Article Text

Abstract
Background Ischemic stroke research faces difficulties in translating pathology between animal models and human patients to develop treatments. Mechanical thrombectomy, for the first time, offers a momentary window into the changes occurring in ischemia. We developed a tissue banking protocol to capture intracranial thrombi and the blood immediately proximal and distal to it.
Objective To develop and share a reproducible protocol to bank these specimens for future analysis.
Methods We established a protocol approved by the institutional review board for tissue processing during thrombectomy (www.clinicaltrials.gov NCT03153683). The protocol was a joint clinical/basic science effort among multiple laboratories and the NeuroInterventional Radiology service line. We constructed a workspace in the angiography suite, and developed a step-by-step process for specimen retrieval and processing.
Results Our protocol successfully yielded samples for analysis in all but one case. In our preliminary dataset, the process produced adequate amounts of tissue from distal blood, proximal blood, and thrombi for gene expression and proteomics analyses. We describe the tissue banking protocol, and highlight training protocols and mechanics of on-call research staffing. In addition, preliminary integrity analyses demonstrated high-quality yields for RNA and protein.
Conclusions We have developed a novel tissue banking protocol using mechanical thrombectomy to capture thrombus along with arterial blood proximal and distal to it. The protocol provides high-quality specimens, facilitating analysis of the initial molecular response to ischemic stroke in the human condition for the first time. This approach will permit reverse translation to animal models for treatment development.
- thrombectomy
- stroke
- technique
- inflammatory response
Statistics from Altmetric.com
Ischemic stroke remains a major cause of death and disability worldwide.1 2 Standard treatment of acute ischemic stroke now focuses on recanalization of the occluded intracranial vessel, and includes the use of tissue plasminogen activator and mechanical thrombectomy.3–5 Although other strategies such as neuroprotection, neurorepair, and stem cell therapy have been explored,6–8 none have thus far yielded a therapeutic standard.
Challenges with translating therapeutic targets from animal models to human disease have impaired this progress. These studies relied primarily on finding drug targets in animal models, and then extrapolating those same targets to the human condition. However, animal models have been inadequate in simulating the human patient with stroke. In the animal models, most studies have not included the modeling of animals with comorbid conditions, have not accounted for age and sex effects, and preclinical trial designs were inadequate.9–11 Furthermore, IV tissue plasminogen activator effects and mechanical thrombectomy in human patients are also difficult or impossible to model in small animals.
From the clinical perspective, human trials of neuroprotective therapies have historically faced problems of delayed timing of therapy, lack of pairing with successful recanalization, and heterogeneity of the included population.12 While significant efforts have been undertaken to overcome these challenges, the interspecies translational barrier remains; most neuroprotective therapies are based on targets from animal studies. Until now, there has been little opportunity to evaluate the biochemical and molecular environment of the human brain during a stroke, which would provide insight into therapeutic targets based on the human response to this pathology.
Since 2015, mechanical thrombectomy (MT) has become a standard treatment for emergent large vessel occlusion stroke. Multiple clinical trials demonstrated the benefit of endovascular recanalization of the occluded vessel in the anterior circulation, and newer trials continue to expand the inclusion criteria of this treatment.4 5 13–17 Thus, as indications for thrombectomy expand, more patients will undergo the procedure. In this setting, there has been early interest in evaluating the thrombi removed during the procedure.18 19 As noted, most of the current work has focused on histopathology of the thrombus, and not yet thoroughly evaluated the molecular milieu of the thrombus and surrounding intraluminal blood. It is crucial to do this, as stroke is as much a biochemical problem of the vasculature and parenchyma as it is a focal vascular anatomic concern.
During our standard technique, we recognized that the thrombus, along with blood proximal and distal to it, is removed and discarded. We have recognized the potential importance of this tissue in the evaluation of stroke in the human condition. A tissue banking protocol has been created through collaboration among multiple research laboratories within our Center for Advanced Translational Stroke Science and our NeuroInterventional Radiology (NIR) service line. We sought to design a banking protocol that would provide high-quality yields of fresh tissue amenable to multiple analytic studies (eg, blood gas/electrolytes, proteomic, and gene expression analyses). The aim of this study was to design the banking protocol, which includes determining the supplies and staffing required, optimizing protocols for research notification, and demonstrating high-quality tissue preservation.
