Article Text

Abstract
Background Cone-beam computed tomography (CBCT) facilitates the acquisition of cross-sectional imaging in angiography suites using a rotational C-arm and digital flat panel detectors. The applications are numerous, including evaluation of implanted devices and localization of cerebrovascular lesions. We present and validate the clinical utility of an alternative fast CBCT acquisition protocol in the context of neurovascular device imaging.
Methods Contrast-enhanced (CE)-CBCT images were acquired using a new 10 s protocol in a phantom head model, swine model, and in patients. The acquisition parameters of both the 10 s and 20 s protocols were exactly the same, except for fewer projections (250 projections in 10 s vs 500 projections in 20 s), resulting in reduced scan time. Image quality was measured quantitatively in a controlled phantom study and qualitatively by blinded reviewers. The latter was performed to assess the image quality of the 10 s protocol pertinent to the device visibility and its apposition to the parent artery.
Results 10 s CBCT images were comparable to 20 s CBCT in both phantom and animal studies. Of the 25 patient images, the reviewers agreed that they were able to discern the flow diverter struts and assess the apposition in all images. The overall rating for all 10 s images was 4.28 on a 5-point scale. No images were rated as less than 3, which was the average diagnostic quality. The ratings were concordant across three blinded reviewers (κ=0.411). Additionally, contrast and spatial resolution between 10 s and 20 s images were similar in non-human models.
Conclusions CBCT images of neurovascular devices can be obtained successfully using a 10 s acquisition protocol. In addition, the 10 s protocol offers faster acquisition, thus allowing its use in awake patients and with an added advantage of lower radiation and contrast dose.
- angiography
- flow diverter
- stent
Statistics from Altmetric.com
Introduction
Cone-beam computed tomography (CBCT) allows the acquisition of cross-sectional imaging in angiography suites using a rotational arm and digital flat panel detectors.1 Contrast-enhanced (CE)-CBCT imaging allows visualization of vessels in three-dimensional space along with surrounding structures such as brain parenchyma and bone.2 The applications of CBCT in neurointervention are numerous, ranging from the evaluation of stents and flow diverters3 to localization of arteriovenous malformations.4 In particular, the superior spatial resolution of CBCT has proved to be beneficial in imaging neurovascular devices such as stents and flow diverters.5
Despite its versatility, there are several limitations to the routine use of CBCT—namely, longer acquisition time, breath-hold during acquisition, and additional radiation exposure. CBCT images acquired on patients not under general anesthesia during follow-up angiographic studies often suffer from motion artifacts and require extensive coaching during acquisition. A faster acquisition of CBCT images would perhaps allow for CBCT imaging in non-cooperative patients along with the added benefits of lower radiation and contrast, without compromising spatial resolution. We present our initial experience of imaging flow diverter stents using an alternative CBCT acquisition, which takes half the time of a conventional CBCT imaging protocol for neurovascular applications.
Methods
Imaging protocol
The conventional CBCT protocol for neurovascular anatomy requires acquisition of projection images in a circular trajectory in approximately 20 s (Siemens AG, Forchheim, Germany; Toshiba Medical Systems, Tochigi, Japan; Philips Healthcare, Best, Netherlands; GE Healthcare, Little Chalfont, UK). In particular, our practice uses a 20 s DR protocol (20 s DR, syngo DynaCT, Siemens AG) consisting of 500 projections, 0.4 degrees/frame acquisition rate, and 20 s acquisition time.
The alternative fast acquisition protocol we evaluated in this paper is a 10 s DR acquisition program (syngo DynaCT, Siemens AG). This imaging protocol consists of 250 projections acquired at an angular increment of 0.8 degrees/frame in 10 s with a 200-degree angular coverage around the patient. For the purpose of comparative analysis, both the acquisitions were performed at 70 Kv, full field of view (48 cm zoom), and 1.2 µGy/frame dose. The only difference between these two protocols is that the 10 s protocol has half the projection images of the 20 s protocol, resulting in shorter acquisition time and lower radiation and contrast dose compared with the conventional 20 s protocol.
