Article Text

Abstract
Background and purpose Vascular wall components (VWCs) are sometimes identified as collagen fibers in specimens retrieved by thrombectomy from acute stroke patients. However, their clinical significance and associated factors remain unclear. The purpose of this study was to clarify the factors associated with VWCs in retrieved thrombi.
Methods Consecutive acute stroke patients treated endovascularly using the Penumbra aspiration catheter or stent retrievers (SRs) at our institute from November 2013 to April 2016 were retrospectively reviewed, and the retrieved thrombi were evaluated histopathologically. VWCs were defined as banded collagen fibers with a distinct boundary observed at the rim or outside of the retrieved thrombi. Factors associated with the presence of VWCs were studied.
Results A total of 150 specimens (76 specimens retrieved by the Penumbra, 74 by SRs) from 101 patients (47 women, age 74.9±11.1 years) were investigated. Applied thrombectomy devices were aspiration catheters in 42 patients, SRs in 21 patients, and both in 38 patients. VWCs were observed in 24 specimens (16%) from 22 patients. A low proportion of erythrocyte components (41.7±24.8% vs 55.0±26.3%, P=0.01), a high frequency of the devices reaching the M2/P2 (75% vs 50%, P=0.02), and a high number of device passages (P for trend=0.02) were associated with VWC positive thrombi. Successful recanalization (Treatment in Cerebral Ischemia ≥2b) tended to be less frequent in patients with VWC positive thrombi than in those without (73% vs 89%, P=0.06).
Conclusions The histopathology of occlusive thrombi, arterial sites where devices reached, and number of device passages, might affect the presence of VWCs in retrieved thrombi.
- mechanical thrombectomy
- vascular damage
- thrombus
Statistics from Altmetric.com
Introduction
The effectiveness and safety of stent retriever thrombectomy devices (SRs) and a direct aspiration first pass technique (ADAPT) using a large bore aspiration catheter, such as the Penumbra Reperfusion Catheter (Penumbra Inc, Alameda, California, USA) have been fully established for acute stroke patients with large vessel occlusion.1–9 However, device related vessel damage, such as vasospasm, perforation, and dissection, sometimes occurs.1–9 In addition to the injury of the vessel wall resulting in apparent vessel rupture or dissection, it was thought that angiographically occult vessel ruptures caused by mechanical stretch on retrieval could be associated with vessel wall permeability impairment and blood–CSF barrier disruption after SR thrombectomy.10 11 It has been reported that the Solitaire FR (Medtronic, Irvine, California, USA) and the Penumbra aspiration system caused vascular injury extending into the medial layer in swine models, suggesting that histological vascular injury caused by the second generation thrombectomy devices could occur at a certain frequency in real clinical settings.12 Vascular injury has also been reported to differ by degree among type, diameter, and length of the thrombectomy device in animal models and in an in vitro live cell platform.12–14 However, the histological changes occurring in the arterial wall following mechanical thrombectomy (MT) in human cerebral arteries are difficult to evaluate.
Collagen fibers in specimens retrieved by thrombectomy were assumed to be parts of the blood vessels in contact with the thrombi or thrombectomy devices.15 We considered that the presence of collagen fibers derived from vascular wall retrieved with thrombi would be a surrogate marker of histological vascular injury. The purpose of the present study was to investigate the frequency, clinical significance, and factors related to the presence of the retrieved vascular wall components (VWCs).
Methods
Patients
Consecutive acute stroke patients treated endovascularly with ADAPT or SR (including a combined stent aspiration technique, such as ‘Solumbra’ and others) extracted from a prospectively maintained database at our institute (the National Cerebral and Cardiovascular Center Stroke Registry (Clinical Trials.gov: NCT02251665)) from November 2013 to April 2016 were retrospectively reviewed, and the retrieved thrombi were evaluated histopathologically. As previously described,16 expert stroke neurologists in our institute determined the patients’ stroke subtypes, according to the ASCOD phenotyping scheme. Patients with extracranial carotid occlusion alone were excluded from the analysis. All patients, or their legally authorized representative, provided written informed consent for endovascular therapy. Consent to participate in this clinicopathological study was obtained using an opt out approach. The research ethics committee of our institute approved the study.
