Article Text

Abstract
Background Despite advances in revascularization tools for large vessel occlusion presenting as acute ischemic stroke, a significant subset of clots remain recalcitrant to current strategies. We assessed the effectiveness of a novel thrombectomy device that was specifically designed to retrieve resistant fibrin rich clots, the geometric clot extractor (GCE; Neuravi, Galway, Ireland), in an in vitro cerebrovascular occlusion stroke model.
Methods After introducing fibrin rich clot analogues into the middle cerebral artery of the model, we compared the rates of recanalization between GCE and Solitaire flow restoration stent retriever (SR; Medtronic, Minneapolis, Minnesota, USA; control group) cases. A maximum of three passes of each device was allowed. If the SR failed to recanalize the vessel after three passes, one pass of the GCE was allowed (rescue cases).
Results In a total of 26 thrombectomy cases (13 GCE, 13 SR), successful recanalization (Thrombolysis in Cerebral Infarction score of 2b or 3) was achieved 100% of the time in the GCE cases with an average of 2.13 passes per case. This rate was significantly higher compared with the Solitaire recanalization rate (7.7%, P<0.0001) with an average of three passes per case. After SR failure (in 92% of cases), successful one pass GCE rescue recanalization was achieved 66% of the time (P<0.005).
Conclusion Application of the GCE in this experimental stroke model to retrieve typically recalcitrant fibrin rich clots resulted in higher successful recanalization rates than the SR.
- flow diverter
- stroke
- thrombectomy
- technique
- technology
Statistics from Altmetric.com
Introduction
Several prospective randomized trials have recently demonstrated the marked superiority of stent retriever assisted mechanical thrombectomy with standard intravenous tissue plasminogen activator (IV tPA) thrombolysis over medical therapy (IV tPA) alone for revascularization of acute ischemic stroke in patients presenting with proximal large vessel occlusion.1–5 The performance of mechanical thrombectomy devices and the efficacy of tPA vary according to the composition and characteristics of the occluding thrombus. Occlusions involving fibrin rich thrombi are more difficult to recanalize, often requiring a greater number of passes with the device than thrombi with higher red blood cell content.6 Clot analogues7 8 have been developed to replicate a range of clot types reported in the stroke literature. The most fibrin rich end of the spectrum in these analogues has been correlated with clot retrieved from clinically challenging cases and subsequently analyzed, thus enabling a relevant re-creation of highly challenging occlusions in vitro. A three-dimensional printed in vitro cerebrovascular occlusion model of stroke has been previously used to test different thrombectomy approaches9 10 and the effectiveness of new thrombectomy devices.11 In the present study, we evaluated a novel clot retriever device, the geometric clot extractor (GCE; Neuravi, Galway, Ireland), by comparing its effectiveness for thrombectomy of fibrin rich clots with that associated with the Solitaire flow restoration stent retriever (SR; Medtronic, Minneapolis, Minnesota, USA) in this occlusion model.
Methods
Device description
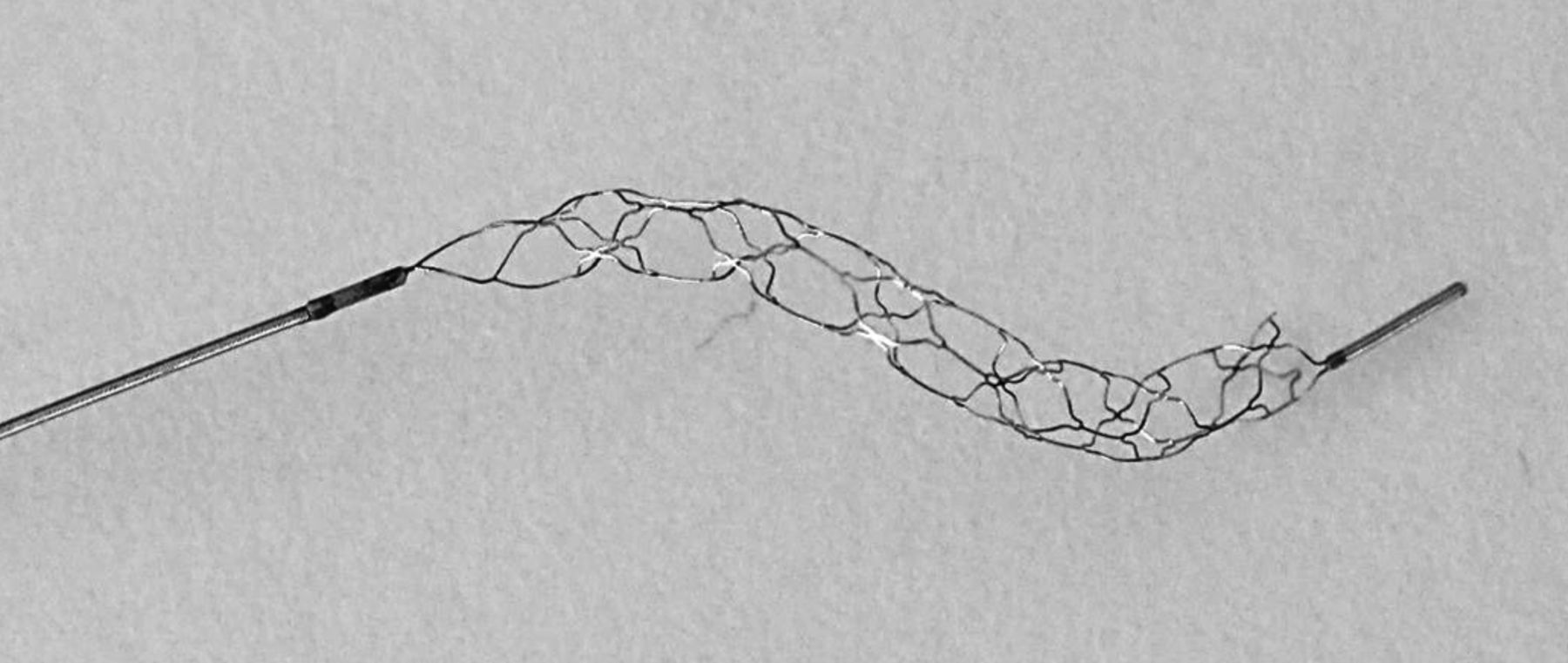
