Article Text

Abstract
Background Woven Endobridge (WEB) embolization is a safe and efficient technique for endovascular treatment of intracranial aneurysms. However, the management of aneurysm recurrence after WEB placement has not been well described to date. We present our multicenter experience of endovascular retreatment of aneurysm recurrence after WEB implantation.
Methods This is a multicenter study of patients who underwent endovascular retreatment after WEB implantation in three German tertiary care centers. Treatment strategies, complications, and angiographic outcome were retrospectively assessed.
Results Among 122 aneurysms treated with the WEB device, 15 were retreated. Of these, six were initially treated with the WEB only, two were pretreated by coiling, and seven large aneurysms were treated in a multimodality approach. Ten were true aneurysm remnants and five were neck remnants. The reasons for retreatment were WEB migration (n=6), initial incomplete occlusion (n=5), and WEB compression (n=4). Retreatment strategies included coiling (n=4), stent-assisted coiling (n=7), flow diversion (n=3), and placement of an additional WEB (n=1). All procedures were technically successful and there were no procedure-related complications. Among 11 patients available for follow-up after retreatment, three were retreated again. At last angiographic follow-up, available in 11/15 cases at a median of 23 months, complete occlusion was obtained in eight cases and neck remnants in three.
Conclusions This pilot study shows that endovascular retreatment of recurrent or residual aneurysms after WEB implantation can be done safely and can achieve adequate occlusion rates.
- aneurysm
- coil
- device
Statistics from Altmetric.com
Introduction
The Woven Endobridge (WEB; Sequent Medical, Aliso Viejo, California, USA) was introduced in 2011 for the treatment of wide-necked and bifurcation aneurysms, which are typically challenging to treat by endovascular means. The WEB is an intra-aneurysmal flow disruptor which is placed within the aneurysm cavity and leaves the parent artery unaffected.1 It potentially provides immediate exclusion of the aneurysm and does not require long-term antiplatelet therapy imperatively. Therefore, the WEB can be used for both unruptured and ruptured aneurysms.2 3
The safety and efficacy of the WEB for the treatment of complex aneurysms has been evaluated in several multicenter studies.3 4 Mid-term adequate occlusion rates in GCP trials have been shown to exceed that of coiling or stent and coil in similar subsets of aneurysms.3 4 However, aneurysm recurrence may occur and a subset of these recurrent aneurysms might require retreatment. The management of residual aneurysms after WEB implantation is potentially different from that resulting from coil compaction or after flow diverter use. It may thus be challenging, because retreatment options have not been well defined and the long-term angiographic outcome after retreatment remains uncertain.5
The objective of this study was to present our multicenter experience with retreatment of recurrent and residual aneurysms after previous WEB implantation. We aimed to assess the safety and feasibility of retreatment and to report on angiographic results.
Methods
We retrospectively evaluated all consecutive patients who underwent successful WEB implantation at three German high volume neurovascular centers between May 2011 and February 2018. All patients who underwent endovascular retreatment of recurrent or residual aneurysms after initial WEB implantation were identified and included. Portions of the data of six included patients were reported in an article that focuses on primary WEB implantation as part of a multimodality treatment in complex, large, and partially thrombosed aneurysms.6 According to the institutional guidelines, no ethics committee approval was required for this retrospective study.
Data collection
The following data were obtained from the medical records: patient age, sex, aneurysm rupture status, aneurysm location, initial WEB treatment (date, WEB type, use of additional devices), anti-aggregation treatment, and retreatment strategy (number, date, treatment method).
Baseline aneurysm characteristics were evaluated by conventional four-vessel digital subtraction angiography (DSA) with three-dimensional reconstructions. Aneurysm width, height, neck width and dome-to-neck (D/N) ratio and presence of intrasaccular aneurysm thrombosis were determined for all aneurysms. An aneurysm was considered as wide-necked if the neck width was larger than 4 mm and/or the D/N ratio was up to 2.
Initial WEB treatment
At our institutions the WEB was predominantly used for complex, wide-necked, and bifurcation aneurysms with an unfavourable configuration for conventional coiling, which would otherwise have required stent-assisted approaches or surgery.
All procedures were performed via a transfemoral approach with the patient under general anesthesia in a biplane angiosuite (Philips, Best, the Netherlands and Siemens, Erlangen, Germany). In the majority of the cases the WEB was delivered through a dedicated VIA microcatheter (Sequent Medical, Aliso Viejo, California, USA). WEBs with diameters 4–7 mm were delivered through a 0.021 inch internal microcatheter (VIA 21), WEBs 8–9 mm through a 0.027 inch (VIA 27) microcatheter and WEBs 10–11 mm through a 0.033 inch microcatheter (VIA 33).
