Article Text

Abstract
Background Despite high recanalization rates achieved with endovascular treatment of acute ischemic strokes, around 50% of eligible patients will not achieve a good outcome. Parameters that may determine patient outcomes include: time from puncture to recanalization, the collateral status, the anesthesia regimen, blood pressure management, and distal emboli. Characterization of distal emboli generated during mechanical thrombectomy has been performed in previous studies.
Objective To further investigate the risk of distal embolization associated with microcatheter navigation across the clot.
Methods A contrast-enhanced clot analog was used in an in vitro model that mimicked a middle cerebral artery occlusion within a complete circle of Willis vascular replica. The clot was crossed with one of the following microcatheters: Pro18, XT-27 or 3MAX. The emboli generated during the procedure were collected and measured.
Results The use of Pro18 and XT-27 resulted in a significant reduction of visible particles (size ≥500 µm) as compared with the 3MAX catheter (P<0.003). For the size range between 8 and 200 µm, there was a trend for Pro18 to generate fewer particles (−18%) than XT-27 but without statistical significance (P>0.05). In comparison with previously published data, acquired under the same conditions, it was found that the clot crossing maneuver accounts approximately for 12% of the total number of small emboli (<200 µm) induced during a stent retriever-mediated mechanical thrombectomy procedure via a balloon guide catheter.
Conclusions The clot crossing maneuver has a significant effect on the total number of small particles induced during mechanical thrombectomy. Smaller microcatheter sizes should be favored when possible.
- catheter
- device
- stroke
Statistics from Altmetric.com
Introduction
The results of five randomized controlled trials showed that early endovascular thrombectomy in patients presenting with acute ischemic stroke caused by an occlusion of the proximal anterior circulation is related to improved functional outcome and reduced mortality as compared with standalone intravenous fibrinolysis.1 It is now accepted as a standard of care.2
Despite high recanalization rates achieved with endovascular treatment of acute ischemic strokes,3 4 more than 50% of eligible patients will not have a good outcome (modified Rankin Scale score 0–2).1 Parameters that may determine patient outcomes include: time from puncture to recanalization,5 6 the collateral status,7 the anesthesia regimen,8 9 blood pressure management,10 11 and the distal emboli burden.12 Characterization of distal emboli generated during mechanical thrombectomy (MT) has been performed in previous studies.13 14 We herein further investigated the risk of distal embolization associated with microcatheter navigation through the clot.
Methods
Creation of middle cerebral artery occlusion
Experiments were performed in a patient-specific circle of Willis 3D printed silicone model, which was connected to a circulation flow loop in preparation for simulation of cerebrovascular occlusion as described previously.13
Real-time flow distribution was monitored using flow sensors (Transonic Systems Inc, Ithaca, New York, USA). Pressure transducers (Validyne Engineering, Northridge, California, USA) recorded the internal carotid artery (ICA) and distal middle cerebral artery (MCA) pressures. The model was calibrated to maintain physiologically representative flow in each branch of the model.
From all our established cerebral emboli-mimicking clot models,15 we decided to use an inelastic clot model that is prone to fragmentation and has been frequently used in previous MT testing for distal emboli evaluation and has bulk mechanical properties similar to emboli retrieved from patients. It was generated by thrombin-induced clotting of bovine blood (2.5 NIHU thrombin/mL blood) with addition of barium sulfate (1 g/10 mL blood).
A segment of clot (4.3 mm in diameter and 6 mm in length) was introduced into the ICA and was carried up to the MCA bifurcation by the fluid flow.
