Article Text

Abstract
Background Case series have described the safety and efficacy of LVIS Jr and Atlas stent-assisted aneurysm coiling, but their comparative clinical performance has not yet been formally studied.
Objective To clinically compare LVIS Jr and Atlas stents, emphasizing comparative rates of technical success and complications.
Methods Our institutional endovascular database was queried for aneurysms treated by stent-assisted coiling with either the LVIS Jr or Atlas stents. Demographic data, aneurysm information, treatment technique, periprocedural and device-related complications, and initial and follow-up angiographic results were evaluated.
Results Thirty-seven patients underwent Atlas stent placement and 27 patients underwent LVIS Jr stent placement for aneurysm coiling. There was no significant difference in aneurysm location, size, coiling technique, and coil packing density between the two cohorts. The rate of initial Raymond 1 occlusion was significantly greater in the Atlas cohort (57% vs 41%, P=0.03). The rate of postoperative ischemic complications, both clinically apparent and as defined on postoperative MRI diffusion-weighted imaging, did not significantly differ between the two groups. Follow-up DSA demonstrated a significantly greater rate of Raymond 1 or 2 occlusion for the Atlas cohort (100% vs 81%, P=0.04), and a significantly lower rate of in-stent stenosis (0% vs 19%, P=0.04).
Conclusion This institutional analysis demonstrates greater obliteration rates and lower in-stent stenosis rates for aneurysms treated via Atlas stent-assisted coiling as compared with those treated via LVIS Jr stent-assisted coiling.
- aneurysm
- coil
- stent
- stenosis
- stroke
Statistics from Altmetric.com
Introduction
In the evolution of intracranial stent design to facilitate aneurysm coiling, a new group of stents have emerged that are compatible with smaller delivery, 0.0165 inch microcatheters, including Atlas and LVIS Jr.1–3 All have the obvious advantage of being able to be delivered via the ‘coil catheter,’ and are the subject of multiple recent reports of their safety and efficacy.2 4–7 While these analyses provide useful preliminary data for these stents, important potential limitations may not be highlighted. Furthermore, results from selected centers may not have reliable external validity. This is already reflected in the literature: in one series using the Atlas for stent coiling, the follow-up complete (Raymond 1) occlusion rate was 93%7; in another series, this rate was 44%.6 Similarly for LVIS and LVIS Jr, reported rates of initial Raymond 1 occlusion have varied from 29%8 to 84%.9 As a center with access to both the Atlas and LVIS Jr stents, we sought to clinically compare these two stents, emphasizing comparative rates of technical success and complications.
Methods
Our institutional endovascular database, maintained under local institutional review board approval, was queried for patients undergoing deployment of the LVIS Jr (n=27) or Atlas (n=37) stents for aneurysm coiling between November 2013 and April 2018. Patient demographic information was extracted together with aneurysm information (location, size, prior treatment) followed by detailed treatment information, including technique, angiographic outcome, and periprocedural complications as documented both clinically and by MRI within 24 hours of treatment. Follow-up clinical and angiographic information were also extracted; in-stent stenosis was tallied if at least 10%. Angiographic results were independently adjudicated by at least two authors.
Procedural technique
All patients with unruptured aneurysms are premedicated for at least 5 days with dual antiplatelet therapy with platelet reactivity testing performed using the VerifyNow assay before the procedure. One patient with subarachnoid hemorrhage treated with the LVIS Jr was given IV Integrilin after stent deployment. One patient undergoing placement of the LVIS Jr was a clopidogrel non-responder and was treated with IV Integrilin after stent deployment. All procedures are performed under general endotracheal anesthesia with neurophysiologic monitoring via common femoral artery access with systemic heparinization.
The Atlas stent was deployed via an XT-17 microcatheter in all cases. Six 3 mm diameter stents were deployed through a transcirculation approach—three for basilar apex aneurysms and three for internal carotid artery (ICA) terminus aneurysms. A Y-stent technique was used in two cases—one for a large basilar trunk fenestration aneurysm and another for a large basilar apex aneurysm. The LVIS Jr stent was deployed via a headway 17 microcatheter in the majority of cases (19/26, 73%). In six cases, it was deployed via a Scepter balloon microcatheter (22%), and in two cases, via the SL-10 coiling microcatheter (7%). Two 2.5 mm diameter stents were deployed via a transcirculation approach: one for an ICA terminus aneurysm and another for a basilar apex aneurysm. Two basilar apex aneurysms were treated by Y-stenting.