In this study, single-layer (SL), double-layer (DL), and single-layer sphere (SLS) WEBs were used. The appropriate WEB size was selected according to the aneurysm width and height as measured on two-dimensional DSA images. Implant sizes were chosen to be slightly larger than the aneurysm equator diameter as recommended in the Instructions for Use (IFUs). However, in seven cases the aneurysm size exceeded the largest available WEB. These aneurysms were treated in a multimodality approach and the WEB was used in combination with a stent, coils or a flow diverter.
Angiographic control and retreatment
Our institutional follow-up protocols consisted of angiographic control 6 and 24 months after the procedure using DSA, magnetic resonance angiography (MRA), or CT angiography (CTA).
The Raymond–Roy occlusion classification (RROC) was used to evaluate the extent of aneurysm occlusion immediately at the end of the procedure and at follow-up imaging (1, complete occlusion; 2, neck remnant; 3, aneurysm remnant). Complete occlusion and neck remnants were defined as adequate occlusion. In case of incomplete aneurysm occlusion, the indication for retreatment was made individually after discussion within an interdisciplinary neurovascular team between neuroradiologists and vascular neurosurgeons. Neck remnants were subjected to retreatment if a relevant risk of rupture due to large size and/or complex shape of the aneurysm was estimated and if retreatment was expected to be associated with low morbidity.
The endovascular retreatment method was left to the discretion of the operator. Retreatment was considered successful if complete cessation of contrast opacification of the aneurysm sac could be achieved.
All procedure-related complications (eg, ischemic and hemorrhagic events) that occurred during aneurysm treatment and during follow-up were recorded. We report both symptomatic and asymptomatic complications. Functional outcome was evaluated by the modified Rankin scale (mRS) at discharge from hospital and at follow-up visits. Treatment-related morbidity was defined as any increase in the mRS score after the procedure.
Anti-aggregation therapy
A bolus of heparin (5000 IU) was administered after groin puncture, followed by aliquots of 1000 IU/hour. Heparin was discontinued at the end of the procedure. For WEB implantation, all patients received acetylsalicylic acid (ASA) 100 mg/day starting 5–7 days before the procedure and ASA monotherapy was continued for a minimum of 4 weeks. In case of additional stent implantation or flow diversion, a daily dual antiplatelet regimen with ASA 100 mg and clopidogrel was administered for at least 4 months post intervention, starting 5–7 days before the procedure. Thereafter, ASA monotherapy was continued. Platelet inhibition was tested in all patients with ASA and accessorily P2Y12 assays where required (VerifyNow, Accumetric, San Diego, California, USA). A platelet inhibition level of 350–550 aspirin response units (ARU) and 30–90% for clopidogrel was required. An insufficient response to either drug was counteracted by dose escalation (eg, clopidogrel 150 mg/day) or substitution with prasugrel (60 mg bolus, 10 mg/day).
Statistical analysis
Descriptive statistics were used. Categorical variables are presented as numbers and percentages. Continuous variables are presented as median and range.
Results
Patient and aneurysm characteristics
Among 121 patients (mean age 58.5±11.9 years, 81 women) with 122 aneurysms who were treated with the WEB device within the study period, angiographic control was available for 103 aneurysms (84.4%). The rates of complete and adequate aneurysm occlusion at the latest available follow-up were 68.9% and 87.4%, respectively. Fifteen patients (14.6%) with incomplete aneurysm occlusion were subjected to retreatment and included in this study. The median patient age at initial WEB placement was 60 years (range 26–73 years) and nine patients (60.0%) were female. Baseline patient and aneurysm characteristics are presented in table 1.
Demographic and aneurysm characteristics of patients with aneurysm recurrences
Six aneurysms were located at the anterior communicating artery, five at the internal carotid artery (terminus 2, paraophthalmic segment 2, posterior communicating artery 1), and four at the basilar tip. Five aneurysms were initially ruptured. The median aneurysm diameter was 9.8 mm (range 5.6–32.6 mm) with a median neck width of 5.2 mm (range 3.8–11.0 mm). The median dome-to-neck ratio was 1.7 (range 1.1–6.8) and all aneurysms were wide-necked.
Procedural details of initial WEB treatment are summarized in table 2. Six aneurysms were treated with a single WEB. Additional devices were used in seven cases (coiling 6, stents 2, flow diverter 1, additional WEB 2). Of these, six aneurysms were larger than the largest available WEB (15 mm) and the WEB was used as part of a multimodal treatment approach (cases 1, 2, 3, 5, 10, 11). In all cases the WEB was used to seal the aneurysm neck once the aneurysm dome had been filled with coils. Two aneurysms were recurrences after initial coiling (case 6, 4 months; case 8, 11 years) that were treated with the WEB.
Initial treatment strategies and angiographic results
Immediate complete aneurysm occlusion after initial WEB placement was obtained in five aneurysms (33.3%), neck remnants in six (40.0%), and aneurysm remnants in four (26.7%).