Methods
Tissue removal
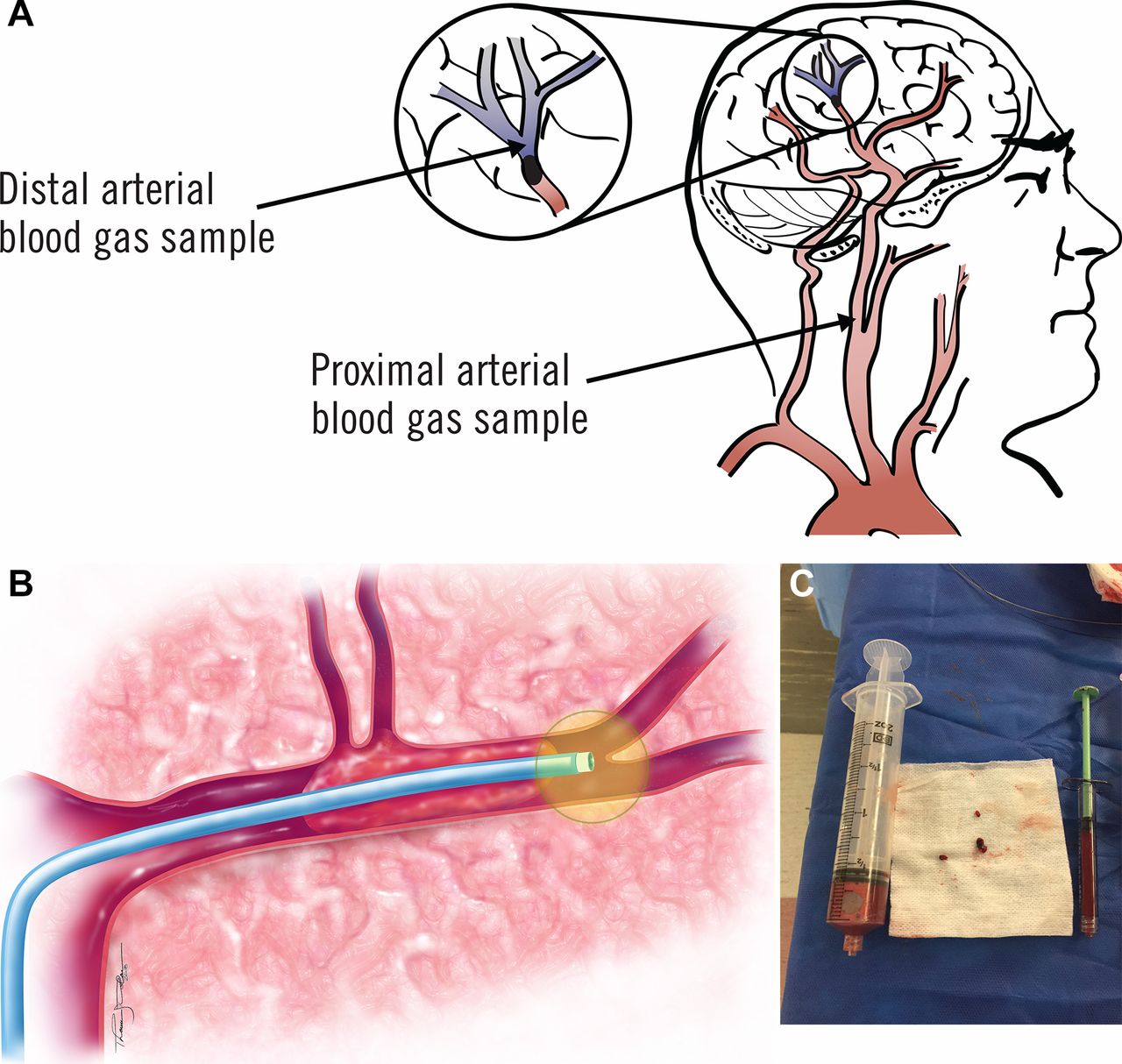
Tissues for banking were those removed during standard thrombectomy. During MT, we navigate through the thrombus with the microwire and microcatheter. We routinely use a microcatheter with a 0.021 inch inner lumen diameter for access. The microcatheter is navigated distal to the thrombus, and we check for back-bleeding through withdrawal with a 1 cc microsyringe. We generally avoid superselective contrast injection to confirm the position of the microcatheter. Thus, the blood that we withdraw is collected in the Blood And Clot Thrombectomy Registry And Collaboration (BACTRAC) protocol. We also perform suction through the guide or distal access catheter during thrombectomy, resulting in removal of systemic arterial blood. These collections, along with the thrombus itself, were routinely discarded before our research protocol (figure 1). The BACTRAC protocol uses these specimens for collection and banking. Of note, we process only proximal and distal blood taken during the first pass of thrombectomy. This is to avoid any possible contamination between proximal and distal blood that might occur if the first pass caused a partial communication across the clot. Blood specimens are processed even in cases where no clot is retrieved or saved. The only case where no blood is taken is that in which the vessel is open at the time of angiography before thrombectomy. All retrieved clot from any pass is pooled.

