Article Text

Abstract
Background Embolectomy using Stent retriever Assisted Vacuum-locked Extraction (SAVE) is effective in intracranial large vessel occlusion. Which post-bifurcational trunk should be chosen for distal stent retriever placement in M1 occlusions is, however, elusive.
Methods We conducted a retrospective analysis of prospectively collected data from a comprehensive stroke center between 2015 and 2017. Eighty-nine consecutive patients with M1 occlusions were treated with SAVE. Digital subtraction angiography (DSA) series were studied to determine the anatomy of middle cerebral artery division, the position of the stent retriever, and to measure vessel diameters. The primary endpoint was first-pass complete/near-complete reperfusion, defined as a modified Thrombolysis in Cerebral Infarction (mTICI) score of 2c or 3, after distal stent retriever placement in the inferior trunk.
Results In 76/89 (85%) patients, microcatheter series were documented. A microcatheter was placed within the inferior trunk in 30/76 (40%) cases. First-pass near-complete/complete reperfusion was more likely to be achieved when the inferior trunk was used for stent retriever placement rather than the superior trunk (mTICI ≥2c: 22/30 (73%) vs 22/46 (48%), P=0.034; and mTICI 3: 20/30 (67%) vs 17/46 (37%), P=0.018). Median diameter of the inferior trunk was larger than the superior trunk (1.4 mm (IQR 1.26–1.62) vs 1.18 mm (IQR 0.98–1.43), P=0.011). The inferior trunk was dominant in 56/76 (74%) cases. Successful reperfusion was associated with placement within the dominant trunk (33/40 (83%) vs 22/36 (61%), P=0.044).
Conclusion The choice of the inferior trunk for distal stent retriever placement in M1 occlusions is associated with a high rate of first-pass near-complete/complete reperfusion when using SAVE.
- stroke
- thrombectomy
- technique
Statistics from Altmetric.com
Introduction
Endovascular therapy with modern stent retrievers has been shown to be the most effective treatment option for patients with acute ischemic stroke (AIS) due to large vessel occlusion (LVO) in the anterior circulation as the clinical outcome is improved when early and successful revascularization of the occlusive lesion is achieved.1 A common neurointerventional embolectomy technique comprises a primary combined approach, which includes the use of a distal access catheter and a stent retriever.2 The Stent retriever Assisted Vacuum-locked Extraction (SAVE) technique is a variation of the primary combined approach and effective with regard to high reperfusion rates, which may be explained by the distal positioning of the stent retriever in relation to the thrombus center and the wedged thrombus position between the catheter and stent retriever.3 However, in many cases complete reperfusion cannot be achieved after one attempt. Possible factors influencing the reperfusion result may be histologic thrombus structure and thrombus length.4 5 In a recent study the thrombus location within the M1 segment of the middle cerebral artery (MCA) was not a predictor of reperfusion success.6 Another study focused on vessel anatomy and showed that strongly curved MCAs with large vessel angles determine the reperfusion result negatively.7
In this study we analyzed the anatomy of the MCA bifurcation in anteroposterior and lateral views of digital subtraction angiography (DSA) and the influence of the post-bifurcational trunk used for distal stent retriever placement in M1 occlusions on first-pass reperfusion success when using SAVE. Based on our own experiences, we hypothesized that the inferior trunk is more effective than the superior trunk due to a larger vessel diameter, as demonstrated in micro-anatomical studies.8 The purpose of this study was also to serve as a viable basis to provide information in which trunk the stent retriever should be navigated into to potentially improve the first-pass reperfusion result.
Materials and methods
Study design and patient selection
A retrospective analysis of data was performed to identify all patients who consecutively underwent embolectomy with the SAVE technique between May 2015 and November 2017. Baseline and angiographic parameters were extracted from a prospectively acquired database.
Inclusion criteria were embolectomy using the SAVE technique in patients aged ≥18 years with M1 occlusions and proper angiographic documentation of the procedure including a post-bifurcational contrast injection via microcatheter behind the occlusion and/or via the aspiration catheter after stent retriever deployment. Cases missing both series in our picture archiving system (Centricity Universal Viewer, GE Healthcare, Chicago, Illinois, USA) were excluded. Only the first maneuver of each embolectomy was used for further analysis. Patients with MCA trifurcation or an occlusion of the internal carotid artery, isolated occlusion of M2 or anterior cerebral artery were also excluded. All eligible patients received intravenous thrombolysis based on the judgement of the attending neurologist according to the guidelines of the National Neurological Society.