Clinical information
The following clinical information was collected for each patient: age, sex, cerebrovascular risk factors, baseline National Institutes of Health Stroke Scale (NIHSS) score, intravenous (IV) recombinant tissue plasminogen activator (rt-PA) administration, occluded vessels, stroke subtypes, endovascular procedures, onset to reperfusion time (in cases where onset times were not evident, the time last known well was treated as the onset time), degrees of reperfusion after MT, and the presence of any intracranial hemorrhage (ICH) and subarachnoid hemorrhage (SAH). ICH was defined as an intracranial hyperdense lesion on 24–36 hour follow-up non-contrast CT scan or a hypointense lesion on gradient echo MRI. SAH was defined as a subarachnoidal hyperdense lesion on a non-contrast CT scan immediately after the procedure. Clinical outcome was measured using the modified Rankin Scale (mRS) score at 3 months, and good clinical outcome was defined as a score of 0–2.
Endovascular treatment
As previously described,16 endovascular reperfusion therapy in patients with acute major cerebral arterial occlusion was performed according to domestic guidelines. The firstline thrombectomy procedure was ADAPT2 using the Penumbra aspiration catheters, including 4MAX, 5MAX (from November 2013 to February 2014), and 5MAX ACE (from November 2014 to April 2016) or SRs (from March 2014 to October 2014). If the firstline procedure was unsuccessful, additional devices were used at the first operator’s discretion. During the study period, one of three interventional neurologists performed thrombectomy as the first operator, of whom experience of SR thrombectomy and ADAPT were from 12 to 27, 21 to 31 procedures at the end of the study period, respectively. The number of device passages was counted consistently during the procedure, regardless of the type of device. If the patient was eligible, IV rt-PA was given using 0.6 mg/kg of alteplase prior to MT within a 4.5 hour window, according to the standard protocol approved in Japan.17 The degree of reperfusion was blindly evaluated on postprocedural angiograms using the modified Treatment in Cerebral Ischemia (mTICI) scale.18 Successful reperfusion was defined as mTICI grade 2b–3.
Histopathological analysis
The specimens retrieved by MT were analyzed histopathologically. Whenever thrombus was retrieved, it was submitted as a separate specimen. Obtained specimens were fixed in 10% phosphate buffered formalin solution for 1 day. Formalin fixed specimens were embedded in paraffin, cut at a thickness of 5 µm, and stained with hematoxylin–eosin and Masson’s trichrome. Histopathological evaluation was performed without knowledge of the clinical findings. Specimens were analyzed for the presence of collagen fibers derived from vascular walls. The banded collagen fibers with distinct boundary existing at the margin or outside of the thrombus were defined as pieces of vascular wall (vascular wall components (VWCs)). Organized thrombus was defined as having an unclear boundary and complicated fibrosis seen in part of the thrombus (see online supplementary figure II). When there were VWCs that could be confirmed at 100× magnification, the specimen was considered VWC positive, even if very small. When VWCs existed, Elastica van Gieson staining was added to verify the presence of the internal elastic lamina (IEL), implying extension of the vascular injury to the tunica media. Additionally, their thickness and area were measured with an optical microscope at 12.5× to 400× magnification, depending on the size of the VWCs. The area of the VWC was measured by plotting the margin of the VWCs manually in a slice stained with Masson’s trichrome. If the collagen fiber was one layer, the short diameter of the VWC was measured as the thickness, and in the case of folded multiple layers, the thickness of one layer was measured (see online supplementary figure II). Then, the ratios of erythrocyte components and of fibrin/platelet components were quantified in a manner previously reported.16 The histological analysis was performed using an Olympus BX51 microscope and image analysis software (cellSens Standard; Olympus, Tokyo, Japan).