Phantom experiment
A phantom consisting of a plastic head model with cerebrovascular anatomy, the Catphan 600 Phantom (The Phantom Labs, Salem, New York, USA) was imaged using a single plane robotic C-arm system (Artis Zeego, Siemens AG) in the preclinical laboratory. A commercially available flow diverter device (Pipeline Embolization Device, Medtronic, Minneapolis, Minnesota, USA) was deployed in one of the vessels in the phantom. CE-CBCT images of the phantom were acquired using 10 s and 20 s protocols by filling the vessels with dilute contrast medium (Omnipaque 300, Iohexol, GE Healthcare, Princeton, New Jersey, USA). Secondary reconstructions around the deployed device were performed and reviewed by the observers. Also, line profile plots along the device outline were computed to compare the gray scale values in both 10 s and 20 s CBCT images.
CBCT reconstructions were performed on the clinical scanner resulting in a matrix of 512×512×391 voxels of size 0.5 mm3. Identical cross-sectional slices were selected in both the volumes and several ROIs were drawn in the background and contrast inserts. Two contrast inserts, with attenuation close to flow diverter density and intra-arterial contrast opacification were assessed using ImageJ software (National Institute of Health, Bethesda, Maryland, USA). The contrast to noise ratio (CNR) for 20 s CBCT acquisition was 6.74 and 19.01 and for 10 s CBCT acquisition was 4.09 and 12.87 for two contrast inserts. Visual inspection of line pair inserts in the phantom by a trained radiologist yielded a visibility of 12 LP/cm for the 20 s CBCT and 11 LP/cm for the 10 s CBCT.
Preclinical experiment
Both 10 s and 20 s protocols were acquired in a porcine model that underwent neurointervention under a protocol6 approved by the Institutional Animal Care and Use Committee. The experimental design was modeled after previous studies of CBCT.7 A flow diverter device was deployed in the carotid artery of the swine. CE-CBCT imaging was acquired on a robotic arm C-arm system (Artis Zeego; Siemens AG) with breathing suspended throughout the scan. A total of 36 mL of iodinated contrast medium was injected using a power injector at the rate of 3 mL/s for the 10 s protocol and 66 mL at the same rate for the 20 s protocol, with an imaging acquisition delay of 2 s for both protocols. Images were reconstructed on a separate workstation and reviewed using thin cross-sectional multiplanar reformatted (MPR) and maximum intensity projection (MIP) to assess the device visibility and apposition.
Clinical evaluation
CE-CBCT images with the 10 s protocol were acquired on a biplane angiographic system (Artis Zee Biplane VC21; Siemens AG) in patients who underwent aneurysm treatment with a flow diverter device as part of the clinical routine. Twenty-five CBCT images from 17 unique patients (16 women, one man, average age 53.1 years) were included in the study under an institution approved protocol (see table 1). Indications included both immediate post-deployment (during the interventional procedure) and follow-up. Of the 25 images, nine were acquired with breath-hold immediately after the flow diverter was deployed while the patient was under general anesthesia. Theoretically, these images do not suffer from any motion artifacts and hence are expected to have superior image quality. Sixteen of the 25 images were acquired during the angiographic follow-up procedure while the patient was awake and coached to hold breath during acquisition. All CBCT images were acquired with contrast administered in the internal carotid artery for a total volume of 36 mL at a rate of 3 mL/s for a duration of 12 s (2 s delay and 10 s acquisition). The injection protocol was kept the same for all phantom, swine, and patient studies.