The GCE (figure 1) is a novel proprietary thrombectomy technology specifically tailored to meet the challenge presented by organized fibrin rich thrombus. The GCE device consists of a laser cut nitinol stentriever connected to a nitinol shaft. The tubular portion of the stentriever device has a diameter of approximately 2.0 mm and is formed into a curved spiral configuration to improve clot engagement without exerting excessive radial force, while the laser cut pattern has been designed with optimized cell parameters to engage the clot and to maximize microcatheter assisted grip on resistant clots. The device has a proximal radiopaque coil and an atraumatic distal radiopaque tip for fluoroscopic visibility.

Optical photograph of a geometric clot extractor (GCE; Neuravi, Galway, Ireland). The GCE device consists of a laser cut nitinol stentriever connected to a nitinol shaft. The device has a proximal radiopaque coil and an atraumatic distal radiopaque tip for fluoroscopic visibility.
This device is delivered through a 0.021 inch microcatheter and is passively deployed. Deployment was within the target occlusion by retraction of the microcatheter, in a similar manner to that for a stent retriever, such as the SR, and consistent with our current institutional practice. On deployment, the unique multiplanar geometry of the GCE is specifically engineered to provide definite engagement with the clot and facilitate dislodgement of resistant clots from the vessel. The individual cells are configured to deeply engage the clot. Immediately after deployment, due to the unique device geometry, controlled readvancement of the 0.021 inch microcatheter to the clot results in a strong grip (microcatheter assisted grip activation). The readvancement force required is noticeably increased when engaging clot with the GCE; once the clot is gripped, the microcatheter and GCE are withdrawn together as a system into the proximal cervical guide catheter.
Model description
The design and manufacturing of the three-dimensional in vitro model of the intracranial circulation used for our thrombectomy experiments has been previously described in detail.12 The model closely resembles the human intracranial circulation and consists of the internal carotid artery segment and middle cerebral artery branches (M1–M4 segments), bilateral A1 anterior cerebral artery segments connected to a single anterior cerebral artery, and a single posterior communicating artery (right side), thus allowing near complete circle of Willis circulation.
The model was connected to a pulsatile pump (Masterflex; Cole-Parmer, Vernon Hills, Illinois, USA). Water heated to 37°C was circulated through the model using a peristaltic pump. The rate of flow into the full neurovasculature model was set at 590 mL/min, which is in the upper range of clinically representative flow rates.13
The resistant fibrin rich clot analogues were produced from ovine blood based on the methodology described by Duffy et al.7 Briefly, ovine blood was anticoagulated using sodium citrate solution immediately after collection. The whole blood constituents were subsequently separated using centrifugation and the extracted plasma was mixed with the red blood cells (RBCs) in a ratio of 99:1 (ie, 1% RBCs by volume). Coagulation was initiated by the addition of calcium chloride and the clotted material was allowed to mature. The resultant clots consists of approximately 25% RBCs and 75% fibrin. The individual clots were cut to 3.5±0.5 mm×4.0±0.5 mm×10.0±0.5 mm to facilitate M1 occlusion.