The primary endpoint was first-pass complete/near-complete reperfusion, defined as a modified Thrombolysis in Cerebral Infarction (mTICI) score of 2c or 3. Secondary endpoints were first-pass rate of successful reperfusion (mTICI ≥2b), occurrence of post-interventional symptomatic intracranial hemorrhage (sICH), and embolization to new territories (ENT). According to the guidelines of the local ethics committees, ethics approval was given for the prospective acquisition of patient data, which was conducted in accordance with the Declaration of Helsinki.
Endovascular treatment
SAVE has been described previously.3 Briefly, based on a triaxial approach, a microcatheter is advanced past the occlusion site into a post-bifurcational MCA trunk randomly. After contrast injection via the microcatheter to confirm intraluminal position, a stent retriever (Trevo variants, Stryker Neurovascular, Fremont, California, USA) is placed with the proximal third across the occlusion site and with the main portion within the post-bifurcational MCA trunk. The stent retriever is deployed over 2–8 min. After retraction of the microcatheter, the aspiration catheter is advanced to the proximal face of the clot to reach a wedge position. The stent retriever and aspiration catheter are then withdrawn into the guide catheter as a unit under continuous aspiration via the aspiration catheter and guide catheter (https://vimeo.com/245744122).
Angiographic analysis
Pre-interventional and post-thrombectomy DSA series were re-evaluated in accordance with the recommendations of the Cerebral Angiographic Revascularization Grading Collaborators from an internal core team that was not involved in the evaluated procedures, consisting of a senior neuroradiologist (MP or IT) and a medical student (SH). The core team was blinded to the clinical outcome, presentation, or any demographic data to assess the initial state and extent of tissue reperfusion after the first embolectomy attempt.9 Evaluation of the microcatheter series and measurements of vessel anatomy and diameter were performed by a senior neuroradiologist (VM) and an assistant physician (AB). The respective MCA trunk of each patient in which the microcatheter was navigated prior to the first embolectomy attempt was evaluated. Vessel diameter of each trunk was determined on microcatheter series in available anteroposterior and lateral views on DSA. Therefore, the tip of the microcatheter was used as a reference to estimate the luminal diameter. In cases of measurement discrepancies, the largest diameter was chosen for further analysis. The allocation of the navigated trunk (inferior vs superior) was decided on a final angiogram in cases of successful reperfusion or on an angiogram after temporary successful reperfusion. Dominance of the trunk was visually assessed on the final angiogram.
In addition, the intracranial vasculature was evaluated either on a multidetector CT angiography (MDCTA) or a biphasic flat-detector CT (FDCTA) by a senior neuroradiologist (IT). FDCTA was performed with a biplane flat detector angiography system (Artis Q; Siemens, Erlangen, Germany), as described previously.10 FDCTA datasets were automatically reconstructed and 24 mm transversal maximal intensity projections including fusion of the first and second phase were analyzed to detect the dominant post-bifurcational trunk ipsilateral and contralateral to the site of the LVO. In cases where no conclusion could be drawn for ipsilateral anatomy, the contralateral side was used for further analysis.
Statistical analysis
Statistical analysis was performed using MedCalc Statistical Software Version 18 (MedCalc Software, Ostend, Belgium; http://www.medcalc.org; 2018). Descriptive statistics are shown as mean and SD if normally distributed and as median and IQR if not. The Mann–Whitney U test and the Fisher test were performed for assessing statistical differences between groups. To assess the predictive value of CTA for evaluation of the dominance of the post-bifurcational trunk we used receiver operating characteristic (ROC) analysis. Statistical significance was defined as P≤0.05.