Summary of scan indications in clinical use
Image rating
Qualitative image analysis was performed on a clinical workstation used for reconstructing and viewing CBCT images in a retrospective fashion. This was performed only for the 10 s acquisition. Ratings were based on the level of image quality, anatomic, and angiographic on a scale of 1–5 (1=poor, non-diagnostic; 2=limited diagnostic value; 3=average, some restricted visibility; 4=good quality, minimal restrictions on visibility; 5=excellent) by fellowship-trained neurointerventional surgeons (SC, PK) and neurosurgery residents who had completed at least 100 diagnostic angiograms (VMS). Image sets were post-processed on a dedicated workstation and viewed in three planes, with windowing capability for the reviewer. Reviewers were allowed to manipulate the images (rotate the axis, zoom in/out) and reformat the images into MPR or MIP format to assess the device coverage at the aneurysm neck and the apposition to the parent artery. Each reviewer was blinded to the protocol used. Similar rating systems have been used previously in rating of CBCT images.8
In addition to the numerical rating for image sets, raters were also asked three clinically relevant questions regarding the images with a ‘Yes/No’ answer:
Are you able to evaluate the device struts?
Are you able to assess the relationship of the flow diverter device to the aneurysm?
Can you assess flow diverter apposition?
These questions were adapted from a previous study that evaluated intracranial stents using CE-CBCT.7
Statistical analysis
Statistical analysis was performed in SPSS (IBM SPSS Statistics for Macintosh, Version 22.0, Armonk, New York, USA). A P value of <0.05 was used as a threshold for statistical significance. Inter-rater reliability was calculated using Fleiss’ kappa. For unequal variances, average ratings were compared with the Mann–Whitney U test.
Results
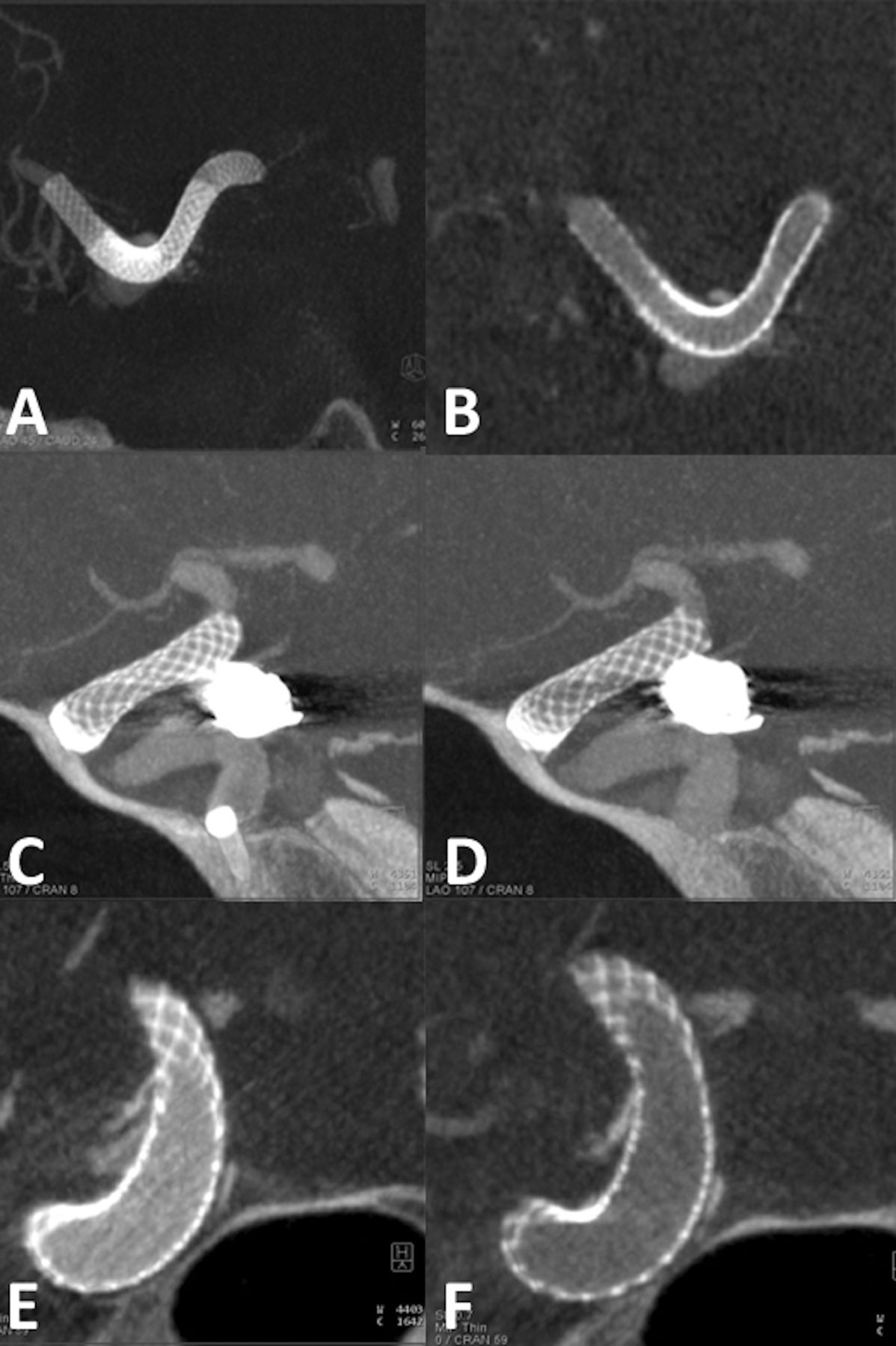
Gray scale value units across a cross-sectional image for 10 s and 20 s CBCT acquisition were comparable in both phantom and swine studies, as shown in figure 1. This is a true comparison of the 10 s protocol with the 20 s protocol as all the parameters were kept constant except for the imaging protocol.