Supplementary file 1
Statistical analysis
Patient clinical information and the characteristics of the specimens were compared between the groups whose specimens were VWC positive and VWC negative. In addition, the characteristics of VWCs obtained by ADAPT were compared with those obtained by SRs. Variables were analyzed using Fisher’s exact test or Pearson’s χ2 test for categorical data, the Wilcoxon Rank Sum test or the Kruskal–Wallis test for continuous data, and the Cochran Armitage Trend test for trend, as appropriate. For all statistical analyses, P<0.05 was considered significant. Statistical analysis was conducted using JMP 12 software (SAS Institute, Cary, North Carolina, USA).
Results
Patient data
In total, 131 consecutive patients with acute ischemic stroke were treated with endovascular therapy at our institute from 1 November 2013 to 30 April 2016. Of these patients, 101 (47 women, age 74.9±11.1 years) were enrolled in this study (see online supplementary figure I). The clinical characteristics of the study population are shown in table 1.
Clinical characteristics and therapeutic process of the study population
Endovascular treatment
Of the 101 patients, 42 were treated with ADAPT, 31 with unsuccessful ADAPT followed by thrombectomy with SRs, 21 with SRs, and 7 with unsuccessful thrombectomy with SRs followed by ADAPT. The following SRs were used: Solitaire FR (Covidien/ev3, Dublin, Ireland) (49 patients), Trevo XP ProVue Retriever (Stryker Neurovascular, Mountain View, California, USA) (2 patients), Trevo ProVue Retriever (Stryker Neurovascular) (13 patients), and REVIVE SE (Codman Neuro/DePuy Synthes, Johnson and Johnson, Raynham, Massachusetts, USA) (3 patients). Thrombectomy with SRs was performed with the Penumbra aspiration catheters as a combined stent aspiration technique in 44 patients.
Histopathological outcomes
VWCs were present in 24 specimens from 22 of 101 patients (22%). The proportion of current smokers tended to be lower (30% vs 53%, P=0.07), the frequency of device reaching distally (the M2 portion of the middle cerebral artery, the P2 portion of the posterior cerebral artery, or more distal) tended to be higher (77% vs 56%, P=0.07), and the number of device passages tended to be greater (median 2 (IQR 1–5) vs 2 (1–3), P=0.08) in the VWC positive group than in the VWC negative group (table 1).
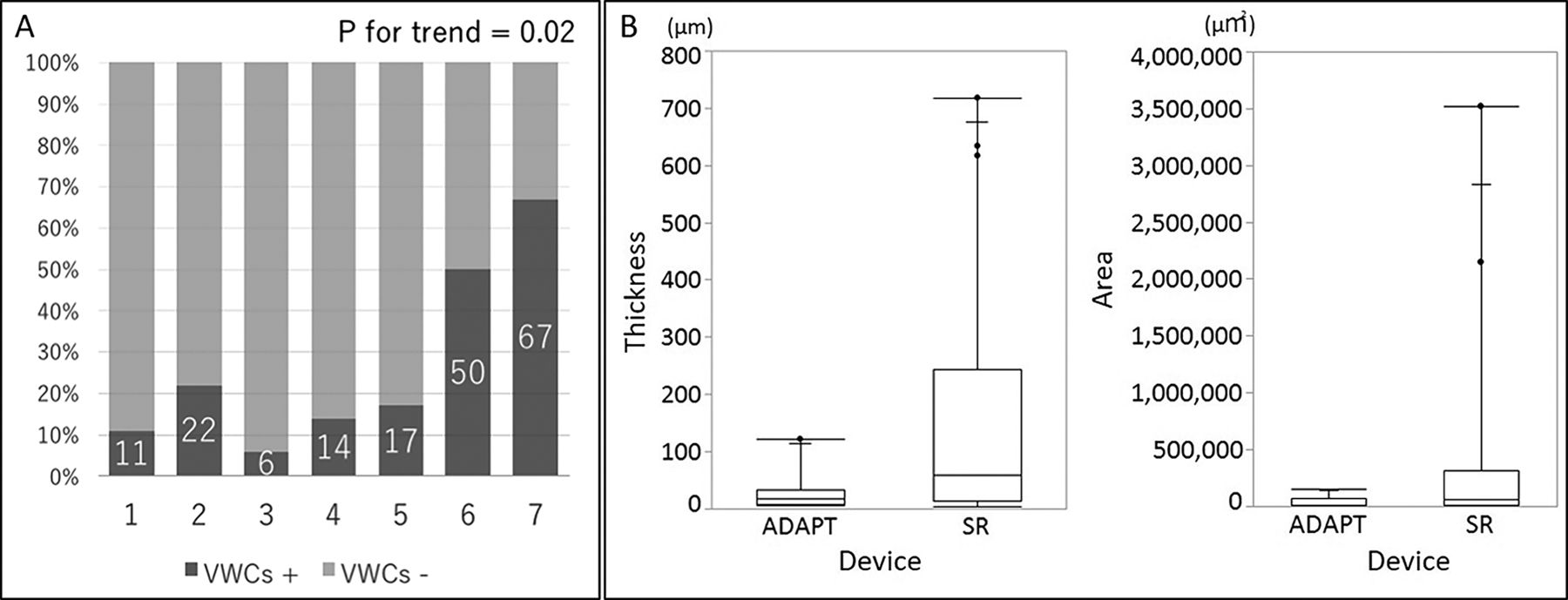
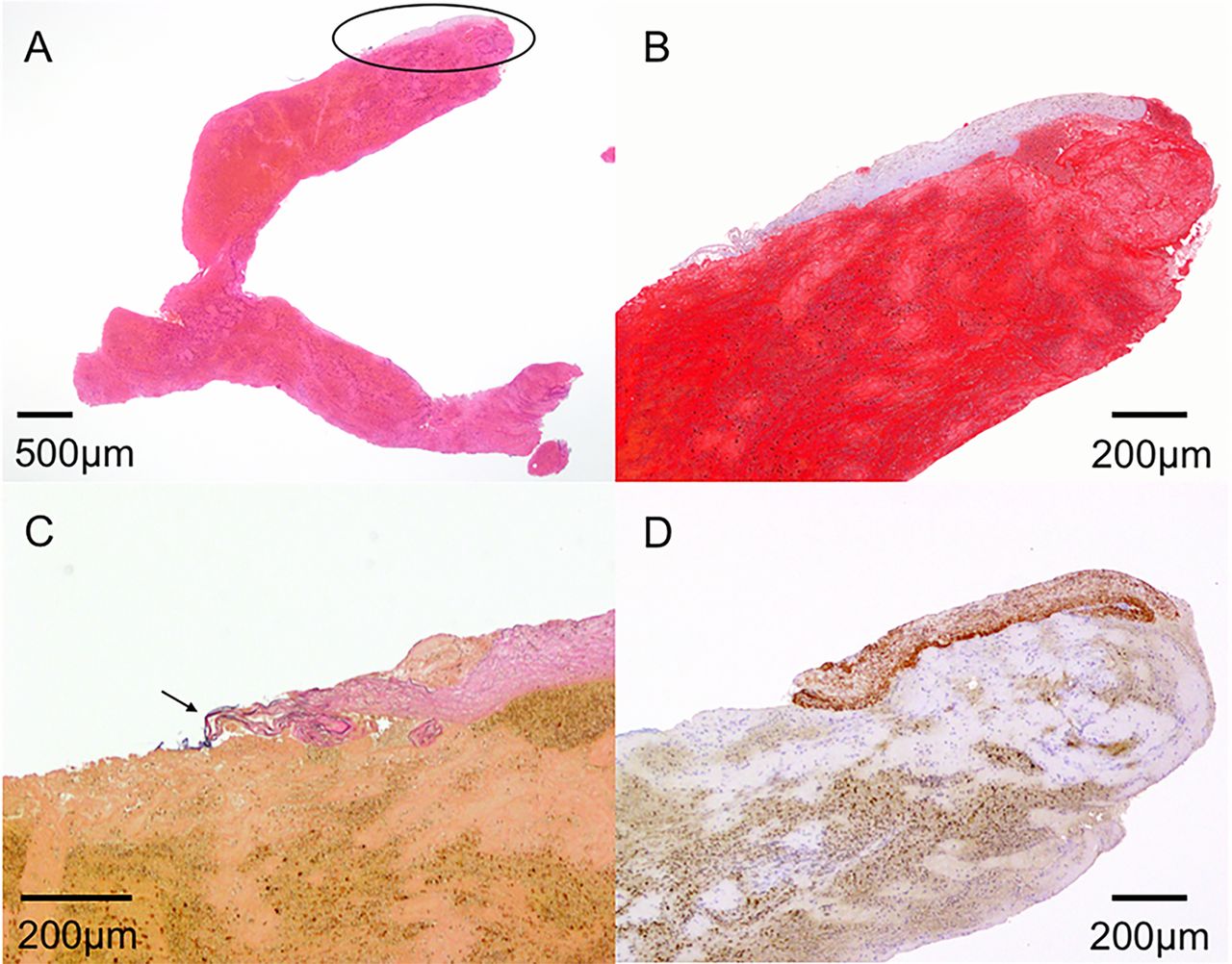
In the analysis of each specimen, VWCs were present in 24 (16%) of a total of 150 specimens. Elastica van Gieson staining was added for VWC positive specimens; of these, 12 specimens (50%) from 11 patients included IEL in the VWCs (figure 1), 7 other specimens did not include the IEL, and VWCs could be no longer