with the TFA approach. Once the origin is engaged with the catheter tip, the glidewire can be advanced into the common carotids or more distal branches and the catheter can be brought into the desired position. We recommend roadmap guidance with the later plane disarticulated to center on the cervical bifurcation while maintaining the AP plane centered on the aortic arch to simultaneously observe the distal catheter and wire while monitoring the proximal catheter in the aorta in case it herniates out into the arch, in an identical fashion to the TFA approach.
Selective angiography of the posterior cerebrovasculature can be performed via catheterization of the left subclavian and subsequently LVA from the aortic arch with the catheter formed as mentioned previously. The right vertebral artery (RVA) is selected with the Simmons catheter but in its unformed state, and as such is best catheterized at the beginning or end of the angiogram. Following completion of the angiogram, the diagnostic catheter is removed.
Closure: patent hemostasis technique
Patent hemostasis refers to the technique of holding the bare minimum amount of pressure needed for hemostasis, and no more. This allows for the artery to remain open while still maintaining hemostasis, rather than aggressively clamping down on the arteriotomy. This later technique also achieves hemostasis, but at the cost of occluding the vessel. The patent hemostasis technique has been well documented to improve radial artery occlusion (RAO) rates through the Prevention of Radial Artery Occlusion—Patent. Hemostasis Evaluation Trial (PROPHET) and PROPHET-II studies.16 17 A radial armband (Terumo, Somerset, New Jersey, USA) is first secured 1–2 cm proximal to the point of arteriotomy and inflated. The sheath is then removed with the band inflated. The band is then slowly deflated until oozing is seen from the puncture site. At this point, a small amount of air is reintroduced to the band to re-achieve hemostasis (thus with the minimal amount of pressure required). Following this, with a pulse oximeter attached to the patient’s index finger, the ulnar artery is compressed manually and the pulse wave monitored (‘reverse Barbeau test’). If radial artery patency is confirmed with a persistent waveform in the presence of a compressed ulnar artery, the patient can be transitioned to the recovery area.
If radial artery patency is not confirmed, compression of the ulnar artery can be continued while maintaining patent hemostasis with the band and pulse oximeter in place, and this sequence is often effective at re-establishing patency.18
Post-procedure
Patients receive assessment of both radial artery patency and hemostasis in the recovery area every 15 min with nurses who had received in-service training with the hemostatic wristband. Thirty minutes after the band is initially placed, 3–5 mL of air are removed from the band at each assessment. This process is repeated until the band is completely deflated, at which point it is removed and a non-compressive sterile dressing applied. Should bleeding be encountered after deflation, the band is re-inflated for an additional 30 min before resuming deflation. All patients were discharged 90 min after closure.
Patient preference and experience
Telephone interviews were conducted for all patients. All elective angiography patients were assessed in the postoperative period within 2 weeks of their procedure via telephone, and all inpatients were assessed following discharge via phone call in the postoperative period prior to the follow-up visit. Patients were asked to describe access site pain, as well as arm pain, in the week following the procedure (ranked as none, mild, moderate, or severe). In addition, patients were asked to report any previous experience with TFA (yes or no). Finally, patients were asked about access site preference for a subsequent angiographic procedure (prefer radial, prefer femoral, or no preference).
Learning curve
In order to quantify the learning curve associated with a transition to a TRA approach, we defined operator efficiency as minutes of total fluoroscopy time divided by the number of supra-aortic vessels catheterized for each angiogram. Vessels included the common carotid artery, internal carotids, external carotids, and vertebral arteries. Thus total fluoroscopy time for a procedure that included angiograms from the right common, left internal, and left external carotid arteries would be divided by 4 to calculate the efficiency metric because both common carotids, and the left internal and external carotid arteries, were catheterized.