(A) Illustration of tissues removed during mechanical thrombectomy for banking. (B) Intracranial samples include the thrombus and blood just distal to it. (C) The specimens collected. These include up to 1 mL of distal blood, the thrombus, and the proximal blood, which varies depending on the suction applied just before thrombectomy.
Tissue banking protocol
We designed a tissue banking protocol that could be seamlessly incorporated into the standard workflow of the mechanical thrombectomy procedure. Initiation of the tissue bank was undertaken with institutional review board approval, and the study was registered with www.clinicaltrials.gov (NCT03153683). The protocol was designed by the multidisciplinary team of the NIR service line combined with the laboratories of the Center for Advanced Translational Stroke Science at our institution. The protocol and workflow were designed to optimize quality and integrity of tissue for electrolyte/blood gas analysis, proteomic, and gene expression analyses. The clots were processed in a way to preserve them for any potential histology analysis as well. To facilitate tissue processing, a laboratory space was created in a wet room adjacent to the NIR angiography suite control room. A centrifuge Microfuge 22R centrifuge (Beckman Coulter Inc; Indianapolis, Indiana, USA) was placed in this workspace, along with tube racks, and extra tubes: Wheaton CryoELITE cryogenic vials (DWK Life Sciences; Millville, New Jersey) (blue, yellow, and green tubes), BD Microtainer Z tubes (no additive; Becton, Dickinson and Company; Franklin Lakes, New Jersey) (red tubes), and BD Microtainer tubes with K2E (K2EDTA; Becton, Dickinson and Company) (lavender tubes).
Inclusion criteria for BACTRAC tissue banking are as follows: the patient or the legally authorized representative provides consent for the study preprocedurally or within 24 hours after the procedure; male or female, aged ≥18 years; suspected acute ischemic stroke based on clinical and radiographic evidence; subjects must meet criteria for intra-arterial thrombectomy as determined and documented at the NIR faculty; subjects must have an acute thromboembolus within an intracranial artery, which undergoes MT; subjects with impaired capacity may be included as the pathology to be studied (stroke) may weaken their capacity; subject must undergo thrombectomy; for women of reproductive age, a urine pregnancy test at baseline must be negative. Large vessel occlusion strokes during pregnancy are relatively rare, but the presence of pregnancy was deemed to be a major confounding variable for analysis.
Tissue integrity analysis
The plasma samples undergo proteomics analysis to determine the protein expression in the blood. This analysis confirms the gene expression results. Second, the analysis determines the expression of proteins that are not dependent on upregulation of gene expression, but are increased by molecular mechanisms, such as mRNA stabilization, which enhance translation of proteins. To analyze integrity for proteomics analysis, the first subject samples of both distal and proximal blood were analyzed by Olink Proteomics (www.olink.com) to demonstrate viability of the plasma for this method. A 30 µL plasma protein aliquot from each sample was sent to Olink; only 1 µL is required for the analysis for each panel. Duplicates of these samples passed quality control, and were run on all 11 of their proteomic panels (92 proteins/panel) for a total of 1012 proteins. An intra-assay coefficient of variance (%CV) was determined in our sample by comparing test samples with internal control samples provided by the Olink assay. The reference value for intra-assay %CV is <15%. Samples below that threshold are homogeneous, indicating a precise assay.
RNA was isolated from seven thrombi using RNeasy Mini Kit (Qiagen, Germantown, Maryland). RNA was extracted from eight distal and peripheral blood samples using a Nucleospin RNA blood kit (Nucleospin, MACHEREY-NAGEL, Düren, Germany) following manufacturer protocols. The quantity of total RNA, based on a A260/A280 ratio, was estimated using a Nanodrop Lite spectrophotometer (Thermo-Fisher Scientific; Waltham, Massachusetts). RNA integrity was assessed using the Eukaryote Total RNA Nano assay on the Agilent 2100 bioanalyzer (Agilent Technologies, Santa Clara, California). After analysis, RNA integrity numbers (RINs) were calculated using the software associated with the Agilent 2100 bioanalyzer.
