Article Text

Abstract
Purpose Several different training environments for practicing neurointerventional procedures have been realized in silico, in vitro, and in vivo. We seek to replace animal-based training with suitable alternatives. In an effort to determine present training model distribution and preferences, we interviewed interventional neuroradiologists from 25 different countries about their experience in distinct training environments.
Methods A voluntary online survey comprising 24 questions concerning the different training facilities was designed and electronically conducted with the members of the European Society for Minimally Invasive Neurological Therapy.
Results Seventy-one physicians with an average experience of 11.8 (±8.7) years completed the survey. The majority of participants had experience with animal-based training (eg, stroke intervention: 36; 50.7%). Overall, animal-based training was rated as the most suitable environment to practice coil embolization (20 (±6)), flow diverter placement (13 (±7)), and stroke intervention (13.5 (±9)). In-vitro training before using a new device in patients was supported by most participants (35; 49.3%). Additionally, preference for certain training models was related to the years of experience.
Conclusion This survey discloses the preferred training modalities in European neurointerventional centers with the majority of physicians supporting the general concept of in-vitro training, concomitantly lacking a standardized curriculum for educating neurointerventional physicians. Most suitable training modalities appeared to be dependent on procedure and experience. As animal-based training is still common, alternate artificial environments meeting these demands must be further developed.
- aneurysm
- angiography
- intervention
- standards
Statistics from Altmetric.com
Introduction
Neuroendovascular treatment rapidly increased over the past few years and has become a favorable well-established treatment technique, particularly for intracranial aneurysms and acute ischemic stroke.1–4 Despite a continuous refinement of available techniques and materials, intraprocedural complications such as arterial perforation and thrombembolic events still remain an issue.5–7 New devices and methods aiming at treating complex aneurysms, reducing adverse events, and improving long-term aneurysm occlusion are constantly emerging, many of which may carry a device-specific learning curve in order to be used safely.8–11 Hence, there is the need for a realistic training environment with the possibility of practicing different procedures and improving neurointerventional skills. Available training setups include computer-based simulations, in vitro training using generalized or patient-specific vascular models, and animal-based training, such as in rabbits or dogs with artificially created aneurysms.9 11–14 Therefore, the use of animal models is still a typical preclinical training opportunity to anticipate difficult clinical conditions.11–14 Due to ethical concerns we seek to replace animal-based training by improving alternative training environments.15
Any such effort must adhere to the needs of the physician community involved in training neurointerventional procedures. We therefore surveyed neurointerventionalists from 25 different countries applying an online survey to assess the current status of training environments in neurointerventional practice.
Materials and methods
No institutional review board approval was required for this survey. A 24-question online survey was compiled using the Lime Survey tool to assess the current status of neurointerventional training environments in European Neuroradiological interventional centers. Questionnaires were addressed to members of the European Society of Minimally Invasive Neurological Therapy (ESMINT), including 344 members in good standing at that time. The survey link was distributed via email. All questions were compulsory contributions and answers were saved anonymously. The Lime Survey identifies the IP address of the participants, limiting respondents to a single response. The study period took 4 weeks from August 2017 to September 2017. Questions are shown in online supplementary table 1–5. Broadly, we assessed the current use of different training modalities and the participants’ perspective on the suitability of the different environments for training specific procedures.
Supplemental material
Statistical analysis
Questionnaire answers were evaluated with standard descriptive statistics (Microsoft Excel for Mac V.15.32 2017, Redmond, WA, USA). Values for years of experience were dichotomized to allow stratified analysis of the ratings for animal laboratory training according to the level of the participant’s experience.