A learning curve was then determined by comparing procedural efficiency for each of the four operators between their initial and subsequent performance (group 1: angiograms #1–5; group 2: angiograms #11–15). Additionally, each fellow’s experience was assessed longitudinally over the course of their training to encompass increases in technical ability that are acquired by performing interventional procedures and experiential learning not captured by these data.
Statistical analysis
We performed statistical analyses regarding operator proficiency as a function of angiograms performed via TRA. Data are presented as mean and range for continuous variables, and as frequency for categorical variables. Calculations of normality were carried out by ladder of powers and calculations of variance by Levene’s test. Continuous data were assessed before and after a median number of angiograms in each fellow using the Wilcoxon matched pairs signed rank test. Linear regression analysis was used to determine the effect of increasing number of angiograms on outcome, as mentioned above. A P value ≤0.05 was considered statistically significant. Statistical analysis was carried out using STATA software, V.14 (College Station, Texas, USA).
Results
Procedure
A total of 148 angiograms were performed in 141 patients during the study period. The radial artery was successfully catheterized in 99.3% (147/148) of patients. The preplanned great vessels of interest were successfully catheterized in 98.6% of cases. In two cases, the left internal carotid artery (LICA) could not be selectively catheterized, with crossover to TFA occurring in one case and LCCA angiography alone used in the other.
Procedural complications
No major complications were seen. Minor complications were seen in 6.75% of cases (n=10), including six patients with RAS and associated forearm pain during the procedure, one patient with minor RAS in the forearm necessitating microcatheter and microwire navigation, one patient with severe RAS in the forearm necessitating crossover to TFA, one patient with persistent forearm pain treated with oral steroids, and one patient with inadvertent catheterization of the anterior interosseous artery requiring crossover to TFA. Radial artery patency measured by reverse Barbeau test at discharge was 100%.