Retreatment
At angiographic follow-up, 10 patients presented with aneurysm remnants and five with neck remnants. Reasons for retreatment were WEB device migration due to coil compaction (n=6), incomplete occlusion at initial WEB treatment (n=5), and WEB compression (n=4).
The median interval between initial WEB embolization and retreatment was 5 months (range 1–23 months), whereby 14 patients (93.3%) underwent retreatment within the first year after WEB implantation.
Procedural details of aneurysm retreatment are given in table 3. Stand-alone coiling was applied in four patients, whereby a balloon was used in one patient. Additional stents were used in seven cases to prevent protrusion of the coils into the vessel lumen due to a wide aneurysm neck and an unfavorable dome-to-neck ratio. Three recurrent aneurysms were treated by flow diversion. In one case, a giant aneurysm (27.0 mm) was initially treated with coiling and additional implantation of two WEBs and a flow diverter to prevent coil protrusion (case 10). Angiographic follow-up showed migration of the WEBs due to coil compaction. Due to the limited retreatment options after flow diverter use, two additional flow diverters were implanted with the help of a balloon. Initial contrast stasis was achieved and angiographic control showed complete aneurysm occlusion.
Retreatment strategies with clinical and angiographic outcome
One patient was treated by implantation of an additional WEB device. In this case, a giant and partially thrombosed anterior communicating artery aneurysm was initially treated with two WEBs and additional coiling. During follow-up coil compaction occurred and resulted in WEB migration, which left a free space for placement of an additional WEB.
All retreatment procedures were technically successful. Immediate complete aneurysm occlusion was achieved in 13 cases (86.6%) and neck remnant in two cases (13.4%). Illustrative cases of retreatment are presented in figures 1–3.
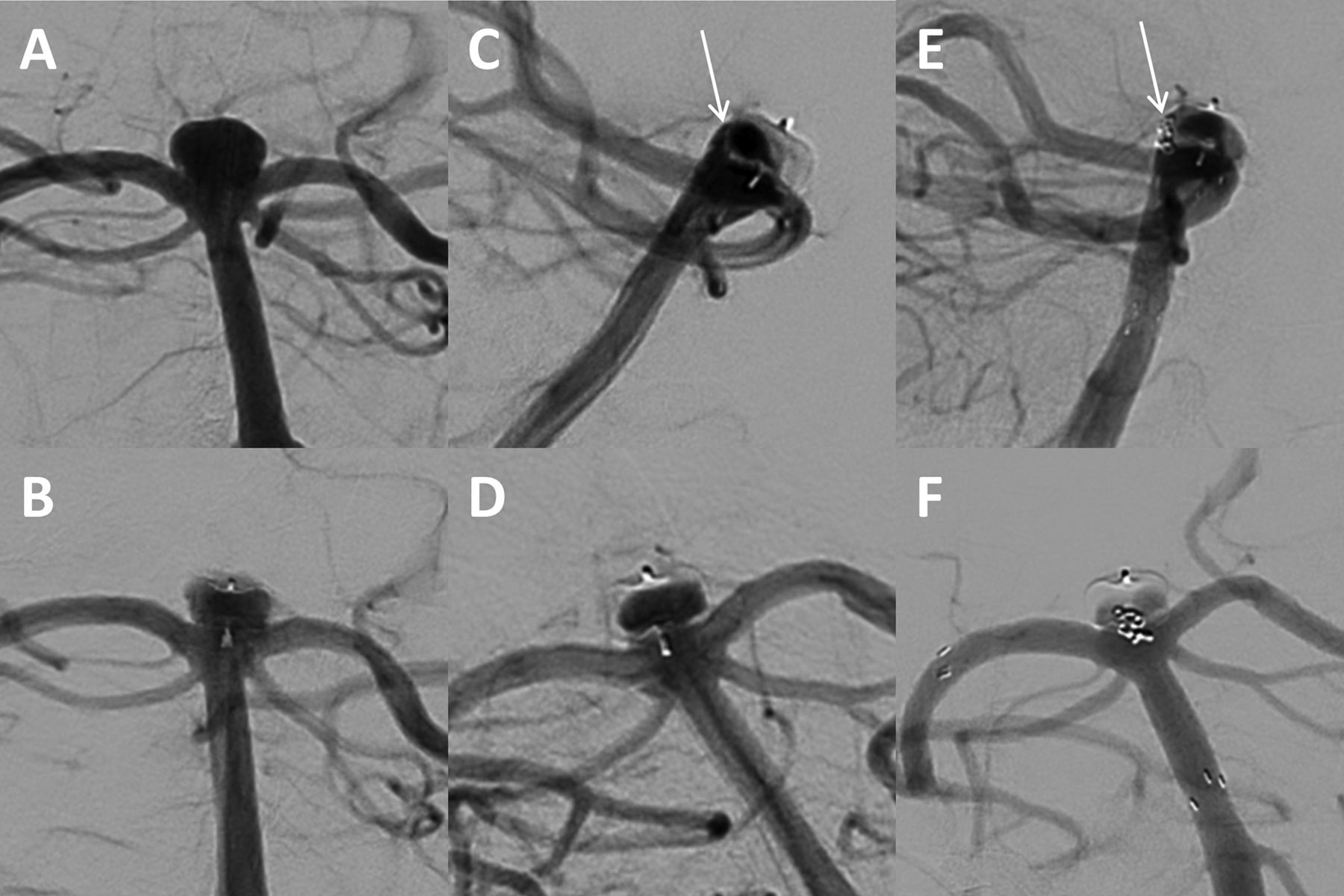
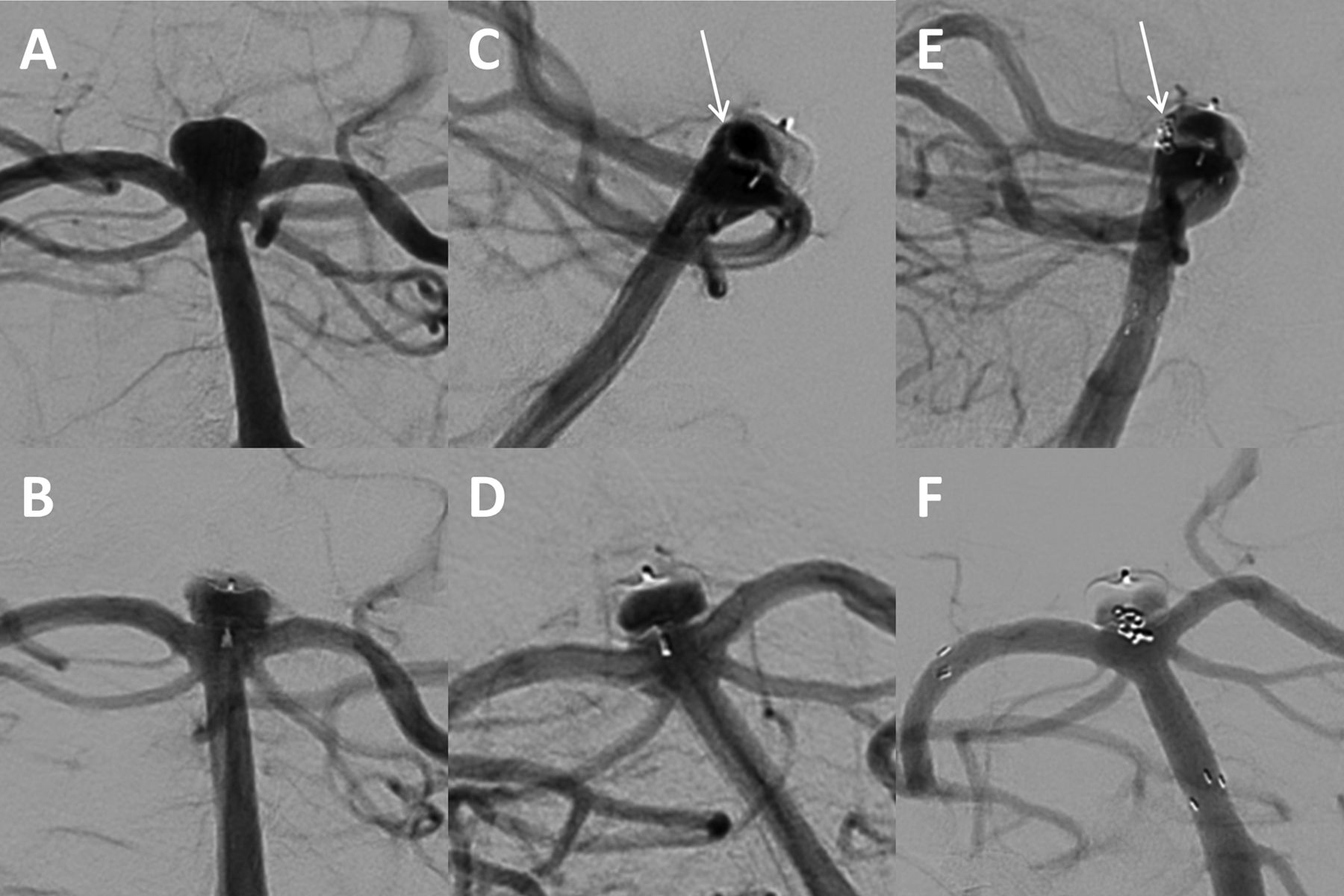
(A, B) A wide-necked unruptured aneurysm at the basilar tip (6.4×4.9 mm) was treated with a WEB SL 6×3 mm after a WEB SL 7x3mm had to be removed because of prolapse into the parent artery (not shown). (C, D) At 6-month angiographic follow-up, digital subtraction angiography shows incomplete occlusion with a small recess between the WEB and the posterior aneurysmal wall (arrow) due to insufficient thrombosis of the aneurysm. There was no change in WEB morphology and position. (E, F) The aneurysm remnant was retreated by implantation of a Neuroform Atlas microstent from the right posterior cerebral artery into the basilar artery, covering the aneurysm neck, followed by embolization of the posterior recess with a single coil (arrow). Immediate angiographic control shows occlusion of the recess and significant stasis within the WEB device.