Results
Out of 344 queried members of the ESMINT, a total of 71 survey responses were included. Due to various missing responses, the total response rates for several questions were below 100%. From all participants who named their country (43; 68.3%), the majority of respondents were from Germany (7; 16.3%), Italy (6; 14.0%), Sweden, and France (each 4; 9.3%). Overall, the following countries participated in our survey: Germany, Italy, Sweden, France, United Kingdom, Denmark, Turkey, Australia, Brazil, Ireland, the Netherlands, Croatia, Hungary, Romania, Norway, Portugal, Switzerland, Serbia, Spain, Finland, Poland, India, Jordan, Latvia, and Belarus. Participants reported a mean neurointerventional experience as first operator of 11.8 years (±8.7, range: 0–35 years).
Utilization of different training environments (survey questions 2–5)
Physicians were questioned about their experience in performing different neurointerventional procedures and training in distinct training modalities (questions 2–5, online supplementary table 1). Participants had significant neurointerventional experience (online supplementary figure 1A), with sizeable majorities reporting having performed each >50 of the questioned procedures clinically (DSA: 57; 80.3%, stenting of the cervical carotid artery: 35; 49.3%, coil embolization: 44; 62%, flow diverter placement: 17; 23.9%, embolization of vascular malformations: 29; 40.8%, and acute endovascular stroke intervention: 37; 52.1%).
Supplemental material
A significant number of participants reported prior experience with different training modalities (online supplementary figure 1B). Across all training modalities, the most commonly trained procedures were coil embolization in an angiography simulator and a vascular flow model (each 66.2%) and flow diverter placement deploying a vascular flow model (60.1%). Overall, a significant number of participants reported participation in some kind of animal laboratory training (ranging from n=13; 18.3% to n=37; 52.1% across the different procedures, online supplementary figure 1B).
Supplemental material
Role of training in practice (survey questions 6–14)
Participants were asked about training and teaching themselves or other neurointerventionalists in different training environments (angiography simulator, vascular flow model, animal laboratory training). Among those respondents reporting regular training (at least once every 1–2 years), all three different training environments appeared to be roughly similarly prevalent (angiography simulator: 11; 15.5%, vascular flow model: 18; 25.4%, animal-based training: 13; 18.3%). Eight (11.3%) out of all physicians never performed training applying any of the three modalities.
Large majorities support or strongly support in-vitro training applying a new device prior to using it in a patient (44; 61.9%) and the general concept of in-vitro training for less experienced operators is to become a mandatory part of specialty training (41; 57.7%).
The concept of ‘observation and gradual performance of tasks’ as the prevalent concept to learn neuroangiographic techniques was identified by the vast majority of respondents (53; 74.6%), whereas only minorities reported structured training using a simulator (8; 11.3%), vascular models (6; 8.5%), or animal laboratory (10; 14.1%). No mandatory non-clinical training programs were reported before performing procedures in patients for the first time by most of the interventionalists (45; 63.4%). Very few respondents from Germany, Italy, Latvia, the Netherlands, Poland, Portugal, and Spain reported mandatory non-clinical training prior to performance of real endovascular procedures (simulator: 4; 5.6%, vascular model: 5; 7.0% and animal laboratory: 4; 5.6%).