Results
Eighty-nine consecutive patients with M1 occlusions were treated with SAVE. Their mean age was 77 years and 56% were female (table 1). Thirteen patients were excluded due to missing microcatheter series (n=8), inability of allocation (n=3), and presence of trifurcation (n=2). For the remaining 76 patients (85%), a microcatheter series prior to the first embolectomy attempt was documented on DSA. First-pass near-complete (mTICI 2c) or complete (mTICI 3) reperfusion was achieved in 44/76 (58%) and 37/76 (49%) patients, respectively. First-pass reperfusion was successful (mTICI ≥2b) in 55/76 patients (72%). Median groin puncture to reperfusion time was 39 min (IQR 28–57). The microcatheter was placed in the inferior trunk in 30/76 (40%) and in the superior trunk in 46/76 (60%) cases. First-pass near-complete/complete reperfusion was more likely achieved if the inferior trunk was used for stent retriever placement (mTICI ≥2c: 22/30 (73%) vs 22/46 (48%), P=0.034; mTICI 3: 20/30 (67%) vs 17/46 (37%), P=0.018, table 2). First-pass reperfusion was successful (mTICI ≥2b) in 25/30 (83%) vs 30/46 (65%) patients (P=0.117). The median diameter of the inferior trunk was larger than the superior trunk (1.4 mm (IQR 1.26–1.62) vs 1.18 mm (IQR 0.98–1.43); P=0.011), with a dominance of the inferior trunk in 56/76 (74%) cases based on DSA.
Baseline and clinical characteristics
Reperfusion results dependent on post-bifurcational stent retriever placement
Stent retriever placement in the dominant trunk occurred in 40/76 (53%) cases. The rate of first-pass near-complete/complete reperfusion was higher when the stent retriever was placed within the dominant trunk as opposed to the non-dominant trunk (mTICI ≥2c: 27/40 (68%) vs 17/36 (47%), P=0.104; and mTICI 3: 23/40 (58%) vs 14/36 (39%), P=0.115); first-pass reperfusion was successful in 33/40 (83%) vs 22/36 (61%, P=0.044) cases. First-pass complete reperfusion was associated with larger luminal diameter of the trunk used for stent retriever placement on DSA: median vessel diameter in patients with first-pass mTICI 3 was 1.37 mm (IQR 1.21–1.61) compared with 1.16 mm (IQR 0.95–1.59) for mTICI <3 (P=0.029, table 3).
Reperfusion result dependent on vessel diameter
Evaluation of the CTA revealed a dominance of the inferior trunk in 68/76 (89%) cases. In 35/76 (46%) cases, the ipsilateral MCA anatomy could be clearly assigned. ROC analysis for assessment of the dominant trunk on CTA compared with DSA revealed a sensitivity of 92.6% (95% CI 82.1% to 97.9%) and a positive predictive value (PPV) of 78.1% (95% CI 73.4% to 82.2%). Of the 35 patients with visible bilateral MCA anatomy on CTA, 34 (97%) showed a symmetric distribution of dominant and non-dominant trunks, meaning that allocation of the dominant trunk on both sides was identical (inferior or superior).
The rate of sICH was 3%; however, it did not occur in cases of near-complete/complete reperfusion after one embolectomy attempt. ENTs were present in four patients (5%), two of whom required more than one maneuver.
Discussion
Endovascular treatment using stent retrievers is currently state of the art therapy in patients with AIS due to intracranial LVO in the anterior circulation.11 The central requirement of embolectomy is fast recanalization and complete reperfusion of the affected territory, as both factors primarily predict patient clinical outcome.12 13 We recently introduced the SAVE technique as a combined approach, which includes the use of a distal access catheter and a stent retriever to achieve a high rate of successful reperfusion.3 One explanation for the effectiveness of this method might be the distal positioning of the stent retriever in relation to the thrombus center and the wedged thrombus position between catheter and stent retriever. However, in some patients a near-complete or complete reperfusion cannot be achieved with a single embolectomy maneuver. Taking into consideration that achievement of complete reperfusion after a single embolectomy maneuver is associated with a significantly higher rate of favorable clinical outcome,14 we analyzed the influence of the post-bifurcational trunk used for distal stent retriever placement in M1 occlusions treated with SAVE. In our study we found that (a) first-pass near-complete/complete reperfusion is more likely to be achieved if the stent retriever is placed within the inferior trunk and (b) the probability of first-pass successful reperfusion is increased if the dominant trunk is chosen for stent retriever placement.