Crossover to TFA
Seven cases (4.7%) required crossover to TFA. Four patients were found to have an aberrant origin of the right subclavian artery, also known as arteria lusoria. The anterior interosseous artery was inadvertently catheterized in one patient. In another, RAS recalcitrant to antispasmodic medication was encountered. In one patient, the LICA was unable to be catheterized successfully due to significant LCCA tortuosity. In each case, the sheath was removed, and a transradial compression band applied to achieve patent hemostasis. TFA was obtained and the cerebral angiogram was completed. Following the procedure, no clinical sequelae or complications were noted.
Selective vessel catheterization
Selective vessel catheterization was performed frequently: the RICA was selected in 69.5% of cases, LICA in 48.7%, RVA in 71.3%, LVA in 23.4%, right external carotid artery in 24.3%, and left external carotid artery in 19.1%.
Learning curve
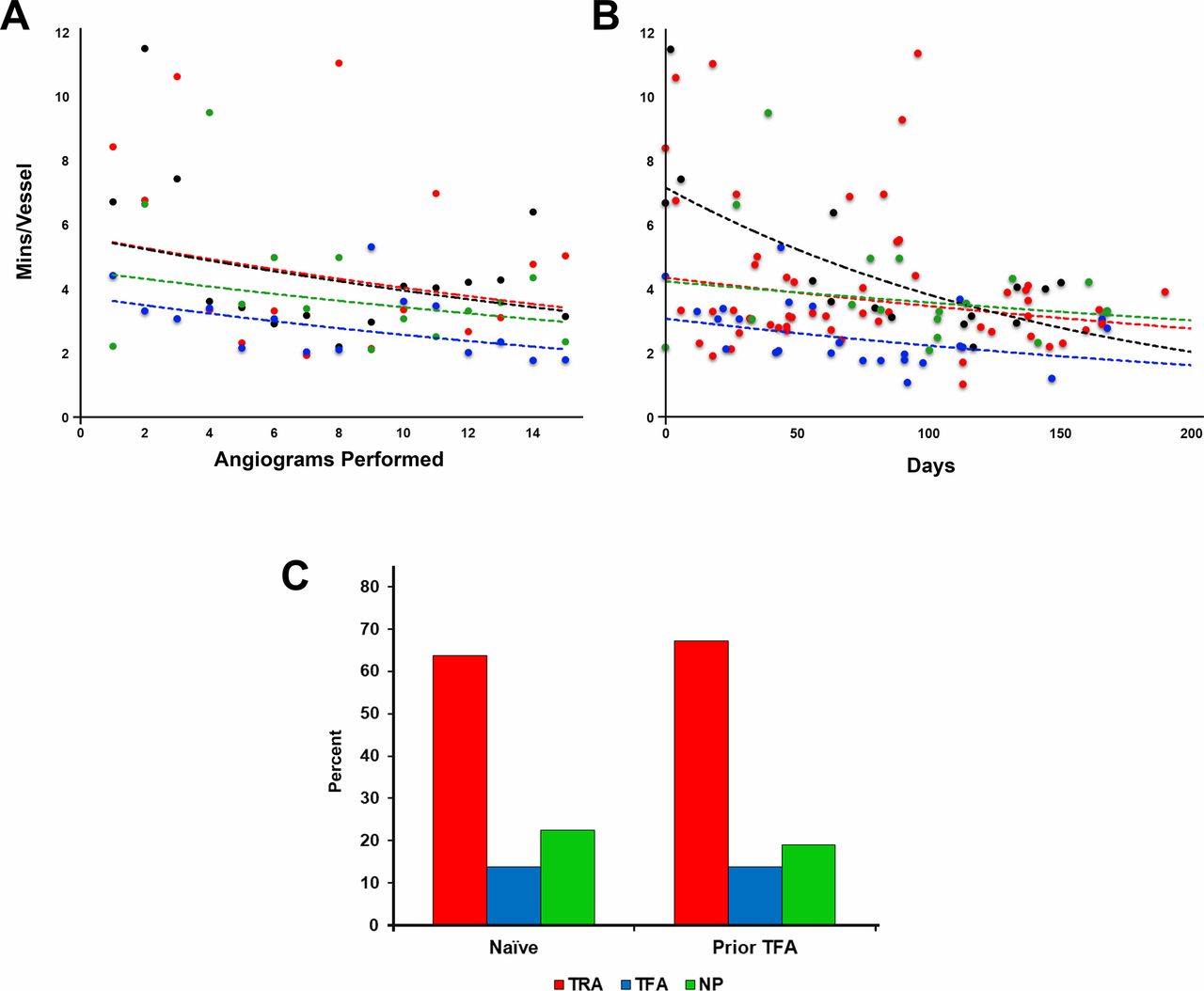
Overall, 16.2% improvement in procedural efficiency was observed between group 1 and group 2 (4.3 vs 3.6 min/vessel, P<0.05), consistent among all fellows. Longitudinal efficiency plots for each fellow by number of angiograms performed, and days from initial exposure, are shown in figure 3A and B, respectively, with accompanying exponential regression trend lines.

Learning curving efficiency plot: operator efficiency in transradial arterial access (TRA) improves as a function of (A) angiography performed and (B) days after initial exposure to the technique. Patients new to cerebral angiography and those having undergone neurointervention in the past also prefer TRA to the transfemoral access (TFA) approach (C). NP, no preference.
Patient satisfaction
Telephone interviews were successfully conducted with 80 patients in the postoperative period. A total of 86.2% of patients reported ‘none’ or ‘mild’ wrist discomfort following the procedure, while 93.7% of patients reported ‘none’ or ‘mild’ arm and shoulder discomfort. A total of 58 of 80 patients (72.5%) had undergone prior TFA. Of patients who had experienced both TRA and TFA previously, 67% (39/58) would prefer transradial access for their next procedure, with 13% (8/58) preferring TFA, and 11 declaring no preference (figure 3C).