Results from a phantom experiment comparing the 10 s CBCT images with conventional 20 s CBCT. (A) 20 s CBCT cross-sectional maximum intensity projection (MIP) thick (5 mm) slice of the flow diverter deployed in the phantom. (B) 10 s CBCT cross-sectional MIP thick (5 mm) slice of the same flow diverter in the phantom. (C) Volume rendering technique (VRT) rendering of the 10 s CBCT images showing the phantom vasculature and the flow diverter. (D, E) 20 s and 10 s CBCT cross-sectional slice used to compare the gray scale values respectively. (F) Plot of gray scale values along the blue and red lines in (D) and (E). Note that the strut delineation and apposition in the 10 s CBCT is comparable to the 20 s CBCT image and the profile plot of 10 s CBCT matches with the 20 s CBCT image.
An overall average rating of 4.28 was given to the 10 s CBCT images obtained in patients. All images received scores between 3 ‘average’ (11%) to 5 ‘excellent’ (39%). Figure 2 shows example images that received a score of 3 (average), 4 (good), and 5 (excellent). Only two of the 25 images received a score of 3 due to deterioration of image quality from motion artifacts. This included both awake and asleep scans. Asleep 10 s images received a mean rating of 4.48, while awake scans were rated 4.16. No statistically significant difference in the image ratings was observed between the awake and asleep scans (P=0.18). Average ratings per rater were 4.20 for Rater 1, 4.44 for Rater 2, and 4.20 for Rater 3. Inter-rater reliability was used to evaluate the 5-point rating scale, adapted from previous imaging studies. Fleiss’ κ was calculated at 0.411, which was interpreted as moderate agreement among the three raters.9 Pairwise κ between the reviewers was 0.467, 0.438, and 0.333.

Example cross-sectional maximum intensity projection thick images from various cases that received a rating score of 3, 4, and 5 acquired during follow-up procedure with awake patients. (A) 10 s CBCT image of a right para-ophthalmic internal carotid artery aneurysm in a patient. Note the image quality was deteriorated from motion during acquisition. This image was given a rating of 3 by all reviewers. (B) 10 s CBCT image acquired of a right ophthalmic artery aneurysm treated with a flow diverter in a patient. This image was given a rating of 4 by all three reviewers attributed to less sharpness in the depiction of the flow diverter device compared with the conventional 20 s CBCT. (C) 10 s CBCT image of a giant middle cerebral artery aneurysm treated with multiple flow diverter devices and a coronary stent in a patient. This image was rated as 5 by all reviewers attributed to the sharp depiction and delineation of various overlapping stents as well as the vessel apposition.