In our cohort nearly three-quarters of the cases showed dominance of the inferior trunk based on DSA. This observation is underlined by previous microsurgical studies which demonstrated a higher frequency of dominant inferior trunks compared with superior trunks.15 16 However, our rate is higher than the aforementioned studies, which found inferior trunks to be dominant in up to 54%.15 This can be explained by the fact that our study design only allowed the classification of trunks as dominant and non-dominant, even in cases where differentiation of vessel caliber was difficult. Thus, our allocation did not include co-dominant trunks. The diameters of both trunks were lower compared with previous studies. While in our study the median diameter of the inferior trunk was 1.4 mm and the median diameter of the superior trunk was 1.18 mm, Kahilogullari et al found mean diameters of 2.55 mm for the inferior trunk and 2.9 mm for the superior trunk15 and Tanriover et al described mean diameters of 2.26 mm for the inferior trunk and 2.19 mm for the superior trunk.8 The lower vessel diameters in our study can be explained by a number of factors. First, the location of measurement differed from other studies. While other studies measured the diameter at the origin of the trunks, we measured it more distally due to the distal placement of the microcatheter. Another contributing factor might be the reduced contrast of the vessel lumen after injection via microcatheter on angiogram-, which was the basis for our measurements. Another aspect might be a reduced tonus of the vessel wall in a post-thrombosed segment.
Positioning of the stent retriever in the dominant trunk led to a high rate of first-pass successful reperfusion. One explanation could be that the increased radial force of the stent retriever has a positive impact on the interaction between the stent struts and the clot if the vessel diameter has a particular size, which may result in better stent deployment in larger vessels. This may provide a better capture profile of the stent retriever with favorable entrapment of the clot. This agrees with a recent study by Kurre et al who inversely demonstrated that, in small (1.5–2 mm) intracranial vessels, stent retrievers with a reduced radial force showed promising reperfusion results.17
Although our study focuses on a certain embolectomy technique called SAVE, the positioning of the stent retriever in the dominant trunk might be reasonable in other combined approaches as well. Despite the fact that other established techniques such as continuous aspiration prior to intracranial vascular embolectomy (CAPTIVE) or aspiration-retriever technique for stroke (ARTS) differ with regard to proximal aspiration, the time point of starting aspiration via the intermediate catheter or the positioning of the stent retriever in relation to the thrombus center, one can assume that better stent deployment in the post-bifurcational trunk due to a larger vessel diameter might improve the effectiveness with these techniques as well.18 19
The anatomy of the MCA should be analyzed on CTA whenever possible prior to intervention to determine the dominance of the post-bifurcational trunk into which the microcatheter and subsequently the stent retriever should be navigated to increase the probability of successful first-pass reperfusion. In cases where the MCA anatomy ipsilateral to the LVO could not be evaluated on CTA, the contralateral side should be assessed as, in our study, 97% of the patients showed symmetrical distribution of dominant and non-dominant trunks on CTA. Assessment of the dominant trunk on CTA compared with DSA revealed a PPV of 78%, which demonstrates the feasibility of CTA for determining vessel dominance.