Clinical and radiographic endpoints
In addition to the tissue, the BACTRAC protocol records clinical and radiographic variables. Clinical variables recorded include: age, sex, race/ethnicity, height, weight, body mass index, premorbid modified Rankin score, location of thrombus, estimated source of thrombus (cardioembolic, intracranial stenosis, dissection carotid occlusion, infection, unknown), presence of tandem occlusion, time from last known normal to thrombectomy completion, IV thrombolysis given versus not given, Thrombolysis in Cerebral Infarction score, National Institutes of Health Stroke Scale score at discharge, modified Rankin score (at discharge and 90 days after treatment), and mini-Montreal Cognitive Assessment (at discharge and 90 days after treatment). Radiographic variables are assessed by an independent neuroradiologist (DEL) not involved in performance of thrombectomy, data analysis, or tissue evaluation. These endpoints include: volume of infarct, grading of intracranial hemorrhage (based on the European Cooperative Acute Stroke Study II scale20 21), and volume of cerebral edema.
Results
Protocol construction and workflow
The tissue processing protocol is illustrated in figure 2. The supplies required by the researcher are stocked in the angiography workspace and include: all required personal protective equipment (gloves, eye protection, and lead); centrifuge; 200 µL fixed pipette and tips; wet ice, Kimwipes, extra tubes, labels, collection cards; PDI Super Sani cloth wipes for clean-up; sterilely wrapped scissors and forceps; and biohazard/sharps containers for all contaminated trash. The researcher brings a small cooler of dry ice from the tissue banking laboratory with them for transfer of specimens back to the laboratory.

Workflow for tissue processing. This shows a step-by-step visualization of the tissue banking protocol. ABG, arterial blood gas; DB, distal blood; PB, proximal blood.
The on-call researcher carries a pager, which is activated with the ‘thrombectomy activation’ page. Institutionally, when an NIR faculty member approves a thrombectomy procedure, a ‘thrombectomy page’ is sent to all team members (nurses, technicians, and stroke coordinators) to activate the procedure. This page includes activation to the on-call researcher. On receiving the page, the collector (on-call researcher) fills a small ice cooler with dry ice (approximately 1 inch layer of crushed dry ice) from the tissue banking laboratory, and proceeds to the angiography suite. The collector is expected to be within 30 min of the hospital to ensure appropriate response time. Blank study folders are maintained immediately outside the angiography suite. On thrombectomy activation, the NIR faculty member completes the inclusion/exclusion criteria sheet in the study folder, verifying the patient as a potential subject. The collector retrieves a prepared bag of prelabeled tubes for the subject contained within the study folder. The tubes are prelabeled with the study ID number (not associated with any personal health information) and sample type. Collectors are not required to enter the angiography suite, but if they do, they are required to don appropriate clothing (scrubs/bunny suit, cap, mask, and lead if needed).
The NIR faculty provides up to three samples when possible: proximal blood (PB) usually in a large syringe (20 or 60 mL from suction); distal blood (DB) in a 1–3 mL syringe; thrombus handed off on disposable gauze. PB and DB samples (500 µL (0.5 mL)) are placed into standard hospital blood gas kits and sent to the hospital’s central laboratory for blood gas/electrolyte analysis. The remaining DB is placed in a K2EDTA lavender blood tube with an orange label, inverted 10 times to mix, and then processed along with the PB tubes. It is important to keep the volume of blood in each tube between 250 and 500 µL, as, otherwise, the EDTA concentration will not be correct, and the various components of blood will not fractionate correctly. The remaining PB is separated into 500 µL aliquots in tubes as indicated: K2EDTA lavender blood tubes at 500 µL each (inverted 10 times to mix), and two red-top blood tubes to be used for serum to 500 µL (inverted six times and allowed to clot at room temperature for 30 min). All DB and PB K2EDTA blood tubes are centrifuged at 2000 g for 15 min. During this centrifuge, the clot is split into three pieces using sterile instruments, and placed into three labelled blue cryotubes, and then flash-frozen on crushed dry ice. When the centrifugation is complete, 200 µL is taken off the plasma layer using a fixed 200 µL pipette and put into a cryotube (green for DB and yellow for PB), leaving the cellular pellet and the buffy coat in the bottom of the lavender tube. Care must be taken to not disturb the buffy coat/pellet when pulling off the plasma. This is repeated for all lavender tubes. Extra tubes are available if needed or if a tube becomes damaged. All green/yellow (plasma) and lavender (pellet/buffy coat) tubes are flash-frozen on crushed dry ice. The red clotted tubes (after 30 min) are placed on wet ice.