Practicing different procedures in distinct training environments (survey questions 15–21)
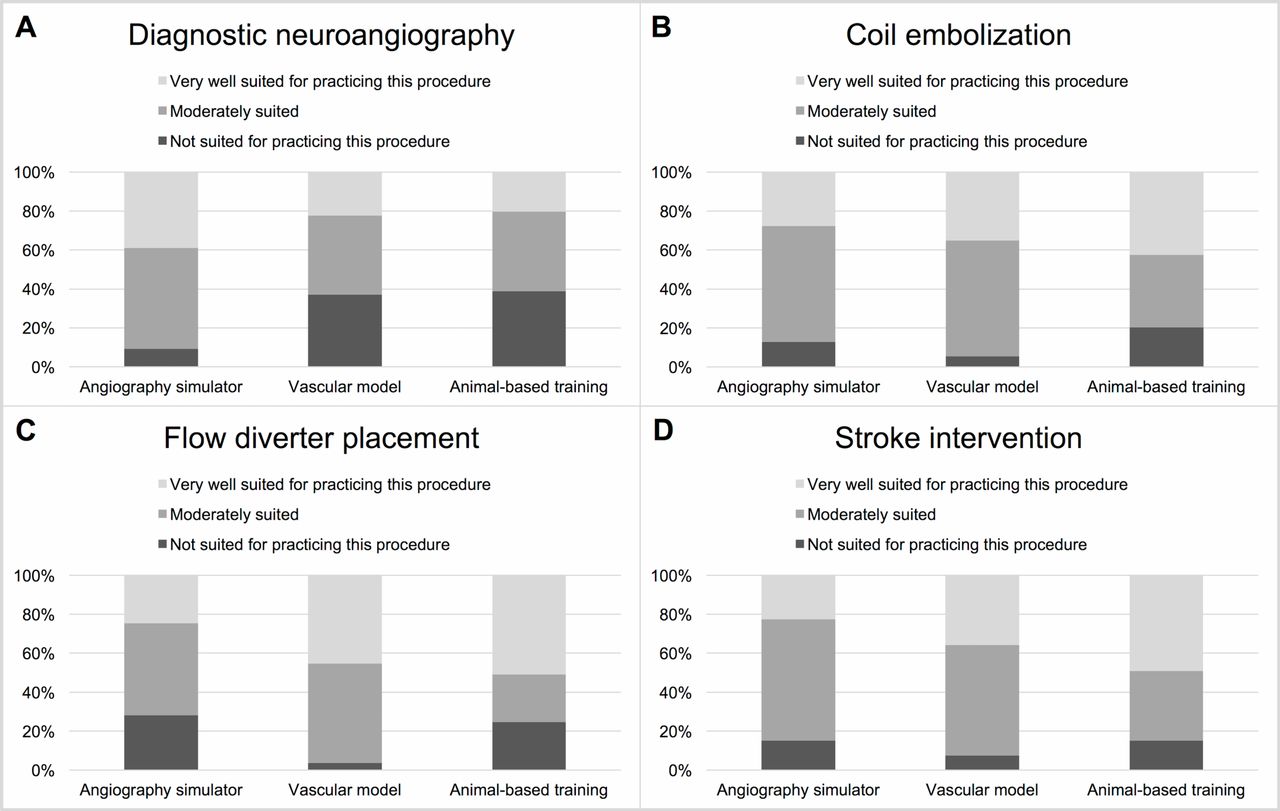
Figure 1 displays results for the suitability of different training environments for learning and practicing distinct neurointerventional procedures as reported by the respondents. To practice diagnostic neuroangiography, the angiography simulator was more frequently rated as moderately and very well suited than other training environments. In contrast, for practicing coil embolization, flow diverter placement and stroke intervention, both vascular models and animal laboratory training were rated as at least equally- or better-suited compared with simulator-based training.
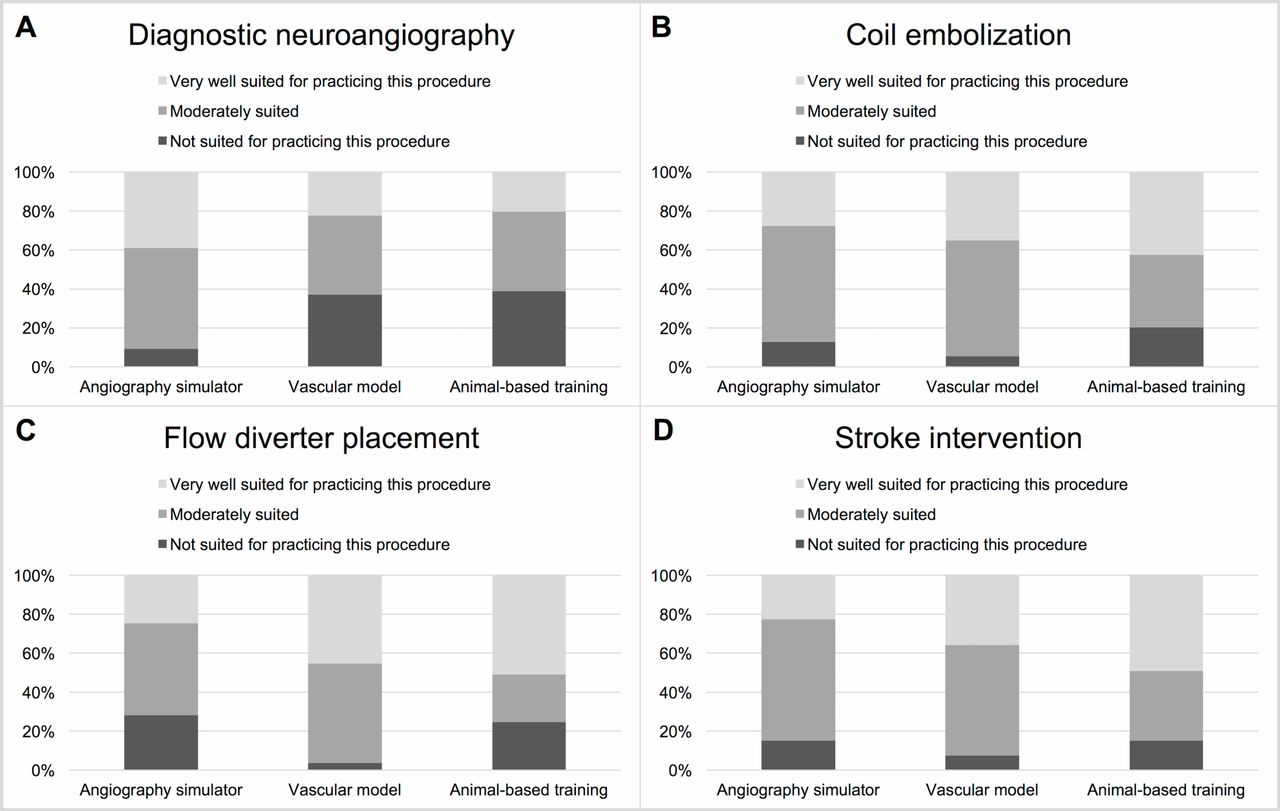
Suitability of different training environments for learning and practicing different neurointerventional procedures. (A) Angiography simulators were mainly rated as very well-suited for learning diagnostic neuroangiography. (B–D) Vascular models and animal-based training were comparably rated as better-suited to learn more complex interventions.
A subset of questions asked participants to rate the distinct training environments regarding their suitability for different levels of trainee experience. In general, participants ascribed limited suitability of simulator-based training for more experienced physicians, while vascular model and animal-based training were more uniformly rated as suitable for different levels of physician experience (figure 2).

Eligibility of distinct training environments to learn neurointerventional procedures according to the physicians’ experience. (A) The majority of participants rated all three modalities as mainly moderately-suited for beginners to learn any intervention. (B) For physicians with 1–2 years of experience animal-based training was rated as best-suited to learn any intervention. (C) For physicians with more than 2 years of experience, angiography simulators were evaluated as moderately- or not well-suited for practicing neurointerventional procedures.
Respondents’ experience and view of animal laboratory training
Stratified analysis of responses according to the respondents’ level of experience (dichotomized according to reported years of experience) revealed different opinions regarding the suitability of animal-based training (figure 3). Across all questioned procedures, physicians who were less experienced ascribed higher ratings of suitability to animal-based training than the more experienced half of the study population.

Reported suitability of animal-based training dichotomized by participant’s experience. (A–D) Across all procedures, the less experienced participants gave higher ratings of suitability for animal-based training.