Clot crossing maneuver
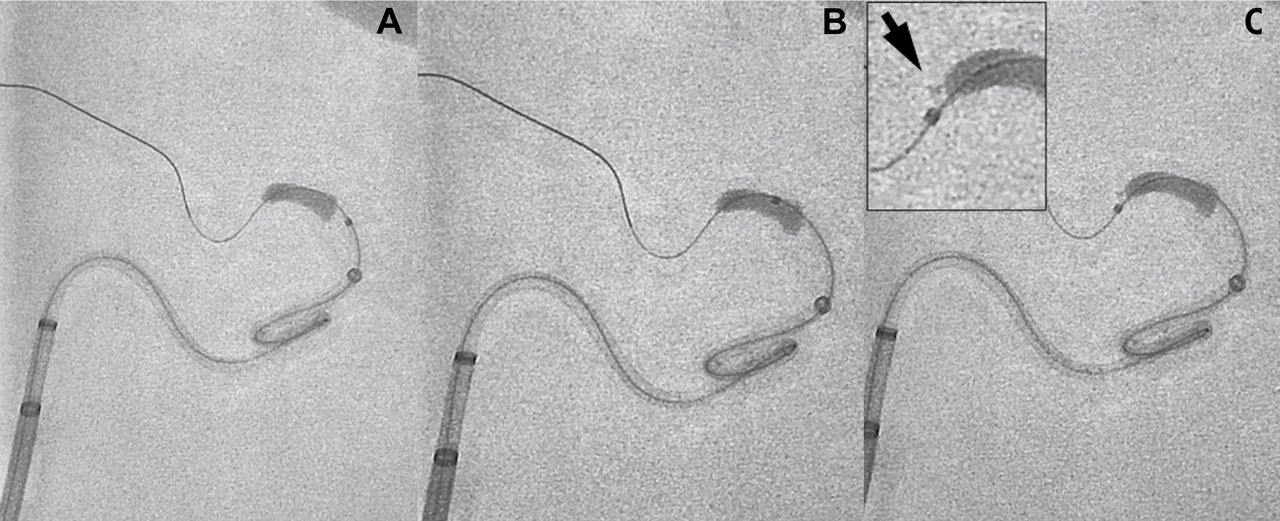
A Synchro-14 guidewire (Stryker Neurovascular, Fremont, California, USA) with a distal ‘J shape’ configuration was used to pass the clot. Then the clot was crossed with one of the following microcatheters with increasing distal outer diameter (OD) sizes: Trevo Pro18 (Stryker Neurovascular), distal OD=2.4F; Excelsior XT-27 (Stryker Neurovascular), distal OD=2.7F; or 3MAX (Penumbra, Alameda, California, USA), distal OD=3.8F. Nine replicates were used for each type of microcatheter (figure 1).

The microcatheter is advanced over the wire through the clot. The wire is then removed and the microcatheter is flushed with a slow infusion of 300 mL of saline to collect the distal emboli. The black arrow indicates a visible fragment generated by the clot-crossing maneuver.
Particle analysis
Once the microcatheter was navigated distal to the clot, it was connected to a power injector to collect the generated distal emboli. A very slow rate (0.5 mL/s) was used to obtain a total flush volume of 300 mL saline. The distal MCA was then clamped and all the system was manually flushed at higher rate to collect potential residual particles.
The emboli generated during the procedure of a size >500 µm were collected and measured with a caliper. The Coulter principle was used to characterize emboli with a size <500 µm.
Statistical analysis
Results were expressed as mean±SD. Data were analyzed using the Prism (GraphPad Software). A check was first made for normality of distribution. If normality was confirmed, then one-way analysis of variance was used. If the distributions were not normal, then a non-parametric Kruskal–Wallis test was used. Significance was concluded for a P value <0.05.
Results
Number and size of visible particles
The total numbers of particles ≥500 µm were 8 (median number per experiment 0, IQR 1), 8 (median number per experiment 1, IQR 1), and 21 (median number per experiment 3, IQR 1) for Pro18, XT-27, and 3MAX, respectively.
The use of Trevo Pro18 and Excelsior XT-27 resulted in a significant reduction of the total length of all visible particles (size ≥500 µm) collected during the nine replicates as compared with the 3MAX catheter (P=0.0029) (figure 2). The mean emboli lengths were 0.6±0.68 mm, 0.8±0.91 mm, and 2.4±1.52 mm for Pro18, XT-27, and 3MAX, respectively.

Total length of all visible particles (size >500 µm) collected during the nine replicates (*P<0.05). Color shading represents the total length of emboli in each replicate.
Fewer particles ≥1000 µm were noted with the use of the Pro18 and XT-27, as compared with the 3MAX catheter(P=0.0104) (figure 3).

Average number of emboli with size ≥1000 µm for the different catheters used to cross the clot.
Number of emboli with size between 200 and 500 µm
Few emboli were found in the range of 200–500 µm, and no significant differences were seen between the catheters studied. The average number of particles in this range was <1.5 in all groups.
Number of emboli with size <200 µm
For the size range of 8–200 µm, there was a trend for Pro18 to generate fewer particles (−18%) than XT-27, but the difference was not statistically significance (P>0.05) (figure 4).

Average number of emboli with size <200 µm for the different catheters used to cross the clot.