identified in additional sections in the remaining 5 specimens. The proportion of erythrocyte components was lower (41.7±24.8% vs 55.0±26.3%, P=0.01) and the proportion of fibrin/platelet components was higher (57.9±24.8% vs 44.3±25.7%, P=0.01) in VWC positive thrombi than in those without. The rate of VWCs increased in proportion to the number of device passages (figure 2A). When the device reached distally, VWCs were frequently observed (table 2).
Histopathologic analysis of each specimen
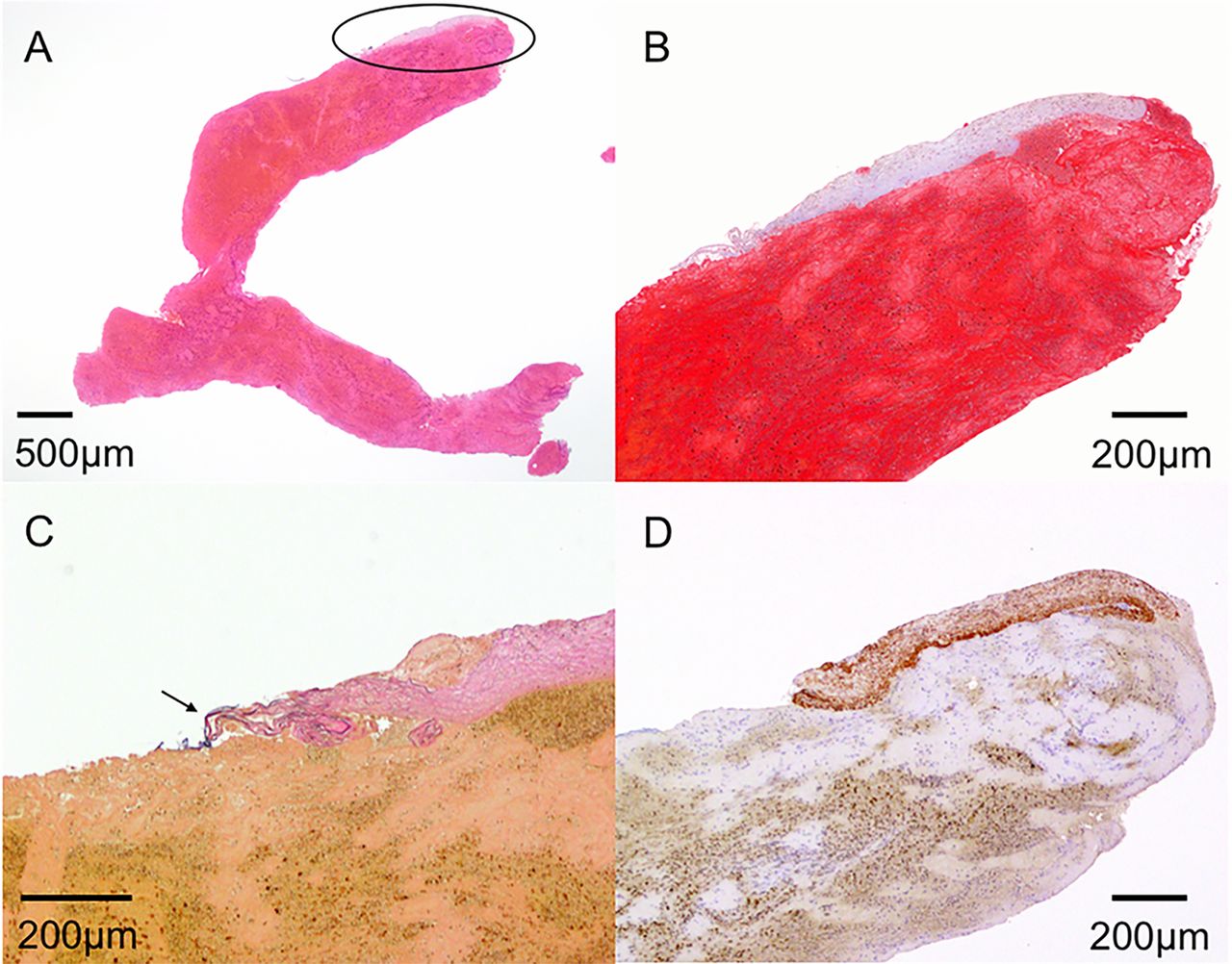
Photomicrograph of the vascular wall component retrieved with thrombus. (A) A piece of collagen fiber attached at the edge of the thrombus (ellipse); hematoxylin–eosin, original magnification ×12.5. (B) Magnified image of a piece of collagen fiber at the edge of the thrombus; Masson’s trichrome, original magnification ×40. (C) A piece of collagen fiber, including the internal elastic lamina; Elastica van Gieson, original magnification ×100. (D) A piece of collagen fiber, including smooth muscle cells; immunohistochemical staining for α-smooth muscle actin, original magnification ×40.
{kind=link}
{kind=link}
(A) Relationship between the number of device passages and the proportion of retrieved thrombi with vascular wall components (VWCs). The rate of VWCs increases in proportion to the number of device passages. The number of device passages