Statistics
Statistical comparisons between our Atlas and LVIS Jr patient cohorts were performed with the Fisher exact test for categorical variables and an independent t-test for comparison of means (age, aneurysm size, coils deployed, coil packing density, follow-up period) for demographic information, treatment, and angiographic results. P values <0.05 were considered statistically significant.
Results
Background
Thirty-seven patients underwent Atlas stent-assisted aneurysm coiling and 27 patients LVIS Jr stent placement for planned stent-assisted coiling. There was no significant difference in patient age, sex, previous aneurysm treatment, mean aneurysm size, or aneurysm location (table 1). Of five previously treated aneurysms in the Atlas cohort, two had previously ruptured remotely (more than 1 year before); otherwise all were unruptured. Of eight previously treated aneurysms in the LVIS Jr cohort, four had previously ruptured more than 1 year before treatment. One additional aneurysm was treated in a patient with acute subarachnoid hemorrhage.
Comparison of demographic and background aneurysm information
Initial technical and angiographic results
Most aneurysms in both cohorts were treated by microcatheter jailing (table 2). In the Atlas cohort, there was one initial device failure/complication (3%). In treating a large basilar trunk fenestration aneurysm with expected Y-stenting, the first stent did not fully open in the smallest portion of the fenestration. In attempting to cross the stent for expansion with a microcatheter, the proximal stent instead herniated into the aneurysm. Serendipitously, the aneurysm could be treated after stenting the other parent vessel limb and coiling. Five initial device failures/complications occurred in the LVIS Jr cohort (19%); two aneurysms were not coiled as a result. In one case, stent deployment resulted in kickout of a jailed coil microcatheter; the stent could not be further crossed and the case was abandoned as significant stent thrombus was observed. In another patient undergoing planned staged Y-stenting, severe in-stent stenosis of the first stent seen at 2-months' follow-up precluded aneurysm coiling and the aneurysm was ultimately clipped. In one patient, a 3.5 mm x 23 mm stent would not expand; it was retrieved and a new stent was deployed. Asymptomatic, stable in-stent clot formation was observed in the new stent. In another patient, a 2.5 mm x 23 mm stent did not fully open proximally in the A1 after deployment, requiring balloon angioplasty. Three cases of acute in-stent clot formation were seen in the LVIS Jr cohort (11%) and none in the Atlas cohort (0%, P=0.07). There was no significant difference in mean coil packing density or number of coils used. The rate of initial Raymond 1 occlusion was greater for Atlas stent-assisted coiling (57% vs 41%, P=0.03) (table 2).
Comparison of initial and follow-up technical, angiographic, and clinical results
Initial clinical results
Symptomatic, periprocedural ischemic complications were seen in four patients after LVIS Jr stent deployment for coiling (15%) and in one patient after Atlas stent deployment for coiling (3%, P=0.15 for comparison). The one patient sustaining a stroke after Atlas stent coiling had a major middle cerebral artery (MCA) stroke after treatment of a large A1 aneurysm, presumably a result of an embolus from the ICA as a result of either dissection or vasospasm. Thrombectomy was attempted but was complicated by perforation. Three patients had minor strokes after LVIS Jr deployment and one patient had a transient ischemic attack with a negative MRI. Two patients had small thalamic infarcts with resultant mild hemiparesis, and one patient had a septal infarct with resultant transient cognitive deficits.
At the discretion of the treating physician, post-treatment MRI scans were obtained in 23 Atlas patients and 21 LVIS Jr patients. Among the 23 patients with Atlas stents, 35% had DWI lesions on MRI; 13% of patients had a single punctate lesion and 22% had multiple lesions. Among the 21 patients with LVIS Jr stents, 38% had DWI lesions; 19% had single punctate lesions and 19% had multiple lesions. Rates of DWI lesions after treatment did not significantly differ between the two groups (table 2).