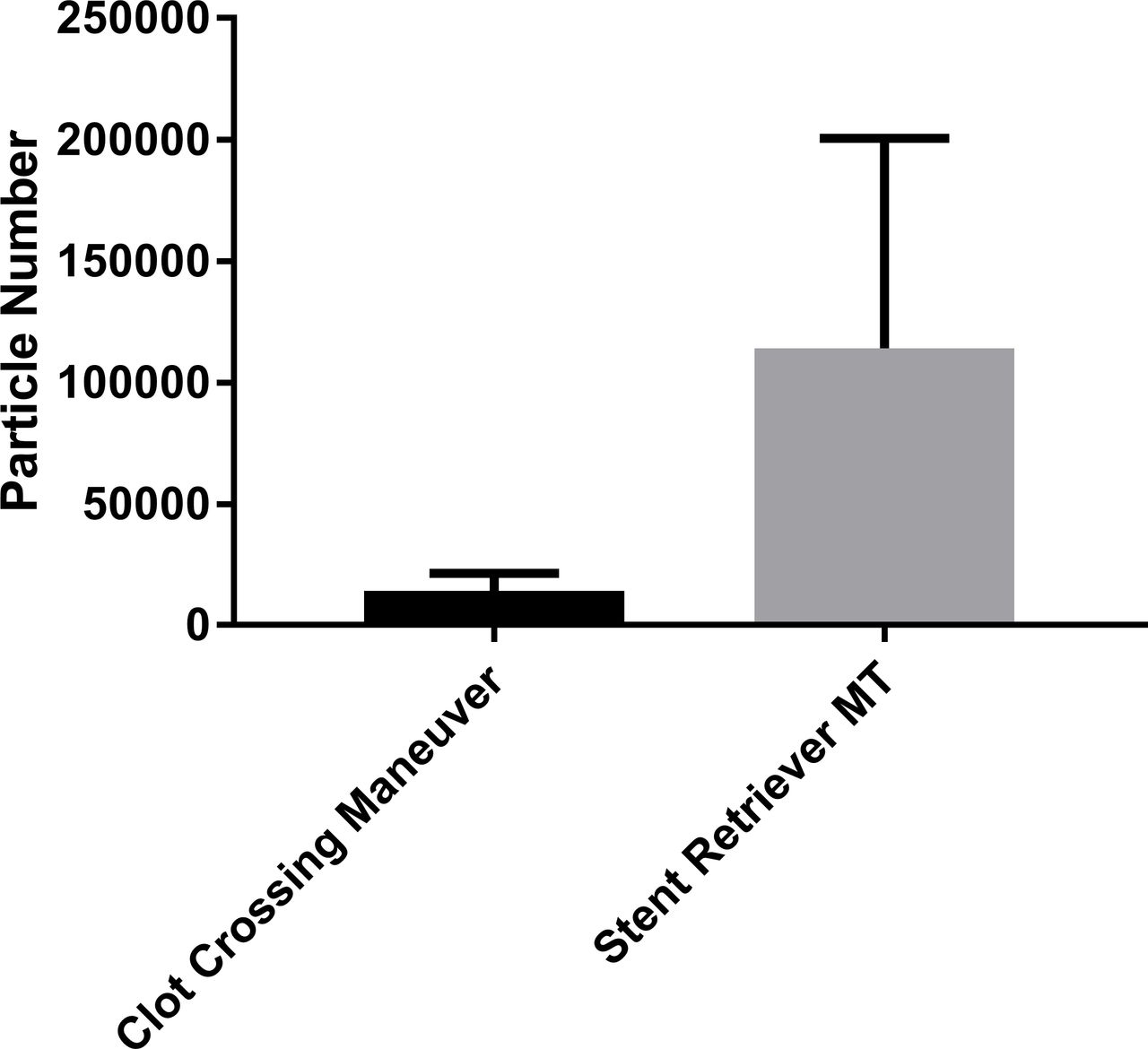
In comparison with previously published data acquired under similar conditions,16 it was found that the clot crossing maneuver accounted for approximately 12% of the total number of distal small emboli induced during stent retriever-mediated MT via a balloon guide catheter (figure 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Average number of emboli with size <200 µm from clot crossing versus historical data from stent retriever thrombectomy with proximal flow control.
Discussion
Thanks to recent technological developments and the results of multiple clinical trials, MT is becoming a mature technique with reports of high recanalization rates.3 To improve the 50% rate of good outcomes,1 research should also focus on procedure details, such as aiming to reduce the potential risk for distal emboli. In the literature, to the best of our knowledge, no data are available on the impact of the clot crossing maneuver, either in vitro or in vivo.
Stent retriever MT
Although significantly reduced with the use of the balloon guide catheter, the risk of distal embolization during MT with stent retrievers is not negligible.13 We have shown here that approximately 12% of the distal emboli burden is due to the clot-crossing maneuver (figure 4).