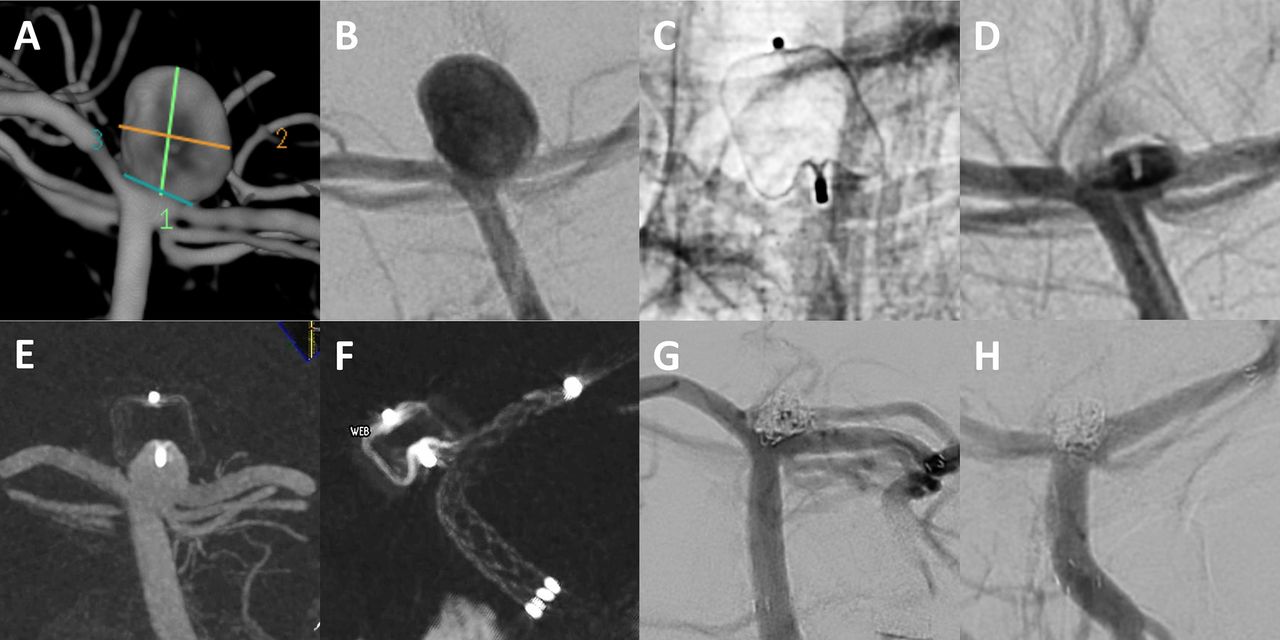
(A) A wide-necked unruptured aneurysm at the internal carotid artery/superior hypophyseal artery (7.8×8.2 mm) was treated with a WEB DL 8×6 mm. (B) Immediately after WEB implantation a small neck remnant remained. At 5-month follow-up, digital subtraction angiography (DSA) (C) and 3D DSA reconstruction (D) showed a recurrent aneurysm due to WEB compression. (E) The aneurysm was retreated by implantation of a FRED flow diverter. (F) DSA after 32 months shows complete occlusion of the aneurysm remnant.