All tubes are transported to the laboratory, where the red tubes are placed into a 4°C refrigerator, while all other tubes are placed into a dedicated secure BACTRAC −80°C freezer. A database tracks the samples from entry into the freezer (study ID, sample type, quantity, date, and collector) until removal (individual, research laboratory, affiliation, study ID, type, quantity, and date). The red tubes are also recorded to keep track of the tube samples that were collected.
To ensure both high-quality specimens and subject confidentiality/proper consent process, we instituted several protocols for training of collectors, and processing of specimens (online supplemental Figures 1 and 2). We began with several ‘superusers’, who were researchers participating directly in the formulation of the tissue banking process. They became trainers, overseeing and monitoring the process performed by other researchers. We instituted these policies to ensure quality and consistency in the samples obtained. Second, as previously described, given that these samples were removed during the standard course of the thrombectomy procedure, our institutional review board allowed 24 hours for consent to be given. If consent was not obtained, all samples and experiments/results derived from them were destroyed. To ensure and document such destruction, we created a standard document for this process (online supplemental Figure 2). This maximized the integrity of informed consent.
Supplementary file 2
Integrity analysis
The first patient sample of both DB and PB was analyzed by Olink Proteomics (www.olink.com) to demonstrate viability of the plasma for this proteomic method. Duplicates of these samples passed quality control, and were run on all 11 of their proteomic panels (92 proteins/panel) for a total of 1012 proteins (table 1). One hundred percent of proteins were detected on cardiovascular iii and oncology ii panels, while 99% of proteins were detected on the neurology panel. The organ damage panel detected the fewest, with 61% of proteins detected. The cardiometabolic and cardiovascular iii panels each showed the most proteins with the greatest differences in expression. Furthermore, 10 of 11 panels had %CV below the 15% threshold, with only the cardiometabolic panel deviating to 17%.
Olink proteomics analysis listed by panel