For all 25 images, the three reviewers could visualize the flow diverter struts and assess its apposition to the parent artery. Furthermore, the reviewers were able to differentiate the strut densities corresponding to single versus overlapping devices. They were also able to identify calcification around the artery in two images. Of the 25 datasets, the aneurysm was already occluded in seven patients and hence question 2 was not applicable. In the remaining 18 images, all three raters were able to assess the relationship of the device to the aneurysm even in the presence of artifacts from coiled aneurysms (six datasets). These assessments are depicted in figure 3.
(A, B) 10 s CBCT cross-sectional maximum intensity projection (MIP) thick (5 mm) and multiplanar reformatted thin (0.6 mm) slices showing overlapping flow diverters deployed in a right middle cerebral artery aneurysm of a patient. Note the varying strut densities at overlapping stents and the single stent depicted by the 10 s CBCT image. (C) Post-interventional 10 s CBCT cross-sectional MIP thick (2.5 mm) slice showing the interface between the flow diverter and coils during the treatment of a residual right posterior communicating artery coiled aneurysm. (D) Cross-sectional MIP thick (2.5 mm) slice of the same patient as in (C) acquired during 6-month follow-up showing the interface between the flow diverter and coils. Note that images (C) and (D) were acquired in asleep and awake settings, respectively and were rated as 4.7 and 