Discussion
In the cardiology literature, the benefits of TRA compared with traditional TFA have been well documented.19 Additionally, TRA for cerebral angiography has been described in several retrospective series and shown to be safe and effective.2 4–6 Nonetheless, use of the transradial approach as the primary method of performing cerebral angiography has not been widely adopted. There are several obstacles to transitioning a cerebral angiography practice to TRA, including familiarity with access and vessel selection, and concerns over safety and technical feasibility of transition to practice. Future studies may be needed to compare TFA and TRA not only in terms of access site complications, but also in terms of radiation exposure to the patient and operator, contrast use, neurological complications, hospital cost, nursing workload, patient preference and patient experience, and recovery time. However, the lessons learnt in our experience adds neuro-specific pearls in addition to the extensive cardiac data on the radial approach.20
Safety of TRA
No major complications (ie, hand ischemia, RAO, access site hematoma, neurological injury) were seen in our series. There was a minor complication rate of 6.75% (10/148). Eight of 10 patients experienced RAS, a known minor complication of TRA. We found RAS, evidenced radiographically or clinically, in 4.8% of patients, consistent with the known 6–10% prevalence in patients treated with antispasmodic medications.1 RAS was successfully treated in six patients with further administration of intra-arterial antispasmodics until it had resolved angiographically and clinically, with only one patient requiring crossover to TFA due to RAS.
RAS and RAO are access site complications unfamiliar to neurointerventionalists, and their prevalence is often cited as an obstacle to transitioning to TRA. While it is imperative to properly manage RAS if it occurs, RAO is considered a more significant problem as its presence precludes the possibility of future percutaneous radial interventions. However, it is important to stress that RAO has almost no clinical consequence. Unlike more proximal access techniques, such as brachial which as an end artery has a known significant risk of limb ischemia, hand ischemia from a radial catheterization for cardiac or neurointervention is case reportable. There is also a misconception about the incidence of RAO, due to heterogeneity in closure techniques in published series. The prevalence of RAO has been noted to be anywhere from 0.8% to 33%, but RAO prevalence with modern patent hemostasis techniques, including ulnar compression, ishas consistently been found to occur in <1% of patients.17 21 In the present study, we have demonstrated that by implementing modern prevention strategies adopted from cardiology, such as the patent hemostasis technique, much of the perceived access site risk can be eliminated. This is in stark contrast with femoral access morbidity, which not only includes ischemia, but also a small, yet non-zero, mortality risk from the access itself. This can be from the rare massive retroperitoneal hematoma but also from initially non-fatal but significant bleeding, as shown in multiple trials that demonstrate a mortality benefit to the radial approach.22 23
Patient selection to maximize safety benefit
While the demonstrated improved safety profile of TRA applies to most patient groups, there are clearly patients that can reap more of a safety benefit from TRA. As expected, these are patients that the traditional TFA has been shown to carry an increased access risk, including obese patients, patients taking anticoagulants, and the elderly.12 24–26 We would also include pregnant patients in this group. Transradial angiography moves the site of access site away from the groin and gravid uterus, decreasing radiation exposure to the fetus during access and navigation of the descending aorta. The abdomen of pregnant patients can even be covered with a lead shield to further decrease radiation exposure. There are also patients whose femoral anatomy favors an alternative approach, such as significant atherosclerotic disease of the distal aortic or common femoral arteries or even with bypass or femoral stents in place. Once we developed enough expertise to become facile with the radial approach, these higher risk patients are now universally done via the radial approach. Additionally, many patients are ideal candidates for TRA due to favorable arch anatomy, to be discussed further subsequently. Box describes the clinical characteristics we find to favor TRA.