Follow-up results
Clinical follow-up was available for all 37 patients undergoing Atlas stent coiling over a mean period of 12.7 months. No patients had clinical evidence of delayed ischemic events, underwent aneurysm re-treatment or sustained aneurysm rupture in follow-up. Formal digital subtraction angiographic follow-up was performed in 25 patients over a mean period of 12.1 months. Clinical follow-up was available for 26/27 patients undergoing LVIS Jr stent placement for planned aneurysm coiling over a mean period of 17.0 months. No patients had clinical evidence of delayed ischemic events or aneurysm rupture. One patient underwent aneurysm re-treatment. Formal digital subtraction angiographic follow-up was performed in 21 patients over a mean period of 11.6 months.
Comparing the two cohorts, there was a significantly greater rate of aneurysm dome filling (Raymond 3 occlusion) among patients treated with the LVIS Jr stent at the last angiographic follow-up (19% vs 0%, P=0.04). Carrying forward initial angiographic results in patients without angiographic follow-up (including all patients), rates of Raymond 3 occlusion still differed between the two cohorts (19% vs 3%), but the difference did not meet statistical significance (P=0.07). There was also a statistically significantly greater rate of in-stent stenosis among patients undergoing stenting with LVIS Jr (19% vs 0%, P=0.04).
Discussion
The emergence of 0.0165 inch microcatheter-compatible dedicated intracranial stents marks an important advance in the evolution of endovascular therapy for aneurysms.1–3 This compatibility facilitates more complex approaches and access to daughter branches with more supple microcatheters that can also be used to coil the aneurysm. With access to both the Atlas and LVIS Jr stents, instead of reporting gross rates of aneurysm obliteration and complications, we sought instead to compare our institutional results with these two stents to allow for more meaningful extrapolative results.
The laser cut nitinol, open-cell design of the Atlas eliminates foreshortening and allows for better predictability of the proximal landing point of the stent as denoted by the proximal marker. This can be particularly relevant in transcirculation cases. Furthermore, extrapolating from an intriguing previous comparison of the Neuroform and Enterprise stents, it may also allow for comparatively better wall apposition around turns.10 Available 4 mm and 4.5 mm diameters for the Atlas stent are advantageous in its use for ICA branch and vertebral aneurysms. As noted in this series, only one ICA branch aneurysm was treated with the LVIS Jr as compared with 10 treated with the Atlas. Given the observed lack of delayed in-stent stenosis after Atlas stent deployment, its smallest 3 mm diameter does not appear to be a limitation as compared with the smaller 2.5 mm diameter LVIS Jr stent.
The woven, closed-cell design of the LVIS Jr allows for retrievability, which can be advantageous. We had one case in which a poorly expanded stent was retrieved and another where the stent was partially deployed to allow for reduction of a looped microcatheter in a large aneurysm. In addition, the reliable compatibility of the LVIS Jr with the Scepter balloon is a noteworthy advantage that allows for seamless transition from balloon-assisted coiling to stent-assisted coiling, as noted in six cases in this series. It is also a more visible stent than the Atlas, which is marked only by proximal and distal radiopaque markers.
These stents were used in similar patient cohorts as defined by patient age, sex, general aneurysm location, and aneurysm size. As LVIS Jr is available in only 2.5 or 3.5 mm diameters, it was used only in one ICA branch aneurysm. Otherwise, basilar apex and anterior communicating artery aneurysms were the most commonly treated aneurysms in both cohorts. Coil technique was generally similar in both cohorts (jailing), although in three cases an LVIS Jr was deployed after coiling owing to coil prolapse. No thromboembolic complications occurred in these three cases. Incomplete stent expansion was seen in both cohorts (7% for LVIS Jr, 3% for Atlas), but stent thrombus formation showed a trend towards being more common after deployment of LVIS Jr (11% of cases vs 0%, P=0.07). One of the three patients with in-stent clot formation was a clopidogrel non-responder (P2Y12 reaction unit (PRU) of 289) who was treated with IV Integrillin after stent deployment. The other two patients were clopidogrel responders (serum PRUs of 170 and 136). All cases of in-stent clot formation were clinically asymptomatic. Shankar et al reported a 14% rate of in-stent clot formation in their detailed review of 100 patients treated with LVIS Jr in a multicenter registry.5 They emphasize, as do we, that these phenomena are often not reported when clinical manifestations are absent. Behme et al reported a similar rate of in-stent clot formation for the LVIS Jr with 2/34 patients in their analysis, both clopidogrel responders, demonstrating intraprocedural in-stent clot formation (6%).11 Wang et al reported 7/69 patients undergoing LVIS or LVIS Jr stenting having stent-related thrombotic complications (10%), which was higher than their observed rate after stent coiling with either the Neuroform or Enterprise stent.12 Our very low rate of in-stent thrombus formation for the Atlas was mirrored by the study of ten Brinck et al, who reported one case of in-stent thrombus formation among all patients with unruptured aneurysms.6 Notably, however, across a cohort of 10 patients with treated ruptured aneurysms, three patients had intraprocedural thromboembolic complications.