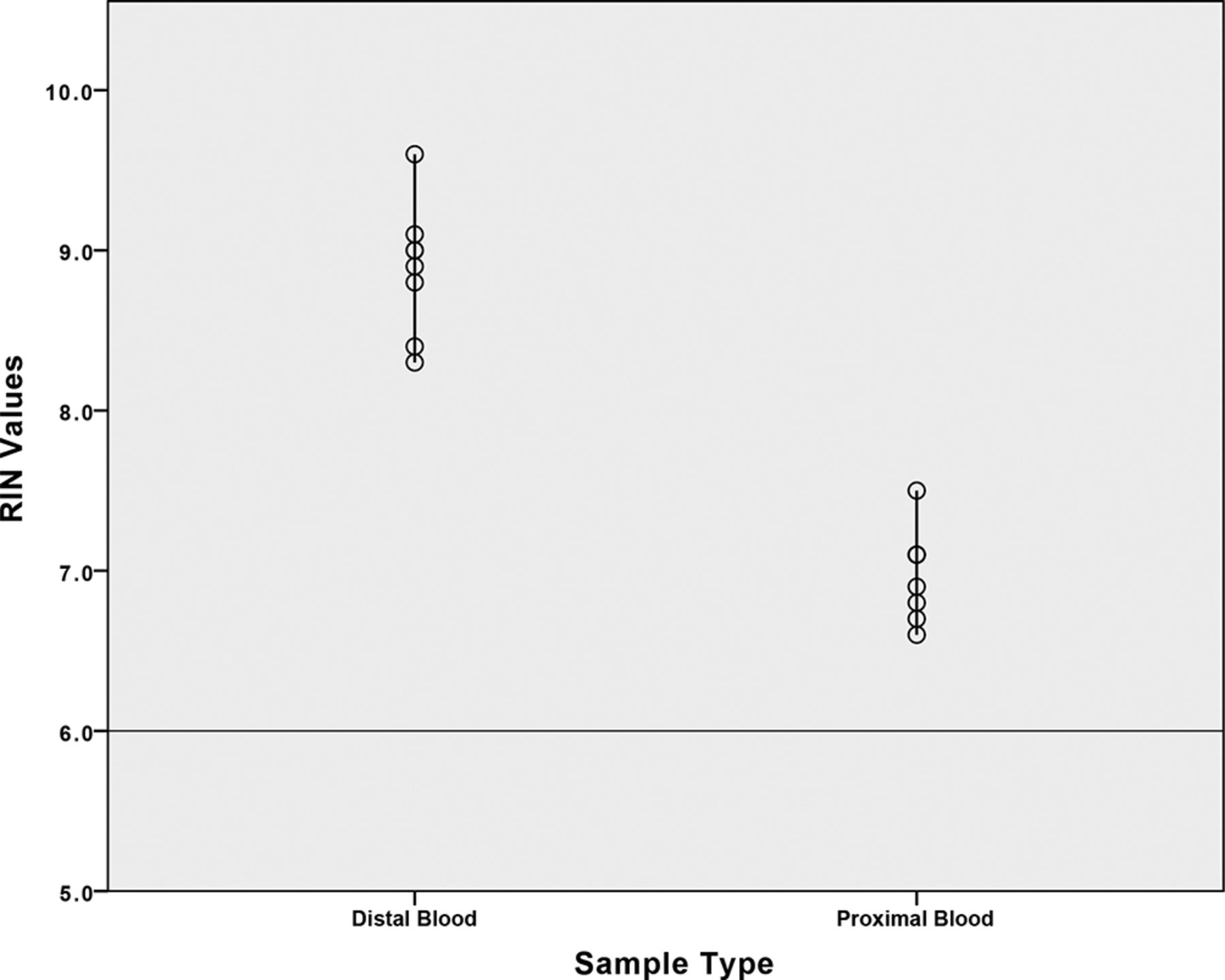
Total RNA preparations were made using Agilent 2100 bioanalyzer. Mean RIN values (±SD) for distal arterial blood were 8.89±0.41 (range from 8.30 to 9.60), indicating high-quality RNA with minimal degradation (figure 3). Mean RIN values (±SD) for proximal arterial blood were 6.98±0.29 (range from 6.60 to 7.50), indicating moderate quality of RNA with minimal degradation (figure 3). Mean RIN values for the thrombi were undetectable. The Agilent 2100 bioanalyzer showed that the total RNA extracted from thrombi samples contained a large peak between 18S and 28S peaks, which is typically genomic DNA.
{kind=link}
{kind=link}
{kind=link}
RNA integrity number (RIN) analysis. Individual samples were plotted on this distribution plot for proximal and distal blood. In both cases, the RIN values were all above the 6.0 threshold, indicating appropriate and adequate quality RNA.
Discussion
Translation of therapies from animal models to humans in acute ischemic stroke has been suppressed by heterogeneity of the patient population, complexities related to medical comorbidities, variations in animal models used, and design of preclinical experiments.9 12 Modeling human stroke in animals can be particularly problematic. Problems include, but are not limited to, the effect of cerebrovascular anatomic variations, comorbidities, and stroke subtypes on neurocritical care needs.22–27 Furthermore, different subtypes and the presence of comorbidities can affect the cellular and molecular responses to the injury. Given these factors, it is critical to develop methodologies for studying stroke pathology actively in human patients. These findings can be used to translate back to animal models to improve therapeutic approaches to stroke using pharmacological targets from human patients with stroke. We developed the BACTRAC tissue bank to meet this need. The goal of the bank is to catalog tissues from patients with emergent large vessel occlusion stroke, paired with radiographic and clinical data, in order to facilitate evaluation of molecular/cellular changes under conditions of known patient and outcome variables. To implement such an apparatus, our immediate goal was to streamline the mechanics of tissue collection/processing, and verify the integrity of the samples obtained.