Clinical and anatomical considerations for the different vascular approaches
Clinical characteristics favoring transradial access
Patients on oral anticoagulants22
Obese patients23
Elderly patients
Pregnant patients
Patients with peripheral arterial disease
Prior surgery or intervention to aorta, iliac, or femoral arteries, or inguinal area
Patients in whom early mobility is important (ie, athletes, patients with low back pain, hereditary or acquired thrombophilias, etc)
Anatomical characteristics
Favors transradial access
Bovine aortic arch
Posterior circulation selective angiography
Type III aortic arch
Favors transfemoral access
Arteria lusoria
Tortuosity of proximal common carotid arteries
Vessel selection
Despite its improved safety profile, TRA is of little use if the great vessels cannot be catheterized. Thus we were keen to investigate the ability to access the supra-aortic vessels via TRA. Starting with which radial artery to access, the right radial artery was the preferred access site for the majority of neurovascular procedures in our series. Catheterization of the right radial artery and navigation into the right subclavian artery affords relatively straightforward access to the RVA, RCCA, and LCCA. The LVA can usually be catheterized from the right radial if all vessels are required, but can be challenging, so if a primary LVA catheterization is desired, we prefer to access via the left radial artery. If the right radial artery is used and the LVA is unable to be catheterized with a Simmons 2 shape, a Simmons 3 shape with its longer distal limb makes catheterization of the LVA straightforward.
Using a Simmons 2 glide catheter, successful selective vessel catheterization was achieved in 100% of cases of the RICA and RVA, and in 98% of cases of the LICA. These rates are similar to what has been previously reported for cerebral angiography via TRA. Previous studies evaluating TRA for cerebral angiographies have also found that selective catheterization can be reliably performed using a Simmons 1 or 2, 5 F catheter (Cook).6 27 Rates of successful selective catheterization of the RICA and RVA were shown to be >95% while the LICA was catheterized successfully in approximately 84% of cases. We found the smaller caliber of the radial, brachial, and subclavian arteries provides excellent catheter support compared with the more capacious iliac arteries and thoracic aorta.