was counted consistently during the procedure, regardless of the type of device. (B) Associations between thickness, area of vascular wall components, and mechanical thrombectomy devices. Area and thickness of vascular wall components tend to be larger in specimens retrieved by stent retriever (SR) than in those retrieved by Penumbra (ADAPT).
Thickness (59.0 (13.8–244.3) µm vs 18.0 (8.8–34.3) µm, P=0.17) and area (57659 (6206–318 623) µm2 vs 5441 (2075–75 360) µm2, P=0.11) of VWCs tended to be larger in specimens retrieved by SRs than in those retrieved by ADAPT (figure 2B, supplementary table I).
Angiographic and clinical outcomes
Successful reperfusion tended to be obtained less frequently (73% vs 89%, P=0.06) in the VWC positive group than in the VWC negative group. In the present study, a higher proportion of erythrocyte components (58.4±24.3% vs 42.4±25.3%, P=0.02), less frequent multiple MT device usage (31% vs 73%, P=0.003), and less frequent device passages (2 (1–3) vs 3 (2–6), P=0.005) were associated with successful reperfusion on univariate analysis (see online supplementary table II). After multivariate adjustment, a higher proportion of erythrocyte components was the sole independent predictor of successful reperfusion (OR 1.03, 95% CI 1.00 to 1.05). The occurrence of ICH or SAH alone was not statistically different between the groups (table 1).