Respondents assessment of distinct artificial training environments depending on prior training experience
We identified the correlation between participants’ assessment of distinct training modalities (angiography simulator, vascular flow model, and animal-based training) in consideration of prior training experience in performing diagnostic neuroangiography, coil embolization, flow diverter placement, and stroke intervention in an angiography simulator, vascular flow model, or in animal-based training, respectively. The majority of experienced respondents rated angiography simulators and vascular flow models as moderately- (angiography simulator 15; 46.9%; vascular flow model 11; 55%) or very well-suited (angiography simulator 10; 31.3%; vascular flow model 8; 40%). Considering animal-based training, opinions varied, as physicians without any prior training experience rated animal-laboratory training equally as not-suited (12; 37.5%) and very well-suited (14; 43.8%).
European countries offering educational neurointerventional hands-on training
Completing the online questionnaire, participants were asked to name their country and the corresponding number of centers offering hands-on training courses (academic neurointerventional centers, training centers owned by the state and company-owned training centers). Although a good response rate was received, we subsequently acquired missing data from remaining European countries by distributing specific e-mails addressed to leading European neurointerventional hospitals, therefore achieving a higher reliability. Countries providing insufficient information due to incomplete answers are marked accordingly.
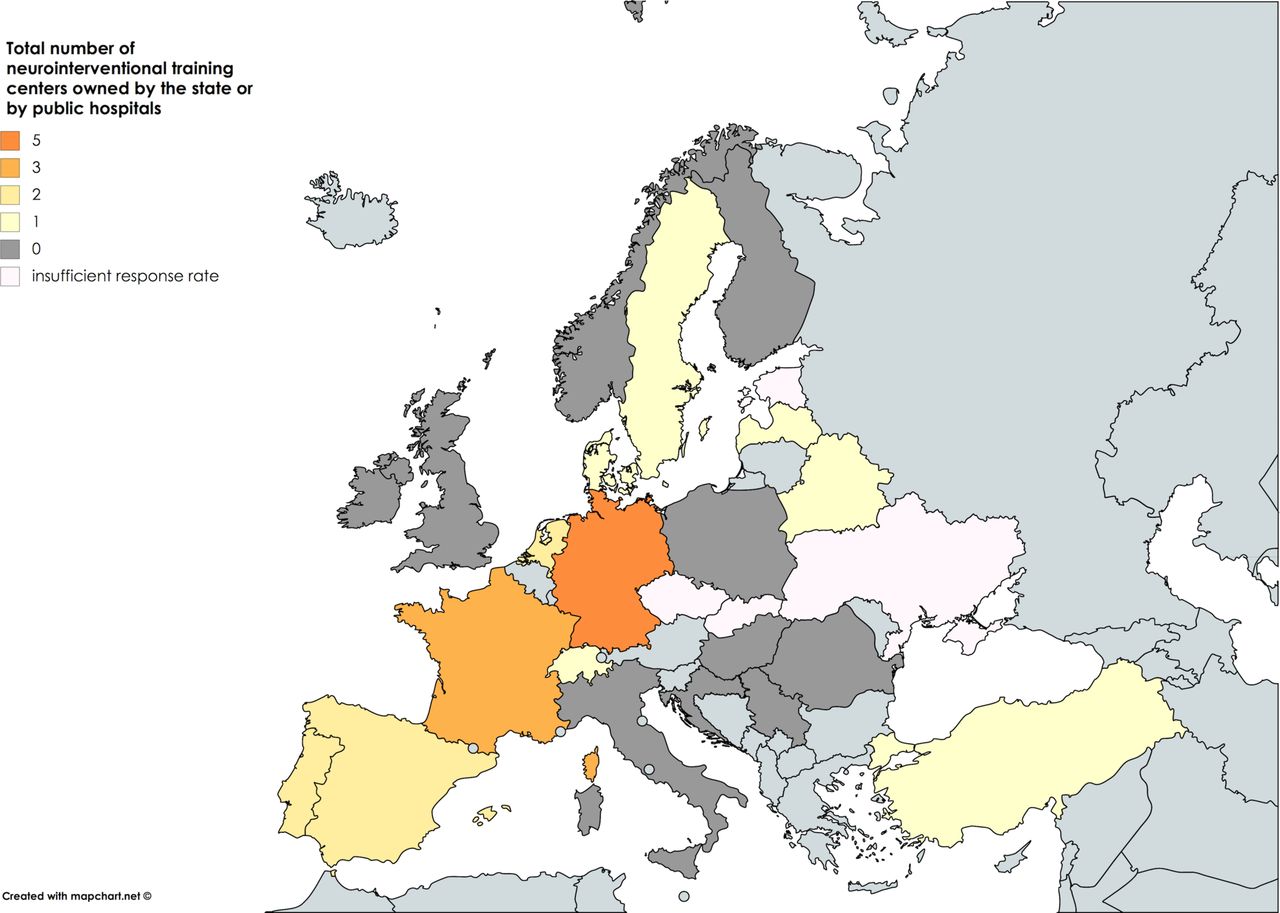
European comparison regarding neurointerventional training centers owned by the state or by public hospitals showed the highest total numbers in Germany (n=5) and France (n=3, see figure 5). The largest number of academic neurointerventional centers was also registered in Germany (n=25) and France (n=34, see online supplementary figure 2). Company-owned training centers were of minor importance with most centers available in Turkey (n=2, see online supplementary figure 3). Relative numbers of training centers per one million inhabitants were calculated by using the population count of The World Factbook 2017, Washington, DC, Central Intelligence Agency, 2017. Most academic neurointerventional centers referring to the population level were reported in Estonia (0.77), followed by Denmark (0.54), Latvia (0.53), and France (0.51). Distribution of state-owned/public hospital-owned and company-owned training centers showed an even spread at a lower level. Corresponding results are illustrated in online supplementary figure 4–6.
Supplemental material
Supplemental material

Valuation of three training modalities dependent on prior experience in practicing distinct neurointerventional procedures. (A, B) Angiography simulators and vascular flow models were rated as moderately- or very well-suited for practicing the above-mentioned procedures. (C) Rating of animal-based training for practicing distinct neurointerventional procedures showed major heterogeneities.