Anatomic factors
While neurointerventionalists have extensive experience with aortic and supra-aortic anatomy, several anatomic nuances are specifically germane to procedures performed via TRA that deserve mention.
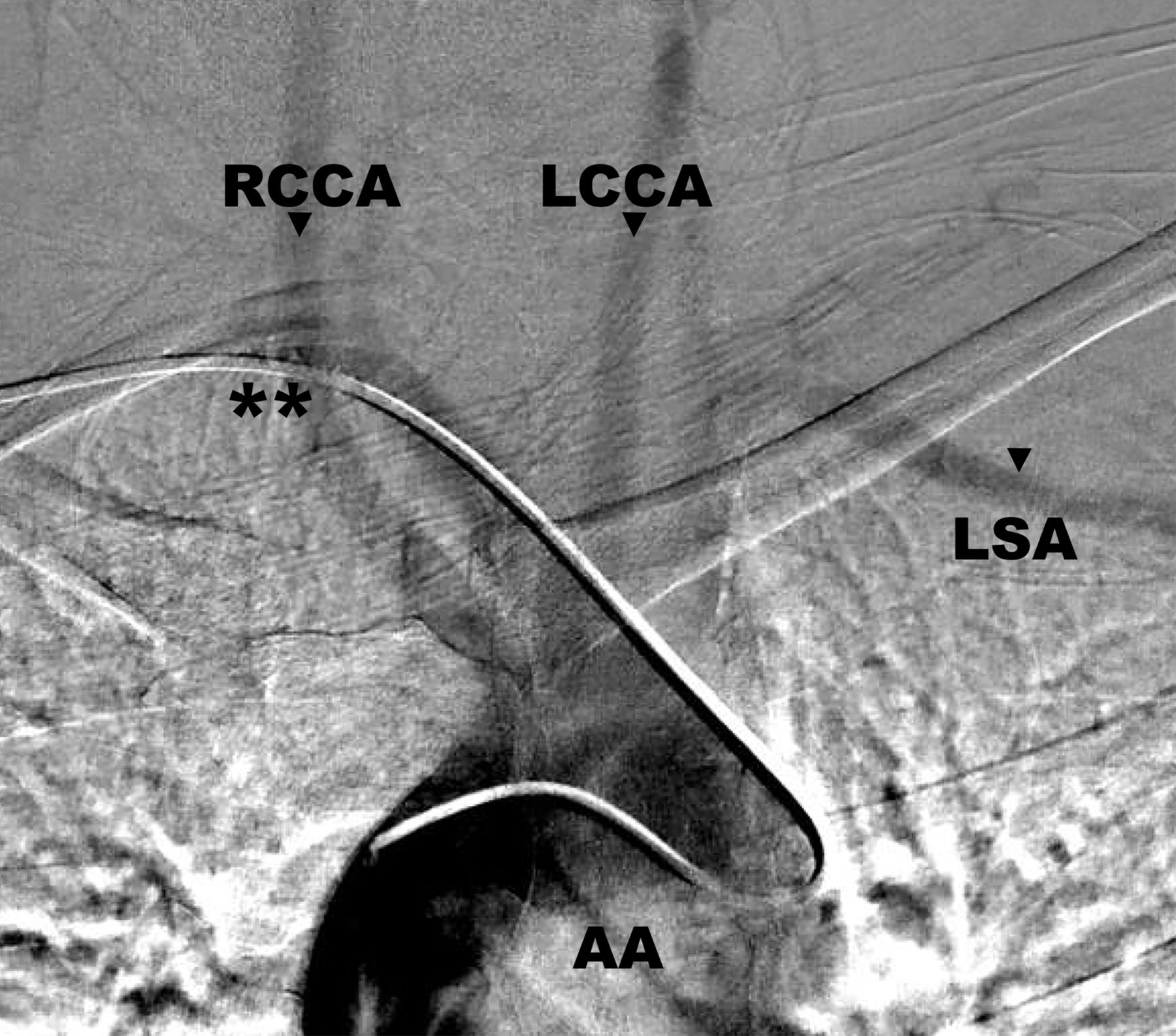
Arteria lusoria
Arteria lusoria refers to an anatomic variant where the right subclavian artery arises as the fourth branch from the aorta, instead of the first (figure 4). In addition, the RCCA arises as the first branch directly from the aortic arch. We encountered this variant in four patients (2.8%). We found this variant greatly increases the technical challenge of performing TRA for catheter cerebral angiography of all vessels but the RVA. Each case encountered in our series required crossover to TFA to complete the angiogram. The prevalence of arteria lusoria ranges from 0.6% to 1.4%, although it is present in 26–34% of individuals with Down syndrome or other chromosomal abnormalities.28 From our experience, the presence of this anatomic variant should be considered a contraindication to TRA.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Angiogram depicting arteria lusoria, where the catheter navigates through the right subclavian artery as it arises as the fourth branch from the aorta (astericks). AA, aortic arch; LCCA, left common carotid artery; LSA, left subclavian vein; RCCA, right common carotid artery.
Bovine aortic arch
In contrast with arteria lusoria, a bovine configuration aortic arch, where the innominate artery and LCCA share a common origin, is an anatomic variant that allows for direct catheterization of the LCCA without needing to enter the aorta. We have consistently found a bovine arch configuration to be significantly easier to catheterize via TRA than the traditional transfemoral approach. The common origin frequently allows for selection of the LCCA directly without the need to form the Simmons 2 catheter in the aortic arch.
Aortic arch type
The presence of an elongated or tortuous aortic arch, such as a type II or III aortic arch, often presents difficulty with catheterization of arch vessels from a transfemoral approach.29 We have found that these aortic arch configurations present a more direct vessel catheterization from a transradial approach, especially of right-sided vessels and the LCCA/LICA with a bovine arch variant, as there is often no need to enter the aortic arch.