The smallest microcatheter size was associated with the least emboli. This finding is probably because the smaller catheter OD reduced the mechanical trauma to the embolus and also provided better deliverability.
The use of longer stent retrievers has proved to be an independent predictor of first pass reperfusion.17 The larger stent retriever size (6 mm) has been shown to present a better cohesion to the vessel wall and stability during retrieval.18 It requires the use of a 0.027 inch microcatheter. Although they have not been associated with better clinical or angiographic outcomes,19 longer stent retrievers are increasingly used, especially in proximal occlusions.
From our results the use of a 0.027 inch microcatheter should be restricted to the use of those 6 mm stents and not be used as a generic platform for multipurpose delivery. Although not recommended by the manufacturers, the 6 mm stents can generally be delivered through the smaller microcatheters at the cost of increased friction forces.
Direct aspiration
Clot removal via direct thrombus aspiration (a direct aspiration first pass technique (ADAPT)) is associated with an increased risk of distal embolization.16 Although not required, in some challenging anatomical conditions the operators would need extra support and would have to pass the clot with a catheter to deliver the aspiration catheter. In those situations, a 0.027 inch microcatheter would be mostly used.20 Some authors also recommend using a larger catheter, such as a 3MAX, to cross the clot.21From our study, we would recommend using only a microguidewire or a small microcatheter because we have shown that 3MAX catheter is associated with a high volume of emboli, especially in the largest sizes range.
However, the results of this study show that the no clot crossing maneuver would be an advantage of ADAPT. Further improvement in aspiration catheter design may allow improved navigation without crossing the clot and higher rates of complete clot ingestion, leading in the end to a significant decrease in distal embolizations.
Limitations
We acknowledge that our study has some limitations. First, the silicone vascular replica imperfectly reflects the flexibility of intracranial vessels and does not interact with the occlusive clot, which might alter the results.
We have shown previously that the stiffness and elasticity of thrombin-induced human embolus analogs are similar to those of cerebral thromboemboli retrieved from patients with acute ischemic stroke.15 We used here a single type of clot that may not reflect the wide range of clots encountered in clinical practice. However, from our characterization study we selected a clot that appears to be in the mid-range between a hard/elastic clot that would have probably induced fewer particles and a very soft clot prone to fragment that would probably have induced more emboli.
In order to put the results from this study into perspective with a complete MT procedure we used historical, published data. However, using the precise conditions and materials as previously reported, bias is minimized.
Finally, it is uncertain which emboli size range has the greater clinical impact but it is very likely that the distal emboli burden can impair patient neurological outcome after MT.12
Conclusions
The clot crossing maneuver has a significant effect on the total amount of small particles induced during MT. Smaller microcatheter sizes, or when possible removing the clot crossing maneuver altogether, should be favored. These experimental results require clinical validation.
References
Footnotes
Contributors JC: designed the study, designed and performed the experiments, analyzed and interpreted the data, drafted the manuscript, approved the final manuscript and agrees to be accountable for the accuracy and integrity of the work. RMK, MJG, J-YC: designed the study, designed and performed the experiments, analyzed and interpreted the data, revised the manuscript, approved the final manuscript and agree to be accountable for the accuracy and integrity of the work. RA, MM, ETL: designed and performed the experiments, analyzed and interpreted the data, revised the manuscript, approved the final manuscript and agree to be accountable for the accuracy and integrity of the work.
Funding Partially supported by research grants from the Fulbright Program, the Philippe Foundation, and the French society of Radiology (Bourse de Recherche SFR-CERF).
Competing interests JC has received educational grant from Microvention/Terumo and Medtronic. MM, J-YC: fee-for-service consulting for Stryker Neurovascular, ETL: fee-for-service consulting for Imperative Care, InNeuroCo, Route 92 Medical, StrykerNeurovascular. MJG: as been a consultant on a fee-per-hour basis for Cerenovus, Imperative Care, InNeuroCo, Medtronic Neurovascular, Phenox, Route 92 Medical, Stryker Neurovascular; holds stock in InNeuroCo, Imperative Care and Neurogami; and has received research support from the National Institutes of Health (NIH), Anaconda, Cerenovus, Cook Medical, Gentuity, Imperative Care, InNeuroCo, Magneto, Microvention, Medtronic Neurovascular, MIVI Neurosciences, Neuravi, Neurogami, Philips Healthcare, Rapid Medical, Route 92M, Stryker Neurovascular, and the Wyss Institute.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Raw data will be available upon request to the corresponding author.