Thrombectomy procedures
Thrombectomy was performed using 4mm×20 mm and 6mm×30 mm SRs (control cases) and the Neuravi GCE device (GCE cases). Before performing each test case, contrast media (320 mgI/mL Visipaque (iodixanol); GE Healthcare, Princeton, New Jersey, USA) was injected into the model, and a baseline DSA run was performed to visualize the intracranial vasculature. The clots were introduced into the carotid artery and allowed to migrate in the vessel under pulsatile flow to the target location at the distal M1 segment of the middle cerebral artery. The clots were allowed to stay lodged for an average of 15 min prior to intervention for both SR and GCE cases. Another DSA run was performed to confirm the occlusion location. The clot was crossed using a 0.021 inch or 0.027 inch microcatheter (Rebar 18 or 27; Medtronic) over a 0.014 inch microwire (Traxcess, MicroVention/Terumo, Aliso Viejo, California, USA) via a 088 inch Neuron Max guide catheter (Penumbra Inc, Alameda, California, USA). Both the SR and GCE device were delivered across the occlusion site and deployed using the microcatheter. The SR was allowed to integrate with the clot for approximately 30–60 s before thrombectomy was attempted. For the GCE cases, no integration time was required. To retrieve the clot, the test devices were retracted through the distal internal carotid artery into the Neuron Max guide catheter. To ensure a challenging test environment, no aspiration or flow arrest was used during the dislodgement and retrieval of the clot to the guide catheter in any of the cases. Manual aspiration via the guide catheter was allowed after removal of either device to clear the guide catheter of any thrombus material.
Following each pass, a DSA run with contrast injection was performed to assess whether baseline flow was restored. The primary end point was the ability to achieve successful recanalization, defined as Thrombolysis in Cerebral Infarction (TICI) 2b or 3 restoration of flow with the device within three passes for each test case. In the event of failure after three passes in any case in the control group, the GCE was used once for rescue therapy to retrieve the clot (rescue cases). Rescue recanalization was considered successful if the clot was fully retrieved (TICI 2b or 3) in a single pass.
Analysis
After performing each case, a baseline DSA run, a post-thrombus run, and a final post-thrombectomy run were evaluated by an experienced neurointerventionist to assign TICI flow revascularization grade and embolization in new territory (ENT) and embolization in distal territory (EDT) scores. The rater was blinded to the thrombectomy device used for the cases shown. ENT was defined as emboli observed on post-thrombectomy angiography within previously unaffected territories (ie, where thrombus was not placed). EDT was defined as emboli seen within the territory of the vessel where the thrombus was originally placed.
Figure 2 shows single images from the DSA runs acquired at different stages during a case from the GCE group. The online supplemental figure 1 shows single images from the DSA runs acquired at different stages during a case from the control group.
Supplementary file 1

{kind=link}
![[SP1.jpg]](https://jnis.bmj.com/content/neurintsurg/10/9/907/DC1/embed/inline-supplementary-material-1.jpg?download=true){kind=link}
{kind=link}
Single images from DSA runs acquired at three different stages during the performance of a geometric clot extractor (GCE) case. (A) Baseline run showing the model vasculature before introduction of the clot. (B) Post-thrombus run indicating the location of the occlusion, in this case the superior M2 segment and Thrombolysis in Cerebral Infarction (TICI) 0 score. (C) Post-thrombectomy run showing the amount of recanalization achieved due to thrombectomy compared with the baseline run. In this case, GCE thrombectomy resulted in full recanalization with a TICI score of 3 and embolization in distal territory and embolization in new territory scores of 0.
The Fisher exact test was performed on the final post-thrombectomy run TICI scores for all three groups. P<0.05 was considered statistically significant.