The presence of a type III arch, however, does occasionally create difficulty in forming the Simmons 2 catheter in the descending aorta, our preferred method of formation. The more inferior innominate artery origin in these patients, relative to a type I arch, creates difficulty in selecting the descending aorta with the wire, and usually necessitates catheter curve formation using a common carotid artery or ascending aorta method. Box outlines the pertinent anatomical considerations when deciding between TRA and TFA.
Learning curve
Technical prowess in performing angiography can be difficult to assess. Technical success of the angiogram is typically determined by the quality of images and successful catheterization of relevant arteries in combination with safe practice to avoid complications. In our series, technical success was achieved in 98.6% of cases, thus making traditional measures of a learning curve impractical to assess. We believe that operator efficiency improves as familiarity with catheter and access techniques increases. Therefore, this overall metric was a natural choice for evaluating the learning curve associated with performing TRA. We chose minutes of fluoroscopy time per vessel catheterized, as it is a robust measure of operator efficiency and could reasonably be expected to decrease as operators became more familiar with the individual steps associated with catheter placement. Additionally, because all operators had previous experience with transfemoral techniques, there were no significant concerns for confounders, such as excess fluoroscopy time during non-essential parts of the procedure.
Based on this metric, we found an improvement in efficiency within the first 15 angiograms performed by each operator, which was not associated with any increase in complication rate. Our data demonstrate that efficiency can be improved within a relatively short experience without sacrificing safety.
Unfortunately, it is difficult to make a direct comparison with transfemoral techniques using the same metric by virtue of the technical differences in catheter placement. As discussed above, there are clearly anatomical factors that favor TRA over TFA when it comes to efficiency. However, we would empirically argue that, on balance, TRA diagnostics appear to take slightly longer to perform than diagnostics done via TFA.
Patient experience and preference
TRA was preferred in a majority of our patients, especially those who had undergone prior TFA. In addition, a majority of our patients experienced little to no discomfort at the access site or in the arm following the procedure. These findings echo similar results found in neurovascular patients undergoing TRA. Satti et al interviewed 25 patients who had undergone both TRA and TFA previously and found that 96% of patients preferred TRA for their next procedure.30 Furthermore, these findings are similar to access site preference data from the cardiology literature, with documented preference rates from 71% to 90% in patients who had experienced both TRA and TFA.31–33
The reason for TRA preference in our patients likely mirrors what has been shown previously in the cardiology literature, where decreased rates of overall discomfort, back pain, and difficulty with ambulation are seen with TRA.33 Our patients are able to sit in bed immediately after the procedure and can ambulate, with assistance, to the restroom with the hemostatic band in place during their stay in the recovery area. In addition, a shorter stay in recovery also enhances patient experience. All patients were discharged after 90 min of observation, compared with 4 hours for TFA at our institution. Furthermore, TRA moves the procedure away from the inguinal region, a delicate area in most patients, to the much less sensitive wrist. Patients who have received prior TFA are especially mindful of these issues, which are likely the cause of the TRA preference.
Study limitations
While these results are generalizable, there are some limiting factors of importance. First, we are constrained by the limitations of the retrospective design of our study—namely, in the ability to discern subtle complications in the postoperative period. We made efforts to prevent significant recall bias by following up with our patients in a timely manner after their procedures, although we are unable to ascertain all potential complications. For example, there are data in the cardiology literature to suggest the possibility of superficial radial nerve injury due to TRA in 1.8% of patients, which manifests as hand pain, numbness, or weakness.34 We did not specifically include this in our surveys at the time of data collection.
Second, we utilized a metric to determine learning curve (ie, minutes of total fluoroscopy time divided by number of supra-aortic vessels catheterized for each angiogram) that had not been previously described or validated in the literature. Nonetheless, we feel this metric is acceptable to assess the learning curve in TRA, as much of the training in the radial approach revolves around formation of the Simmons 2 catheter and then navigating to a specific target vessel. These two steps require continuous fluoroscopy time, so therefore, if operators use less fluoroscopy time, then it indicates more efficient formation of the Simmons 2 curve and then vessel selection.