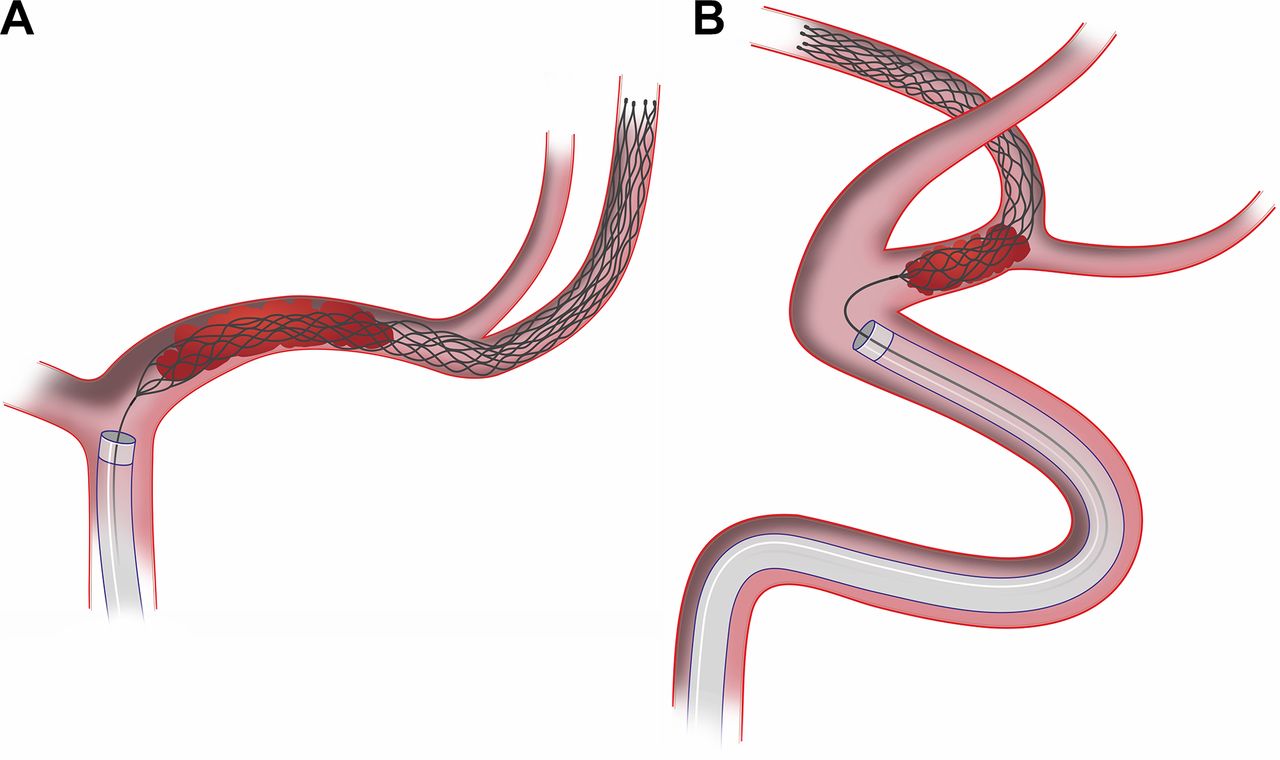
We recommend that, after analyzing the pretreatment CTA, the dominant trunk should be assessed and microcatheterization of this trunk should be conducted. The stent retriever should be navigated into the inferior trunk if it is found to be dominant on CTA as described above (Figure 1) or in cases where no conclusion could be drawn regarding dominance of a trunk on CTA. During the procedure it is difficult to visualize the post-bifurcational segments due to poor or no contrast opacification. Thus, the operator should pay special attention to the lateral DSA view as an oblique trajectory of the microcatheter is typical when it is navigated towards the inferior trunk. A subsequent angiogram via the microcatheter can be done to confirm catheterization of the inferior trunk and positioning of the microcatheter tip distal to the clot.
This study has several limitations. First, it is a small and retrospective study with the attendant selection bias. Confirmation of our results in a larger cohort is necessary and will be conducted. Second, a fraction of patients with non-successful reperfusion had to be excluded due to a missing final angiogram and subsequent inability of allocation, which might be a further bias. Third, differentiation between dominant and non-dominant vessels was assessed visually without recording true diameters due to a missing reference in the final angiogram. Fourth, individual variations in patient anatomy (eg, trifurcation) were not considered. Furthermore, the angulation of the MCA was not taken into consideration, which might have an influence on the reperfusion success as well.
Conclusion
Our findings suggest that the post-bifurcational positioning of the stent retriever in patients undergoing embolectomy with the SAVE technique due to an acute M1 occlusion influences the first-pass reperfusion result. Our data indicate that stent retriever placement in the inferior trunk, which is usually dominant, may increase the rate of complete/near-complete reperfusion with fewer stent retriever passes. This approach may also have an impact on the clinical outcome of these patients, which needs to be investigated in further studies. Useful information about the vessel anatomy can be received on CTA prior to the intervention.
{kind=link}
Schematic illustration of recommended stent retriever positioning in a left M1 occlusion with a dominant inferior trunk. (A) Anteroposterior view. (B) Lateral view.
References
Footnotes
Contributors Conception and design: VM, M-NP. Acquisition of data: AB, IT, SH. Analysis and interpretation of data: VM, AB, M-NP. Drafting the article: VM, M-NP. Critically revising the article: all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests VM and IT: minor travel grants: Stryker Neurovascular, Kalamazoo, USA. M-NP: minor travel grants and modest speaker’s honoraria: Stryker Neurovascular, Kalamazoo, USA; Phenox, Bochum, Germany; Penumbra, Alameda, USA; Acandis, Pforzheim, Germany; Siemens, Forchheim, Germany.
Ethics approval The study received waived approvals by the local ethics committees of the participating centers. The study was conducted in accordance with the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.