Discussion
SR and ADAPT using the Penumbra aspiration catheter have achieved higher recanalization rates, lower complication rates, and better clinical outcomes.1–9 However, there are some reports of vascular injury caused by SR and ADAPT.2–9 The incidences of SR related complications in the pivotal randomized controlled trials were as follows: SAH 0.6–4.9%, intraventricular hemorrhage 1%, vessel dissection 1.7–3.9%, vessel perforation 0.6–4.9%, and vasospasm 3.9–4%.3–8 In the Contact Aspiration vs Stent Retriever for Successful Revascularization (ASTER) study, the rates of procedure related adverse events caused by ADAPT were as follows: SAH 6.9%, vasospasm 2.6%, arterial perforation 2.6%, and arterial dissection 2.6%, with no significant differences compared with patients treated with SR.9
The rates of any ICH or SAH in the present study, 36.6% and 16.8%, respectively, seemed high. Since ICH on MRI was included, the proportion of ICH would have been higher. The rate of any ICH at 24 hours was, however, approximately 46% in the ASTER study,9 being equivalent to or higher than that in the present study. The rate of SAH in the present study was higher than in the pivotal randomized controlled trials,3–8 but almost equal to the rate in a Korean observational study reported by Yoon et al (16.2%).10
In animal studies, Gory et al12 reported that the Merci, Catch Thromboembolectomy System, Solitaire FR, and Penumbra caused endothelial denudation, medial layer edema, and mural thrombus in swine superficial femoral artery models. It has also been reported that arterial wall damage decreased in vessels with clots when using SR, indicating that the length of the device should be close to the length of the clot to reduce the surface area in contact with the vessel wall.12 Among the thrombectomy devices, Penumbra created less endothelial denudation and mural thrombus than the other wall contact device samples in animal models and in an in vitro live cell platform.12–14 Teng et al13 reported that the degree of vascular endothelial cell injury was related to vessel diameter, suggesting the importance of applying devices that properly match the dimensions of the vessels.
To assess the histological changes occurring in the arterial wall following MT in human cerebral arteries directly is difficult, but analyzing the specimens retrieved by MT helps to gauge the histological changes occurring in the arterial wall.
Singh et al found CD34 positive endothelial cells derived from blood vessels in 11 of 48 thrombi retrieved by SRs, without any attached subendothelial connective tissue.19 On the other hand, half of the VWC positive specimens (8% of total thrombi obtained) included the IEL in this study. Older age (mean age 74.9 years vs 67 years) and a higher proportion of East Asian patients, who are more likely to be affected by intracranial atherosclerosis than patients of other races,20 in the present study may be causal factors responsible for the difference in the detection rate of subendothelial connective tissue between the studies. Furthermore, arterial tortuosity and a small sized artery are thought to be caused by intracranial atherosclerosis, and a Japanese study showed that the horizontal segment of the middle cerebral artery tended to be angulated sharply in acute stroke patients who underwent MT.21 Excessive tortuosity constrains effective delivery of the device and exertion of retraction force.21 22 In addition, atherosclerotic change and tortuousness could extend the frequency and depth of vascular injury during MT.23 24 East Asian patients, including Japanese, with acute large vessel occlusion may be more vulnerable to MT than patients of other races in the light of vessel wall injury.
From the present results, vascular injury caused by MT in human cerebral arteries seemed to expand deeper than reported in animal models.12 14 There are some reasons that can be inferred. One of the reasons is the structural characteristics of human intracranial arteries. Intracranial arteries have a lower wall to lumen ratio than extracranial arteries, as the vessel wall of human cerebral arteries is thinner than that of animal models with similar vessel diameters. In addition, there have no external elastic lamina between the media and adventitia, and the adventitia is very thin compared with vessels of similar luminal diameter in other parts of the body.25 There are essential structural differences between human cerebral arteries and animal extracranial arteries, and human cerebral arteries are more delicate. Also, the arteries in animal models do not have atherosclerotic changes and tortuousness, whereas there may be atherosclerotic change in patients’ cerebral arteries, especially in East Asian patients, as mentioned above.20 In fact, VWCs observed in the present study included fibrous caps of plaque.