Results
A total of 13 GCE and 13 SR thrombectomy experiments were conducted. Recanalization was rated as successful in 13 (100%) GCE cases, and this rate was significantly higher compared with that for the SR cases (1 (7.7%)), P<0.0001). Among the 12 (92%) SR failure cases when GCE was used as a rescue device, recanalization was rated successful in 8 (66%) cases (P=0.0036). ENT and EDT occurrence were noted in 2 (15%) and 4 (30.7%) SR cases, respectively; in 0 and 1 (7.6%) GCE cases, respectively; and in 1 (8%) and 4 (33.3%) GCE rescue cases, respectively. The results are summarized in table 1. The average number of passes per case was 3 in the SR cases, 2.15 in the GCE cases, and 1 in the rescue cases where only one pass was allowed per protocol.
Radiographic outcomes of thrombectomy experiments
Discussion
The investigators of recent prospective randomized trials in which stent retriever mechanical thrombectomy was used to recanalize large vessel occlusion during acute ischemic stroke have reported final TICI 2b or 3 scores in 60–85% of cases.1–5 14 15 In the Solitaire With the Intention For Thrombectomy as PRIMary Endovascular treatment (SWIFT PRIME) trial, the intervention group exhibited a substantial gain in reperfusion (defined as a Treatment in Cerebral Ischemia score of 2b or 3) of 88% immediately and 83% at 27 hours post-thrombectomy, compared with the medical only treatment group, which exhibited 40% revascularization at 27 hours post tPA.5 In the Extending the Time for Thrombolysis in Emergency Neurological Deficits–Intra-arterial (EXTEND-IA) trial, the percentage of ischemic territory that had undergone reperfusion at 24 hours was greater in the endovascular therapy group (89%) than in the standard tPA only group (34%).2 In a pooled analysis of SWIFT PRIME, Endovascular Treatment for Small Core and Anterior Circulation Proximal Occlusion with Emphasis on Minimizing CT to Recanalization Times (ESCAPE), EXTEND-IA, and Randomized Trial of Revascularization with Solitaire FR Device versus Best Medical Therapy in the Treatment of Acute Stroke Due to Anterior Circulation Large Vessel Occlusion Presenting within Eight Hours of Symptom Onset (REVASCAT), successful recanalization (TICI 2b or 3 representing restoration of blood flow to >50% of the affected territory) occurred in 77% treated with the Solitaire as the only or predominant device.15
Despite the excellent results obtained in the randomized trials and ongoing improvements in procedural efficacy, successful reperfusion (ie, TICI 2b or 3) is not achieved in approximately 20% or more cases.14 In the ESCAPE trial, REVASCAT, and the Multicenter Randomized Clinical Trial of Endovascular Treatment of Acute Ischemic Stroke in the Netherlands (MR CLEAN), revascularization was not successful in 28–41% of patients.15 16 The reason for poor revascularization results is multifaceted. Challenges such as the type of occlusion, nature of the clot, length of the clot, vascular architecture, and patient comorbidities may all play key roles. The presence of vessel tortuosity can further exacerbate the difficulty of addressing these challenging occlusions. Tortuosity can make it more difficult to dislodge the clot, possibly due to the line of force applied to the clot by the stent retriever and the potential for vessel movement and deformation.17
Although in most cases excellent rates of TICI 2b or 3 reperfusion can be achieved using current stent retriever technology, challenging cases remain in which satisfactory reperfusion is not achieved despite several passes and manipulations of the thrombectomy device. The new GCE technology was designed to retrieve clots recalcitrant to recanalization. These resistant clots have been associated with high fibrin composition.8 18
In this study, the performance of the GCE and SR in retrieving fibrin rich clots was compared. A three-dimensional printed, complete circle of Willis bench model with a closed flow loop was used. This model incorporated vessel tortuosity, normal intracranial flow, and a high fibrin clot analogue to study the potential for this technology. No flow arrest or aspiration was used in the study cases to simulate a ‘worst case’ challenging environment in an attempt to replicate some of the conditions affecting the 15–40% of clinical cases in which adequate reperfusion is not achieved. The integration time for cases in which the SR was used was shorter than is typically practiced. The purpose was twofold. First, the shortened integration time may reflect actual clinical scenarios that occur on occasion at our institution and anecdotally at others. Second, no integration time is required for the GCE, and the shorter integration time in SR cases allowed the devices to be compared on a similar platform.
The results from the study demonstrate that the use of the GCE as a primary device was more effective than the SR in retrieving fibrin rich clots (P<0.0001). On average, the number of passes for the GCE cases was 2.15, whereas for the SR (control) cases it was 3, which was the maximum allowed. Among the 12 failure to recanalize cases following SR thrombectomy, GCE rescue achieved successful recanalization in eight cases with only a single additional pass. The observed differences in SR cases were often associated with dislodgement of thrombus in the more tortuous carotid siphon and subsequent re-occlusion of the treatment segment. The unique geometry of the GCE device facilitates microcatheter assisted grip activation of clot. As a result, dislodgement of thrombus in the carotid siphon was not observed at the same frequency as with the SR.