{kind=link}
{kind=link}
{kind=link}
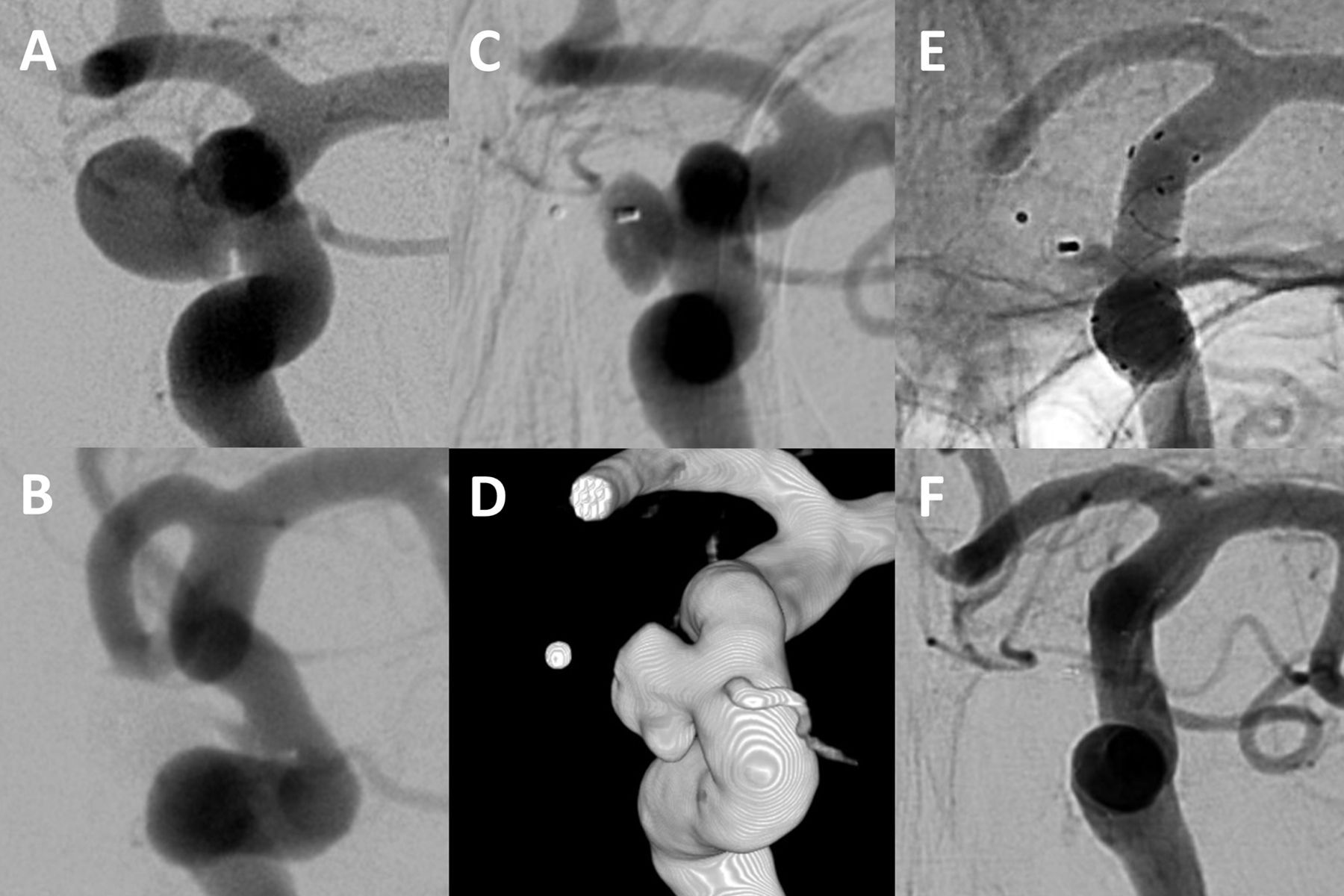
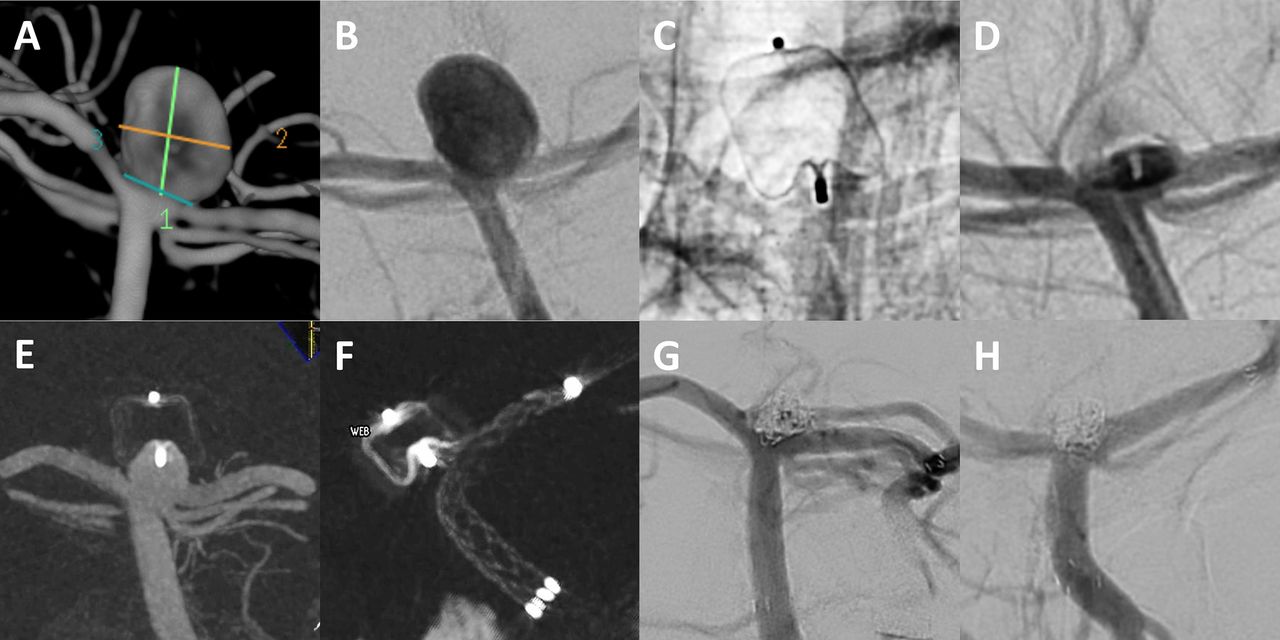
Three-dimensional rotational angiography (A) and digital subtraction angiography (DSA) (B) show a ruptured aneurysm at the basilar tip (7.8×7.4 mm). The aneurysm was treated with a WEB SL 8×5 mm (C), achieving immediate complete occlusion (D). Angiographic control after 9 months showed an aneurysm remnant due to WEB compression (E). The aneurysm remnant was retreated by a combination of Enterprise microstent (F) and coiling (G). Ten months after retreatment, DSA shows complete aneurysm occlusion (H).