![[SP1.jpg]](https://jnis.bmj.com/content/neurintsurg/11/3/283/DC2/embed/inline-supplementary-material-2.jpg?download=true){kind=link}
![[SP2.jpg]](https://jnis.bmj.com/content/neurintsurg/11/3/283/DC3/embed/inline-supplementary-material-3.jpg?download=true){kind=link}
{kind=link}
{kind=link}
{kind=link}
![[SP3.jpg]](https://jnis.bmj.com/content/neurintsurg/11/3/283/DC4/embed/inline-supplementary-material-4.jpg?download=true){kind=link}
![[SP4.jpg]](https://jnis.bmj.com/content/neurintsurg/11/3/283/DC5/embed/inline-supplementary-material-5.jpg?download=true){kind=link}
{kind=link}
{kind=link}
Colored European map showing distribution of training centers owned by the state or by public hospitals offering hands-on training courses throughout Europe.
Discussion
The survey was performed with the intention of disclosing the current status of neurointerventional training models particularly in regard to the incidence of animal models applied and training environments preferred. To our knowledge, this survey is the first to report the experience in different neurointerventional training environments in European countries. Including answers of 71 neurointerventional participants from 25 different countries, it can be considered as representative of European neurointerventional practice.
In neurointerventional practice, training environments are important in facilitating the safe use of existing and new devices, particularly with regard to intraprocedural complications.3 4 8 10 Therefore, a structured neurointerventional education with the possibility of hands-on training in artificial surroundings is necessary. For learning diagnostic angiography as a beginner, participants of our survey most favorably rated angiography simulators (figure 1A). To learn more complex interventional procedures such as coil embolization of cerebral aneurysms, implantation of a flow diverter, and acute endovascular stroke intervention (figure 1B-D) both animal-based training and the use of vascular models or angiography simulators were more commonly rated as suitable applications. In our opinion, one of the reasons why simulators were rated as less suitable for more complex procedures may be the lack of direct, ‘true’ tactile feedback. This type of tactile feedback can be experienced in vascular models and animal-based training, and certainly contributes significantly to the learning curve associated with procedures such as flow diverter implantation, which require intimate control over the movement of the pusher wire and associated catheters to allow adequate device positioning. Therefore, further refinement of vascular models should be focused on improving the reproduction of these more complex interventions, which would both address the need for an adequate training environment reflected by our study’s respondents as well as increase the likelihood of actually replacing animal experiments. Interestingly, in addition to their suitability for less complex interventions, angiographic simulators were also rated as particularly suitable for training lesser-experienced physicians. These findings may be helpful, e.g. for designing a tiered-stage training curriculum incorporating both simulators and vascular models.