To guide our efforts, we referred to current and previous evaluations of human components of stroke. Simons et al evaluated correlations between a hyperdense artery sign and thrombus composition in 40 subjects They found that the radiographic sign was associated with early phase clot pathology.28 Niesten et al evaluated red blood cell, platelet, and fibrin compositions of 22 subjects after thrombectomy, assessing relationships with stroke subtype.29 Dargazanli et al evaluated the presence of CD3+ T cells in the thrombi removed during thrombectomy, in relationship to stroke subtype.30 These studies primarily focused on the histological composition of the thrombus, with no effort to routinely salvage protein and RNA for analysis. Proteomics and gene expression analyses provide windows into pathways of injury, and highlight potential areas for therapeutic intervention. Furthermore, we can use the integrity of protein and RNA in our samples to verify the quality of tissue obtained, reflecting the controlled and reproducible nature of the banking protocol.
To our knowledge, only one other group has evaluated blood distal to an intracranial thrombus during stroke. Flores et al evaluated blood gas parameters in samples drawn in 16 subjects undergoing endovascular recanalization procedures.31 This process provided insight into how tissue collection could be incorporated into standard thrombectomy. The authors obtained the specimen, and then injected contrast superselectively to verify microcatheter position distal to the clot. There is some evidence that these microinjections can increase the risk of intracranial hemorrhage.32 We routinely use microsuction through the microcatheter to confirm location distal to the thrombus, and to ensure no perforations or dissections. In such a way, we use tissues already lost in the process of thrombectomy. While circulating peripheral arterial and/or venous blood could be previously studied in acute stroke, this availability of distal blood is unique to thrombectomy patients. Furthermore, unlike these previous studies, our process required specific training for researchers performing tissue processing and banking, along with collection of all clinical and radiographic outcomes. With RNA and protein analyses verifying the quality of the tissues obtained, we have successfully designed a tissue banking protocol for evaluations beyond histology and blood gas analysis.
Our study and the BACTRAC protocol have some limitations. This study requires someone to be available within 30 min to receive and process the samples. Several people are needed for a weekly rotation and backups in case the on-call individual is indisposed. Furthermore, our ability to enroll on weekends and nights is variable depending on staff. One concerning result was the low integrity of RNA from the thrombus itself. This is probably due to the small amount of RNA in the thrombus, along with the known presence of RNases. While this could hamper analysis of the thrombus itself, it does not negate evaluation of the proximal and distal blood. However, all blood samples contained very high to high-quality RNA. These samples will be used for future comparisons to determine genes expressed in the ischemic environment. The thrombi RNA will be used to examine gene expression on a qualitative level.
Conclusion
Understanding molecular and cellular changes intraluminally and within the thrombus in human acute ischemic stroke will provide vital information on the course of pathology in the clinical condition. We have created, for the first time, a step-by-step protocol for banking proximal artery blood, the thrombus, and distal intracranial arterial blood during MT. This approach will accelerate translational stroke research toward new methods of diagnosis, and innovative treatments. Moreover, these analyses of the tissues will permit us to translate results from the human patient to animal models to develop new therapeutic approaches based on the initial responses to the ischemic episode.
Supplementary file 1
Acknowledgments
We thank Tom Dolan for his outstanding medical illustration in figure 1B, and Mary Faulkner for her excellent service as the BACTRAC study coordinator.
References
Footnotes
Contributors JFF is the principal investigator for the BACTRAC tissue bank. Responsibilities included oversight and submission of regulatory documents, design of the tissue bank, collection of tissues, evaluation of data, and drafting of the manuscript. LAC is the administrator of the tissue bank; she catalogues the specimens and tracks their use in experiments. She also played a strong role in design of the banking protocol. AAG also played a strong role in the design of the banking protocol. She oversaw the training of new researchers on the protocol. SRM collected the clinical data, and designed the database for clinical/radiographic data collection and storage. KES, ALT, DNE, and SMD all played roles in consensus-design of the tissue bank. They collected and processed the samples included in the analysis. DEL designed the radiographic imaging data collection methods, and is the neuroradiologist who performs the assessments. AA and SG are neurointerventionalists who perform thrombectomy and collect tissues. JMR oversees the tissue collection training protocol, and assists with tissue collection. GJB and KRP played strong roles in the formation of the interdisciplinary collaboration. In addition, they design questions of the banked tissue, and perform analyses of the tissue for integrity and also for new markers/cytokines.
Funding Initial support for preliminary data was provided through an institutional grant from the University of Kentucky Department of Neurology.
Competing interests None declared.
Patient consent Not required.
Ethics approval University of Kentucky institutional review board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The authors will make the BACTRAC tissue bank collection protocol available upon request. These data are included in the manuscript, but the authors encourage collaboration with other laboratories. Please contact the corresponding author (JFF) for details.