Complications
There was no intraoperative aneurysm rupture. Moreover, symptomatic or asymptomatic thromboembolic complications did not occur in any case. We did not observe any delayed adverse events during a median clinical follow-up period of 36 months (range 8–54 months). There was no procedure-related morbidity and mortality in any patient at discharge or during clinical follow-up.
Angiographic outcome
After retreatment, 11 patients were available for angiographic control with a median follow-up period of 17 months (range 6–43 months). Complete aneurysm occlusion was attained in six cases (54.5%) and neck remnants in five (45.5%). There were no aneurysm remnants.
Three patients with neck remnants underwent a second retreatment by means of endovascular coil occlusion (case 1), WEB + coils (case 2), or stent-assisted coiling (case 3). All three aneurysms had a complex configuration and were initially treated with the WEB and multiple additional devices. The reason for recurrence after the first retreatment was coil compaction in all three cases. The decision for second retreatment was made because we assumed an increased risk of further aneurysm growth and potentially spontaneous aneurysm rupture due to the large size (>20 mm) and complex configuration of the aneurysm.
At last angiographic follow-up (median 23 months, range 6–43 months), adequate aneurysm occlusion was attained in all cases (complete occlusion, 8; neck remnant, 3).
Discussion
In the current study we present our ‘real-world’ experience in the treatment of residual or recurrent aneurysms after WEB implantation. Of 15 aneurysms included in the study, six were initially treated by a WEB only, seven in combination with other endovascular techniques, and two were pretreated by coiling. In six cases the WEB was used off-label as part of a multimodal treatment approach for large aneurysms that exceeded the largest available WEB, as described in a previous publication.6 Since treatment options for these aneurysms are generally limited, we used the WEB to seal the aneurysm neck after filling the aneurysm dome with coils to prevent coil protrusion, assuming the WEB to be superior to standard coiling based on our previous experience with this device. As there is direct contact with the WEB during retreatment, we did not exclude these aneurysms from the study.
Since 2011 the WEB device has emerged as a safe and efficient option for endovascular treatment of wide-necked and bifurcation aneurysms which are otherwise difficult to treat by conventional endovascular means. In the cumulative population of the three prospective studies WEBCAST (WEB Clinical Assessment of Intrasaccular Aneurysm), WEBCAST-2, and French Observatory, complete and adequate occlusion at 1-year follow-up was observed in 52.9% and 79%, respectively, and retreatment was performed in 6.9%.4 In our series, similar angiographic results were obtained. The rates of complete and adequate aneurysm occlusion after WEB implantation were 68.9% and 87.4%, respectively, thus confirming the high efficacy of the WEB. However, the retreatment rate of all aneurysms with available angiographic follow-up in our series was 14.6%, which is within the upper range of retreatment rates reported in previous comparable studies.3 7 To some extent this may be related to the fact that we also used the WEB off-label as part of a multimodal treatment approach for several large and partially thrombosed aneurysms that are not indicated for WEB placement according to the device IFUs but otherwise also extremely challenging to treat as described in a previous publication.6 Independent of the endovascular treatment strategy, these aneurysms are known to carry a high risk of recurrence.8 9
In our study population we identified two reasons for aneurysm recurrence: device migration and WEB compression. WEB device migration means that the WEB has moved from the initial site of placement into the aneurysm sac, whereas the aneurysm size remains stable. In our series, device migration occurred in six aneurysms. Interestingly, this phenomenon was only observed in aneurysms treated by a combination of WEB and coiling. In all cases, the aneurysm was larger than 15 mm and the coils were placed within the aneurysm dome, whereas the WEB covered the aneurysm neck to prevent coil protrusion. Therefore, it may be speculated that coil compaction allows the blood flow to push the WEB distally into the aneurysm sac.