Our survey confirms that in several European countries, animal-based training is still quite frequently utilized for teaching neurointerventional procedures and is generally regarded as suitable, particularly for training more complex interventional procedures (see also figure 1). Coil embolization and acute endovascular stroke intervention were the most commonly practiced procedures, both being associated with relatively high reported frequencies of animal based-training. These procedures therefore qualify as particularly valuable targets for the development of improved vascular models when aiming to reduce animal experiments. Physicians with expertise in using animal-laboratory training rated this type of training modality as suitable for beginners to learn distinct neurointerventional procedures, whereas respondents without experience working on animal models heterogeneously assessed its eligibility (see figure 4). Remarkably, a majority of participants rated animal-based training as moderately- or even very well-suited for beginners, without these participants themselves being experienced in the use of animal-laboratory training. Although the reasons for the aforementioned heterogeneities remain unknown, these results can be interpreted as a general need for a more standardized neurointerventional training curriculum and the principal support for the use (and therefore the development) of vascular models offering an adequate training environment resembling human structures, which may offer an ethically preferable alternative to animal experiments.
The results of our survey furthermore show that the participants’ level of experience seems to affect the preferred training environment. Animal-based training was rated preferably to learn and improve operator skills by less experienced respondents, whereas the more experienced physicians evaluated animal-based training as less suitable (see figure 3). This relationship may point at the shortcomings of animal-based training. Animal models include constant bloodflow with its typical hemodynamic forces and representative haptics of the vessel walls as well as the possibility for thrombosis and vasospasm.14 Participants might appreciate the awareness of operating on a living creature, generating a more realistic setting. However, animal models are poorly predictive regarding clinical complications16 and carry inherent limitations such as the non-human anatomy (which often poorly reflects the disease process being simulated, particularly for coil embolization) or unrealistic device behavior, such as the strong microcatheter pulsation often observed in the rabbit elastase aneurysm model.9 10 14–17 An alternate interventional training method using silicone models based on 3D printing technology might be a feasible approach to overcome some of the important limitations of animal-based training and has been shown to be a crucial part of the education for neuroradiologists so far.9 17 3D printing of vascular structures offers the possibility of testing endovascular devices in different patient-specific conditions, ranging from simple straight vessel anatomy over severe curvature or stenoses to the multitude of different real aneurysm morphologies. From an educational standpoint, the ability to theoretically rehearse a challenging case based on DSA and video recordings and afterwards perform training in an anatomically identical vessel model, is unique to this training environment and certainly exciting.
Our results might indicate that the shortcomings of animal-based training are more evident to more experienced physicians. The future improvement of vascular training models should therefore aim at overcoming some of these limitations of animal-based training while trying to increase acceptance, particularly among lesser-experienced physicians.