While coil packing density was similar between the two cohorts, we observed higher rates of initial Raymond 1 occlusion after Atlas stent-assisted coiling (57% vs 41%, P=0.03). Our rates of initial Raymond 1 occlusion are comparable to reported results for both Atlas stent-assisted coiling11 and LVIS Jr stent-assisted coiling.1 8 The difference in rates of Raymond 1 occlusion persists but is no longer statistically significant if one excludes patients with previously treated aneurysms or the two patients who could not undergo coiling of their aneurysms owing to severe in-stent stenosis or in-stent thrombus formation after microcatheter kick-out. Wang et al reported significantly greater rates of initial Raymond 1 occlusion after stent-assisted coiling with Neuroform (65%, n=109) as compared with LVIS or LVIS Jr (48%, n=73).12 Rates of periprocedural complications and MRI-adjudicated ischemia were the same between the two cohorts in our study.
Follow-up angiographic results showed lower rates of dome remnants (Raymond 3 occlusion) in the Atlas cohort (0% vs 19%, P=0.04). Carrying forward patients without angiographic follow-up, a difference was still seen but was no longer statistically significant (3% vs 19%, P=0.07). Interestingly, 11/11 patients with Raymond 2 or 3 occlusion after Atlas coiling demonstrated improvement in aneurysm occlusion at follow-up, with nine improving to Raymond 1 occlusion. Eight of ten patients with Raymond 2 or 3 occlusion after LVIS Jr coiling also demonstrated improvement in aneurysm occlusion at follow-up. Such significant improvement has been reported previously for the LVIS Jr,12 13 with some attributing it to a potential ‘flow diverting’ property of the stent. Given similar rates seen for the Atlas stent, it would be difficult to consider that this occurred as a result of a ‘flow diverting’ property of the stent, itself. Importantly, no patients sustained aneurysm rupture in either cohort over the follow-up period.
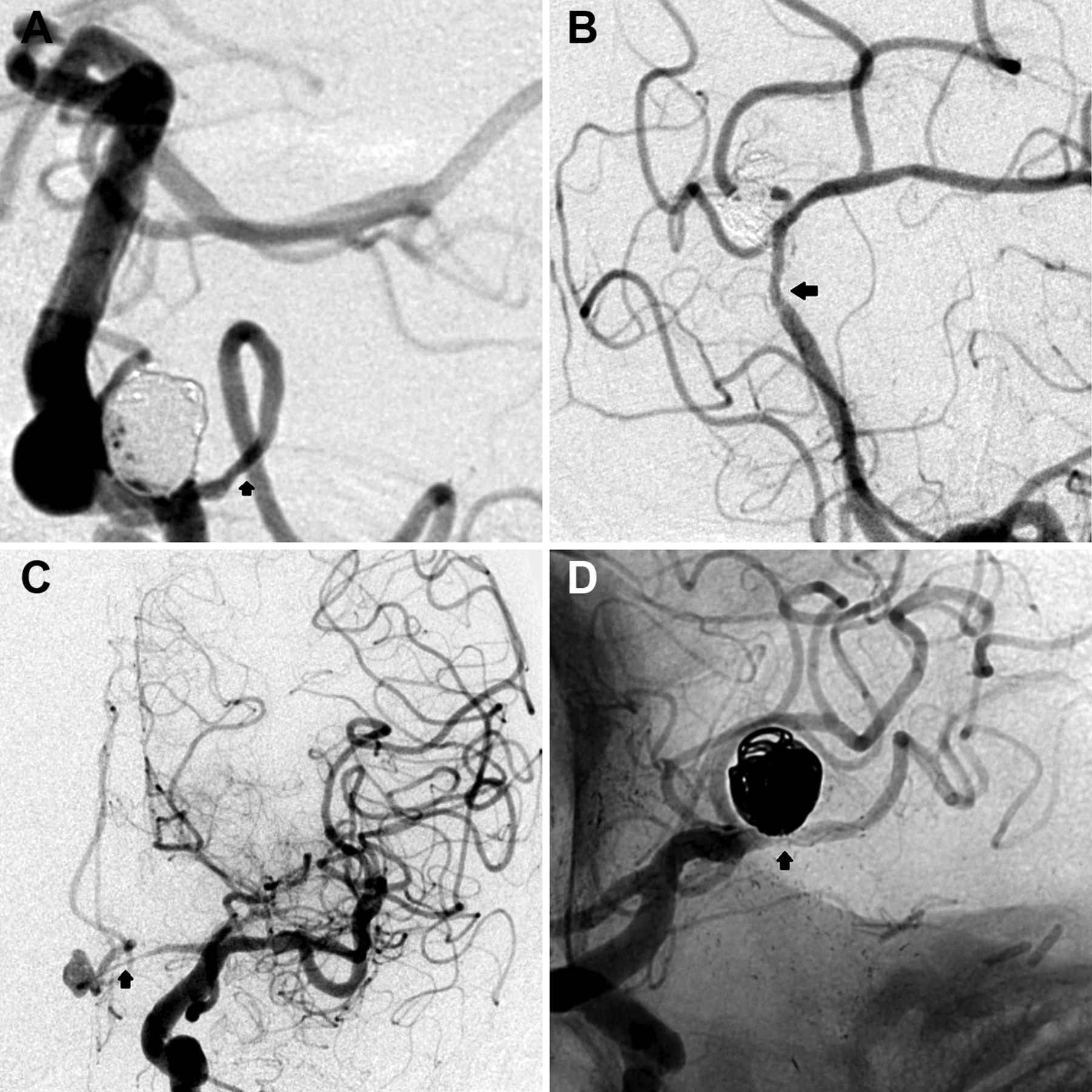
Perhaps the most intriguing result in this study was the significant difference in rates of in-stent stenosis at follow-up. Some studies have not described in-stent stenosis after LVIS Jr deployment,8 9 but Cho and colleagues reported an in-stent stenosis rate of 87% for 30 aneurysms with formal angiographic follow-up.3 Another study by Feng and colleagues reported a 10% rate of