4, respectively. (E) 10 s CBCT cross-sectional MIP thin (0.7 mm) slices showing the flow diverter and its interface to the aneurysm as well as the calcification of the artery in a patient who underwent embolization of a right ophthalmic artery aneurysm. (F) 10 s CBCT cross-sectional slice of the same patient as in (E) showing the occluded aneurysm and calcification of the artery.
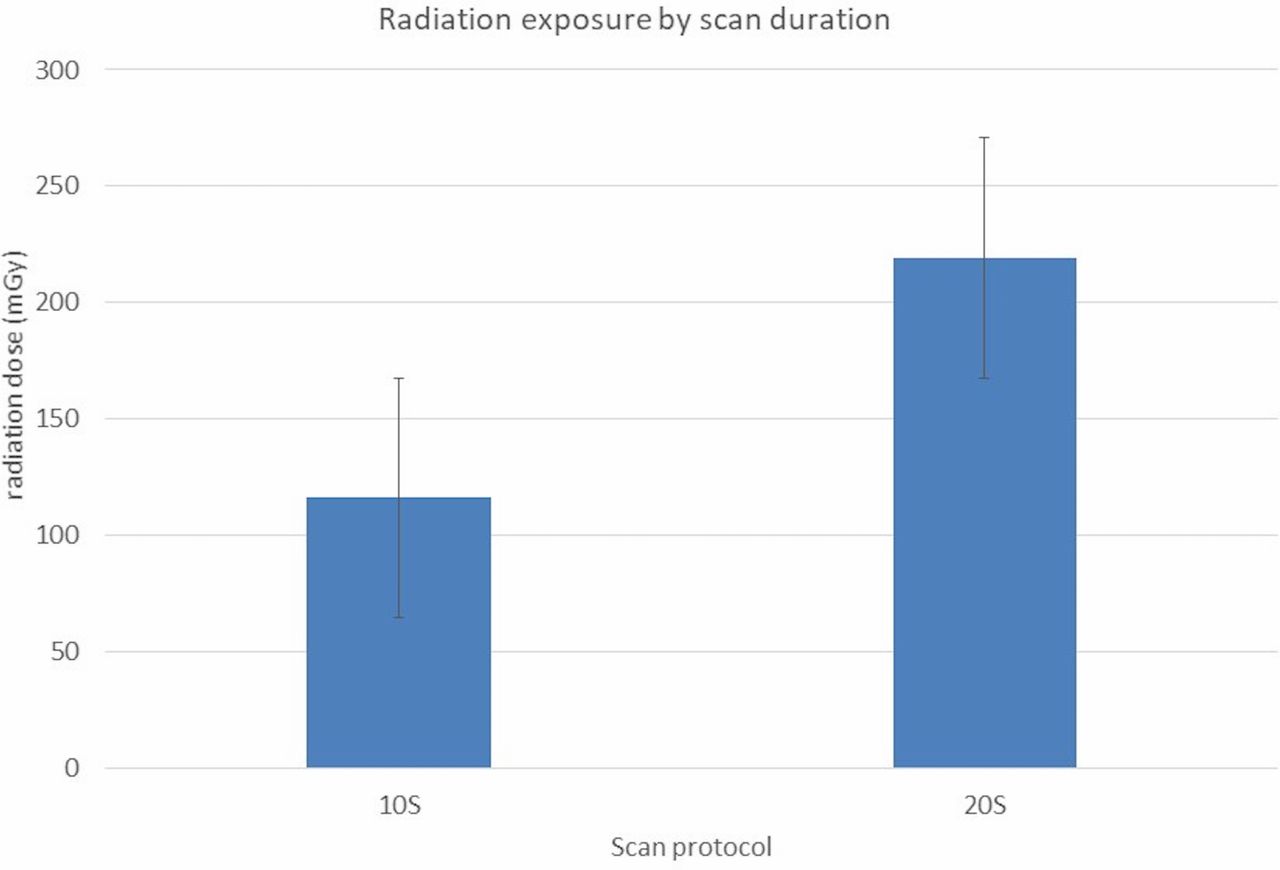
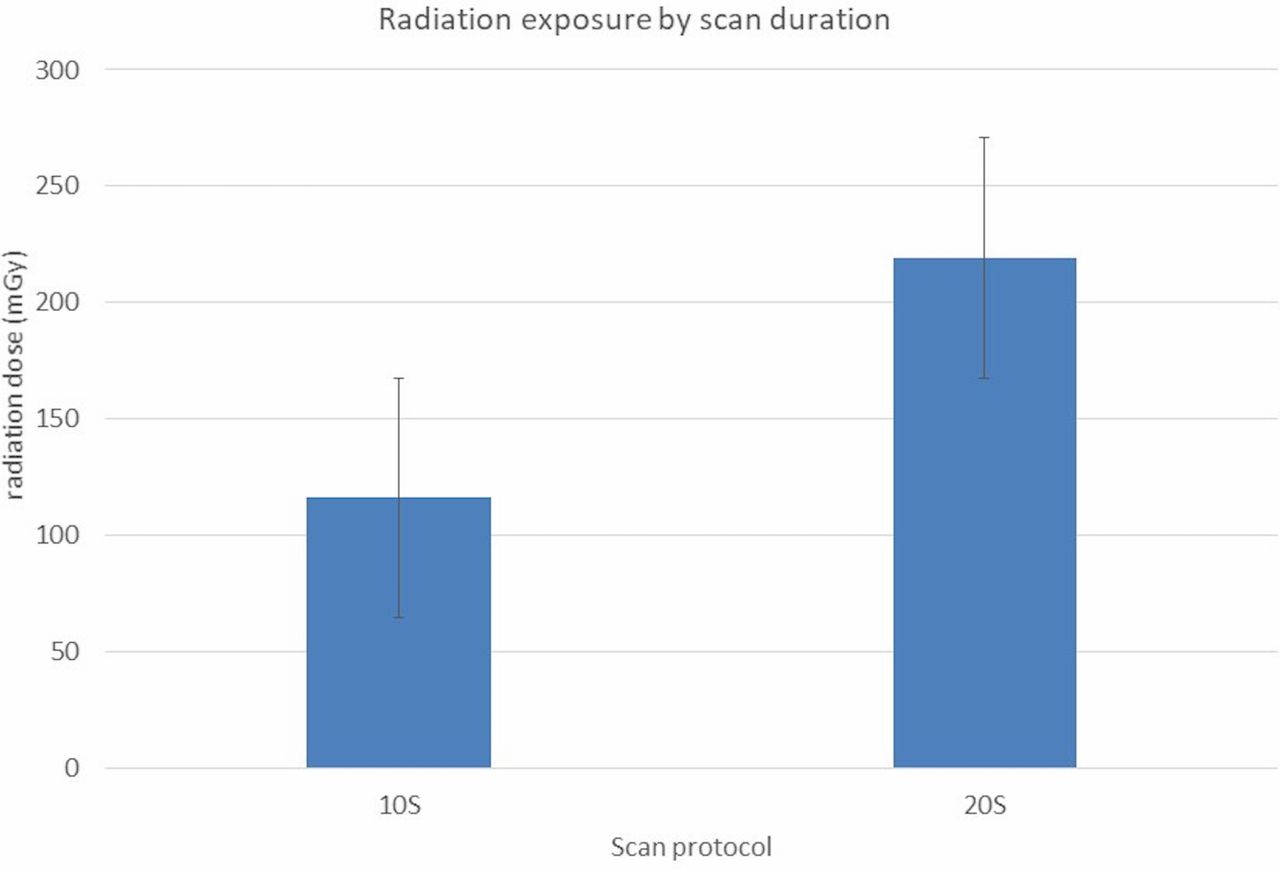
Patient radiation exposure from the 10 s CBCT acquisition was decreased compared with 20 s, as shown in figure 4. Since the 10 s protocol (250 projections) has exactly half the projection images of the conventional 20 s CBCT (~500 projections) protocol, the radiation dose delivered to the patient is also half that of the conventional 20 s CBCT. The contrast load is also reduced from 66 mL to 36 mL.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Radiation exposure by scan duration. A linear correlation is seen with scan duration, with 10 s scans having exactly half the dose of a comparative 20 s scan.
Discussion
CBCT is now a commonly used technique in neurointervention, whether as a diagnostic modality or in the post-interventional phase of treatment evaluation. On the one hand, still-developing tools such as optical coherence tomography offer more invasive methods for evaluating the vasculature and endovascular devices with high fidelity.10 High-resolution CBCT protocols also aim for the same bar, to reach even higher resolution. However, the utility of CBCT imaging is limited due to longer acquisition time, added radiation exposure, and contrast load.10 The fast 10 s CBCT protocol we evaluated aims for a different goal—that is, to provide images of comparable quality with less risk and burden on the patient.
In this study we evaluated the quality of images obtained using fast 10 s CE-CBCT protocols. In applying this new protocol in a phantom model, swine model, and in clinical practice, the theoretical benefits were realized in ease of acquisition, application in awake patients, and with an added benefit of reduced radiation exposure and contrast dose. This was evaluated against the theoretical effect of the decreased resolution compared with the conventional 20 s CBCT protocol. Reviewer ratings demonstrated that the flow diverters can be imaged successfully using an alternative fast 10 s protocol and the images were comparable to reference 20 s CBCT images. The 10 s CBCT images provided enough spatial resolution and contrast resolution to assess the flow diverter structure, relationship to the aneurysm neck, and parent artery apposition. Similar findings have also been observed in imaging other devices such as stent retrievers.6 The contrast dose used in the 10 s protocol is nearly half that of the 20 s protocol (36 mL vs 66 mL) as the injection rate is the same between the two and time is reduced by 50%. This provides additional clinical benefit in patients with pre-existing renal issues or in young children.