As our survey reveals some disparities regarding training modalities and preferences, it points out the central issue of lacking a standardized neurointerventional curriculum in Europe at once. The general concept of neurointerventional in-vitro training to test new devices prior to clinical use and to teach neuroangiographic skills as a part of specialty and subspecialty training was strongly supported by the majority of our respondents, although hardly any queried training programs (angiography simulators, vascular models, or animal training) were rated as mandatory before performing interventional procedures in patients for the first time. Most of the physicians are trained by observing and gradually performing tasks independently before performing diagnostic and interventional procedures in patients. Furthermore, European comparison relating to the different neurointerventional types of training centers offering educational hands-on courses revealed wide imbalances (see also figure 5). Neurointerventional education seems to be well-developed in central Europe, showing the highest total numbers of academic centers and offering a sufficient number of hands-on courses per million inhabitants at the same time. However, it must be conceded that not all neurointerventions are done and therefore trained in academic hospitals and that health structures differ between countries. Comparing the regional distribution of state-owned and company-owned educational centers considerable homogeneities with overall insufficient numbers of training centers could be observed, indicating the high demand for widening these educational structures. The critical issue of major worldwide differences regarding the organization of neurointerventional training was reported earlier.18 19 Hence a structured approach for different neurointerventional training concepts is needed, aiming to improve operators’ technical skills. European differences must be overcome to provide a thriving education for all neurointerventionalists independent of their origin. Apart from providing the required theoretical background, an adequate educational curriculum should include skill-based training in a dedicated training environment. Performing a fixed number of procedures in a training environment or passing certain skill-based assessments might be considered before working with patients and simultaneous observation of real interventions in the angiosuite should be guaranteed. There is the need for future research to determine which training environment is most-suited, but we believe that a combination of angiography simulators and vascular models can be utilized to design a well-rounded training curriculum and would support this approach from an ethical point of view. In our opinion, and supported by the survey results, angiography simulators might be most useful for learning and practicing the basic steps of angiography and interventional procedures. Subsequently, vascular flow models are necessary to offer a higher degree of realism in terms of catheter and device haptics, and detailed vascular anatomy. Several opportunities for resident training in surgery comprising vascular surgery simulation laboratories are already in use, successfully showing that simulator training can increase practical skills.20–22 The endorsement of simulation to augment practical training and the benefit of developing a standardized simulation curriculum was already reported earlier by Duran et al who surveyed 183 surgical trainees about the educational value in simulation training.22 We therefore conclude that not only the reduction of animals applied in interventional training settings, but moreover a standardized educational curriculum, is appropriate to train neurointerventionalists.
The survey had several limitations. As the ESMINT served 344 members in good standing at the time of distributing the survey link, the response rate was only moderate (21%). Although it cannot be guaranteed that all replies were from actual ESMINT members, all participants confirmed to work as practicing neurointerventionalists. Near-complete or incomplete datasets were relatively frequent (n=21). We didn’t ask for the average number of performed neurointerventions per year, which might have shown an association with the individual opinion on training opportunities. Additionally, we did not assess the participant’s formal background in terms of medical specialty or subspecialty training. As our data was only acquired from European centers it cannot be directly applied to other countries.
Conclusions
Our survey reveals detailed information about the current status of training environments in European neurointerventional practice, including the frequency of animal-based training. Despite the lack of a standardized European curriculum for educating neurointerventional physicians, animal models appear to be widely used for teaching neuroendovascular procedures. They seem to be favored among less experienced physicians and for the training of more complex procedures. Based on this knowledge, alternate training modalities should be developed to reduce the need to sacrifice animals for neurointerventional training.
Supplemental material
![[SP5.jpg]](https://jnis.bmj.com/content/neurintsurg/11/3/283/DC6/embed/inline-supplementary-material-6.jpg?download=true){kind=link}
Supplemental material
![[SP6.jpg]](https://jnis.bmj.com/content/neurintsurg/11/3/283/DC7/embed/inline-supplementary-material-7.jpg?download=true){kind=link}
Supplemental material
![[SP7.jpg]](https://jnis.bmj.com/content/neurintsurg/11/3/283/DC8/embed/inline-supplementary-material-8.jpg?download=true){kind=link}
References
Footnotes
Contributors Conception/design of work – AMF, J-HB. Data collection – AMF, JS. Data analysis and interpretation – J-HB, AMF, JF. Drafting the article – AMF. Critical revision of the article – JS, J-HB, AMF, JF. Final approval of the version to be published – J-HB, AMF, JF. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved – JS, J-HB, AMF, JF.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.