Finally, we were only able to capture approximately 60% of our initial cohort for the post-procedural survey. Our capture rate reflects the challenges in obtaining adequate follow-up in patients who received a diagnostic angiogram during an emergent hospitalization as opposed to an elective admission. Additionally, the capture rate ultimately reflects the difficulties in contacting the patient population seen at our home institution more so than our inability to capture a higher percentage of patients.
Technical pearls of transradial access
Apply topical lidocaine/prilocaine to the puncture site in the preoperative area. It increases patient comfort, reduces access site pain, and facilitates easier access.
Make sure the wrist is positioned close to the hip rather than out from the body. In addition to ensuring that the lateral plane can be brought into the field, this also prevents the catheters from sliding down the leg of the patient. Elevating the wrist and forearm on towels to bring it to the level of the surface of the leg is also beneficial.
Apply subcutaneous lidocaine on either side of the radial artery in the wrist to help stabilize the artery for puncture, and minimize ‘rolling.’
Have a low threshold to use ultrasound to access the radial artery. While it seems cumbersome, it has actually been shown to lower time to access for TRA. Ultrasound is immediately available for all TRA procedures at our institution, and the senior author mandates it for all his radial cases to lower time to access.
Dilute the antispasmodic cocktail by aspirating blood into a 20 mL syringe from the introducer sheath prior to gentle infusion over 1–2 min to decrease patient discomfort associated with calcium channel blocker infusion.
If resistance is encountered during standard pulling or pushing of the catheter, suspect spasm in the forearm or brachium and administer antispasmodics through the sheath. Also, benzodiazepines can be administered intravenously to help reduce muscle tension in the affected arm.
In cases where there is significant peripheral arterial atherosclerosis or narrowing in the arm, a microwire can be used to safely pass through the distal stenosis and bring the diagnostic catheter into the larger caliber brachial artery. Consider using an exchange length BMW microwire (Abbott, Chicago, Illinois, USA) and downsizing to a 4 F diagnostic catheter system.
It is surprising how often the guidewire goes directly into the RCCA or even the LCCA from the innominate artery. Always probe gently with the guidewire to determine the anatomy.
While re-forming the Simmons curve via the descending aorta is clearly the more elegant technique, have a low threshold to form it off of the aortic valve if the wire will not direct down the descending aorta. Some arch anatomies preclude this navigation and we have found forming it off the aortic valve to be simple, fast, and safe.
Most importantly, as one of our fellows was told at a cardiac radial access course: "If you want to be successful, you cannot dabble in radial access". It does take time and some commitment to get over the learning curve. Once surmounted, however, TRA is surprisingly simple to perform.
Conclusion
During this initial experience with the transradial approach, no major complications were observed, and the technical success of the procedures was consistent with the traditional transfemoral approach. Thus we have demonstrated that safety and technical outcomes can be preserved while transitioning to a primarily transradial approach. Furthermore, we have shown that marked improvement in operator efficiency can be achieved in a short number of cases during this transition. Finally, we found that patients experience little to no wrist or arm discomfort with the radial approach, and those that are familiar with both TRA and TFA overwhelmingly prefer TRA for their next procedure. These findings, when taken in the larger context of the safety benefit seen in cardiology from TRA, should call for a re-evaluation of the role of TRA in catheter cerebral angiography. Whether this feasibility can be extrapolated to complex neurointervention remains to be seen.
References
Footnotes
BMS and SS contributed equally.
Contributors All authors contributed to the conception, data gathering, and drafting of the manuscript. RMS performed the statistical analysis. RMS, DRY, and ECP provided manuscript oversight and administrative support. All authors critically reviewed the manuscript and approved its final submission.
Competing interests None declared.
Ethics approval The study was approved by the institutional review board of the University of Miami Miller School of Medicine, Miami, Florida, USA.
Provenance and peer review Not commissioned; externally peer reviewed.