angiographic moderate or severe in-stent stenosis after LVIS deployment.14 Our four cases of in-stent stenosis are illustrated in figure 1. None of these cases demonstrated in-stent clot formation during the procedure and all patients were clopidogrel responders (PRU range 47–150). This excludes an additional case of asymptomatic complete stent thrombosis that occurred after deployment of a stent in the posterior inferior cerebellar artery, which developed an in-stent clot during the procedure.

{kind=link}
Cases of mild (A,B) and severe (C,D) in-stent stenosis on angiographic follow-up.
Limitations of this study include our sample size and single institutional experience/results. This analysis does not represent a randomized comparison of the two stents and technical experience of all operators was greater with the Atlas stent as it was introduced after the LVIS Jr stent. Follow-up is limited (mean of 1–1.5 years), and not all patients underwent postprocedural MRI. Nevertheless, it is difficult to expect that these limitations will influence the clinically significant finding of a greater rate of in-stent stenosis at angiographic follow-up for the LVIS Jr device.
Conclusion
This institutional analysis demonstrates that for similar cohorts of patients with cerebral aneurysms treated with the Atlas or LVIS Jr for stent-assisted coiling, rates of initial complete angiographic obliteration (Raymond 1), and follow-up obliteration (Raymond 1 or 2) class were significantly greater for aneurysms treated with the Atlas stent. In addition, the rate of in-stent stenosis was significantly lower in angiographic follow-up for the Atlas stent.
References
Footnotes
Contributors BAG: drafting of the article. BAG, WJA: acquisition of data/data analysis. All authors: review and revision of article before submission. BTJ: study supervision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests TGJ received a grant, non-financial, from Fundació Ictus Malaltia Vascular and modest honoraria from Silk Road (consultant), Medtronic and Stryker Neurovascular (consultant/advisory board), and Neuravi (consultant). BTJ is a consultant for Medtronic and Stryker Neurovascular (Co-PI, ATLAS study). AFD is a consultant for Medtronic and Penumbra.
Patient consent Not required.
Ethics approval Pittsburgh local institutional review board (UPMC).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement N/A.