Use in awake patients
Arguably the most important theoretical strength of the 10 s protocol is its use in awake/lightly sedated patients. Traditional CBCT (~20 s acquisition time) requires the patient to remain still for 22 s. This compares unfavorably with three-dimensional rotational angiograms (3D-RA), with a 5 s protocol, that are routinely used in awake patients. Depending on institutional limitations or interventionalist preference, most diagnostic angiograms and even many minor interventions are done under mild sedation. This prevents the use of conventional 20 s CBCT in most diagnostic contexts and, as such, the most common use in most institutions is when a patient is anesthetized in a post-treatment setting. In contrast, the 10 s CBCT protocol cuts the acquisition time in half resulting in a shorter breath-hold for 12 s. This also results in reduced contrast load of diluted contrast (66 mL vs 36 mL) for the 20 s and 10 s protocols, respectively, thus facilitating the use of CBCT in awake patients during diagnostic angiograms.
Radiation exposure
One of the important considerations associated with all angiographic procedures is the significant radiation exposure. CBCT scans and 3D-RA further increase patient exposure, which can be a consideration both in single session and lifetime exposure for patients with vascular lesions who may need multiple scans and/or procedures. Traditional 20 s CBCT scans have a radiation exposure of 5174.07±2567.6 µGy/m2,8and the 10 s protocol reduces the radiation dose to the patient by approximately 50%. During a long procedure in a pediatric patient, such a reduction could be quite meaningful.
Limitations of study
This study was designed as an early evaluation of a new protocol and as a translation of these new protocols from the bench (phantom and animal models) to the bedside (a few early patients). Further and more widespread use of the protocols will yield more information as to its utility in clinical neurointerventional practice. One of the main limitations of this study is that it mainly focuses on imaging flow diverter studies. Although these results can be extended to other neurovascular devices such as stents and other flow-diverting devices, a systematic study is required to image these other low-profile devices with the 10 s CBCT protocol, especially in the presence of coil mass.
Furthermore, this protocol may not be adapted for soft-tissue imaging such as identifying a hemorrhage or a parenchymal anomaly. Theoretically, the 10 s CBCT protocol has half the projections of a conventional 20 s CBCT protocol and thus both contrast and spatial resolution of the 10 s protocol need to be studied thoroughly in the context of low-contrast imaging studies.
Finally, we have stated the ability to do ‘awake’ scans as a theoretical benefit of the 10 s protocol. However, this theoretical benefit has yet to be fully evaluated and will be the focus of future studies.
Conclusions
CBCT images can be obtained successfully and easily using faster 10 s acquisition protocols. This has been tested with positive results in phantom and animal models and successfully translated to patient use. The 10 s protocol significantly limits the radiation dose, reduces contrast use, and allows its use in awake patients without any significant compromise in image quality. Further studies are necessary to determine its utility and outcome in a larger cohort of patients. These data support further exploration in routine clinical use.
Acknowledgments
We would like to thank our veterinary care team at Baylor College of Medicine, led by Dalis Collins. We are grateful for the expertise of Sebastian Schafer from Siemens Healthcare who assisted with Catphan phantom scans. Finally, we appreciate the assistance with statistical analysis by Divya Lakshminaryanan from the Department of Statistics, Baylor University.
References
Footnotes
Contributors Conception and design: PK, VMS, SRC, GC. Acquisition of data: all authors. Analysis and Interpretation of data: PK, VMS, SRC, GC, KMC. Drafting the article: PK, VMS, SRC, GC. Critically revising the article: all authors. Reviewed submitted version of manuscript: PK, VMS, KMC, GC, JJ, SRC. Study supervision: PK, SRC.
Disclaimer Dr PK serves as a consultant to Stryker and Medtronic.
Competing interests GC is an employee of Siemens Healthcare USA, the manufacturer and developer of the angiographic equipment and software used in this work.
Ethics approval Baylor College of Medicine Institution Review Board (IRB)
Provenance and peer review Not commissioned; externally peer reviewed.