Histopathology of occlusive thrombi, number of device passages, and arterial sites where devices reached were associated with the presence of VWCs in retrieved thrombi. As confirmed in the present study, we previously reported that erythrocyte-rich thrombi were positively associated with successful reperfusion after thrombectomy.16 An increased number of device passages against distal fibrin/platelet-rich thrombi could lead to vascular injury.
There may be a way for a clinician to estimate the presence of VWCs before thrombectomy. It has been reported that the absence of the hyperdense middle cerebral artery sign (HMCAS) on CT or the susceptibility vessel sign (SVS) on gradient echo MRI may indicate fibrin predominant occlusive thrombi or atherothrombotic in situ occlusion.26 27 When treating occlusion of the distal part of the M1/P1 with absence of HMCAS or SVS, there would be a risk of vessel injury. In that situation, it may be important to select the correct thrombectomy device in terms of length and dimensions, or the correct reperfusion strategy, not thrombectomy but angioplasty with or without stenting.
The thickness and area of the VWCs tended to be larger in specimens retrieved by SRs. As demonstrated previously using animal models,12–14 the extent of vascular damage seemed different between thrombectomy devices in the real clinical setting. These differences are probably explained by variations in the designs and mechanisms of the devices. The aspiration catheter applies aspiration force to the proximal base of the thrombus. On the other hand, wall contact devices (SRs) capture the clot by exerting continuous radial force against the arterial wall, having more surface area in contact with the vascular wall. Furthermore, they require repositioning and passing procedures. The aspiration devices appeared to reduce irritation in the arterial wall, thus lowering the risk and severity of vascular injury.12 28 There was, however, an important bias in the present study. The results of the SR group might reflect a higher number of passages and higher complexity of retrieval procedures because ADAPT was the firstline procedure, and SRs were frequently used as a bail-out procedure in the majority of the study period.
In addition to the above mentioned issues, there are several limitations of the present study. This was a single center, retrospective study with self-assessed data. There may be inherent selection bias. The thrombi retrieved from intracranial vessels in many cases are friable and decompose before being sampled in formalin. Therefore, the observed specimens are not always representative of the entire thrombus. In particular, thrombi are often stuck within the SRs and need to be mobilized and tend to fragment during this process, which may be a potential procedure specific bias. VWCs obtained with thrombus were so small that there could be false negatives in this study, and it was difficult to obtain enough specimens for several types of stains. It was also difficult to evaluate the quantity of the VWCs accurately.
Conclusion
In this study of retrieved specimens with MT, both ADAPT and SR devices caused various vascular injuries. The ratio of erythrocytes of occlusive thrombi, arterial sites where devices reached, and the number of device passages might affect the presence of VWCs in retrieved thrombi from acute stroke patients. Further studies are essential to confirm the clinical effects of these findings.
References
Footnotes
Contributors Study conception and design: NF and MH. Drafting the article: NF. Revising the manuscript critically for important intellectual content: MH, HI-U, and KT. Acquisition of the data: all authors. Technical/material support: TH, HY, TS, JCT, KN, and HI-U. Analysis and interpretation of the data: all authors. Study supervision: HY, TI, and KT. Final approval of the version to be published: all authors.
Funding This work was supported by the Japan Society for the Promotion of Science, Grant in Aid for Scientific Research (C) 15K10381, and by the Japanese Society for Neuroendovascular Therapy.
Competing interests None declared.
Patient consent Not required.
Ethics approval The study was approved by the research ethics committee of the National Cerebral and Cardiovascular Center.
Provenance and peer review Not commissioned; externally peer reviewed.