EDT occurrence was observed in four SR cases. In the GCE primary therapy cases, EDT was noted in one case. Among the rescue cases, EDT was observed in four cases and ENT in one case. It should be noted that we treated failure to recanalize following GCE rescue therapy as EDT. These results indicate that the GCE was highly effective in retrieving fibrin rich clots in the in vitro stroke model under challenging flow conditions without adjunctive aspiration.
The GCE technology may have the potential to improve reperfusion rates and reduce the number of passes required in challenging cases, with a likely associated improvement in patient outcomes. Although it may not always be readily apparent at the beginning of a case that an occlusion will be challenging and may be caused by a fibrin rich clot, there are clues that may help in identifying these cases. Patient history, imaging, and the feel of the occlusion when crossing with a guidewire and the microcatheter may all provide indicators of a resistant clot. There is also growing evidence that thrombectomy cases that take more time with a high number of device passes result in less favorable clinical outcomes (modified Rankin Scale scores >2 at 90 days).19 This new technology has the potential to reduce the number of passes required to remove resistant fibrin rich clots and may facilitate the recanalization of some occlusions that currently cannot be removed, with resultant improved outcomes.
A limitation of this study is that all testing was conducted in an anatomically accurate three-dimensional printed in vitro large vessel occlusion stroke model with a single fibrin rich clot analogue to represent what is likely to be a range of conditions and anatomies that make up the challenging 15–40% of cases that have a poor reperfusion outcome. Further analysis could include in vivo studies and the assessment of devices in various anatomical models with a range of clot analogues. Additionally, many stent assisted thrombectomies involve the adjunctive use of mechanical aspiration, and this could account, in part, for some of the disparities seen between the two devices.
Conclusion
Data from our in vitro studies indicate that application of the novel GCE to retrieve typically recalcitrant fibrin rich clots resulted in higher successful recanalization rates than the SR.
References
Footnotes
VSF and SVSN contributed equally.
Contributors Conception and design: AHS, VSF, SVSN, and KMM. Data acquisition: VSF, SVSN, KMM, and LG. Data analysis and interpretation: all authors. Drafting the manuscript: SVSN, VSF, and AHS. Critically revising the manuscript: all authors. Final approval of the manuscript: all authors.
Funding Funding and devices were provided by Neuravi Ltd. Data collection, analysis, and interpretation of results was performed by the authors, independent of company input; and all content is solely the responsibility of the authors.
Competing interests AHS declares the following competing interests: Financial interests: Apama Medical, Buffalo Technology Partners Inc., Cardinal Health, Endostream Medical Ltd., International Medical Distribution Partners, Medina Medical Systems, Neuro Technology Investors, StimMed, Valor Medical; Consultant:Amnis Therapeutics Ltd., Cerebrotech Medical Systems Inc., Cerenovus (formerly Codman Neurovascular, Neuravi, and Pulsar Vascular), CereVasc LLC, Claret Medical Inc., Corindus Inc., GuidePoint Global Consulting, Integra (formerly Codman Neurosurgery), Medtronic (formerly Covidien), MicroVention, Penumbra, Rapid Medical, Rebound Therapeutics Corporation , Silk Road Medical, Stryker, The Stroke Project Inc., Three Rivers Medical Inc., Toshiba America Medical Systems Inc., W.L. Gore & Associates; Principal Investigator/National Steering Committees: Codman & Shurtleff LARGE Aneurysm Randomized Trial, Covidien (now Medtronic) SWIFT PRIME and Solitaire With the Intention For Thrombectomy Plus Intravenous t-PA Versus DIRECT Solitaire Stent-retriever Thrombectomy in Acute Anterior Circulation Stroke (SWIFT DIRECT) trials, MicroVention CONFIDENCE Study and FRED Trial: Flow Diversion Versus Traditional Endovascular Coiling Therapy, Penumbra 3D Separator Trial, Penumbra COMPASS, and INVEST trials, MUSC POSITIVE trial, Neuravi ARISE II Trial Steering Committee; Board Member:Intersocietal Accreditation Committee. (Dr. Siddiqui receives no consulting salary arrangements. All consulting is per project and/or per hour.) All other authors declare no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional data may be made available by contacting the corresponding author.