Due to its oblong shape and its shape memory, the WEB was initially expected to be less prone to compaction than coils. However, several studies described a phenomenon called ‘WEB compression’, which means a decrease in the height of the device due to the deepening of the device recesses at both sides resulting in partial reperfusion of the sac.10–12 According to a recent study with core laboratory evaluation of anatomic results, modification of the WEB shape occurs in approximately 30% and seems not to be related to WEB sizing.11 WEB compression can lead to aneurysm recurrence, mostly small neck remnants which generally do not require retreatment.11 However, in our series we included four aneurysms in which aneurysm recurrence could be related to WEB compression. All of these aneurysms were initially treated by a single WEB without ancillary devices.
Generally, recurrent aneurysms carry an increased risk of spontaneous aneurysm rupture and may therefore require retreatment. However, retreatment of aneurysms after WEB implantation has not been studied in detail and the clinical and angiographic outcome remains uncertain. To date, there is only one published case report on recoiling after WEB implantation.5 Hence, retreatment strategies after WEB implantation remain a subject of debate and neurointerventionalists might feel unsure how to deal with WEB recurrences. Thus, physicians may tend towards further angiographic follow-up rather than retreatment, which might increase the risk of spontaneous aneurysm rupture and subarachnoid hemorrhage.10
The current study is the first to evaluate the treatment strategies for recurrent or residual aneurysms after WEB embolization in a larger case series. The results of our series show that retreatment of aneurysms after WEB embolization can be performed with a high rate of technical success and procedural safety. The selection of the appropriate endovascular method for retreatment after WEB implantation was predominantly based on anatomical considerations. Stand-alone coiling was considered as first choice for aneurysm retreatment, since this method is associated with low complication rates and does not per se require antiplatelet medication. In these cases, the microcatheter was placed within the recanalized aneurysm lumen between the WEB device and the aneurysmal wall. The space between the WEB, aneurysm wall, and parent artery could then be reliably embolized with coils, leaving the WEB unaffected. The operators note that visbility of the neck remnant independent of working projection made radiographic control over WEB recurrence easier compared with coil recurrence where platinum might obscure the view to some extent.
Since the WEB is usually used for wide-necked and bifurcation aneurysms, stand-alone coiling is not always feasible for retreatment due to unfavourable anatomical configuration. Additional stents were implanted if the coils could not be securely placed within the reperfused aneurysm cavity and tended to prolapse into the vessel lumen. In all these cases, the previously placed WEB did not pose a problem for stent placement.
The use of flow diverters for treatment of recurrent aneurysms is not yet widely established, but has shown promising aneurysm occlusion rates and an acceptable morbidity in case series.13 In the current study, three patients with recurrent aneurysms at the internal carotid artery were treated by flow diversion to redirect the blood flow away from the aneurysm lumen. However, flow diverters are rarely used for bifurcation aneurysms, which constitute the majority of aneurysms treated by the WEB.
Generally, retreatment of aneurysms after multimodal treatment was technically not different from aneurysms treated with a single WEB. In particular, we did not observe iatrogenic device migration in the aneurysms that were initially treated by WEB and coil. In our series the rate of recurrent aneurysms treated with additional devices was rather high (80%), which presumably reflects the complexity of these aneurysms. Of note, 11 of 15 aneurysms were eventually retreated by using stents or flow diverters. As a consequence, these patients require double antiplatelet medication. This analysis indicates that stand-alone coiling is often not sufficient for retreatment after WEB implantation, which might be attributed to the unfavorable aneurysm configuration (wide neck and/or low dome-to-neck ratio). However, by applying the described endovascular techniques, we were able to achieve a noticeable reduction in contrast opacification of the reperfused aneurysm sac in all cases. Immediate complete occlusion was obtained in 13 of 15 cases and neck remnants in two cases.
In the current literature, the rate of aneurysm recurrence after a second endovascular treatment is reported to be 15–50%.14–17 In accordance, 54.5% of our retreated aneurysms presented with a neck remnant at further angiographic control and three aneurysms were retreated for a second time. These three aneurysms were initially larger than 20 mm and were previously treated by using a multimodal approach. In this context, aneurysm size is the main prognostic factor in stable aneurysm occlusion after a second coil embolization following aneurysm recurrence.14 Finally, stable adequate occlusion could be achieved in all aneurysms that were available for angiographic follow-up.
In general, the occurrence of complications and morbidity related to WEB implantation is considered to be quite low. A recent meta-analysis found complication rates of 14% (95% CI 9% to 19%); serious adverse events were mainly related to thromboembolism and hemorrhage.18 In our series there were no procedural adverse events and no treatment-related morbidity or mortality. Moreover, we did not observe any thromboembolic events, although all aneurysms were wide-necked, which constitutes a potential risk factor for thrombus formation.19 Concerns of iatrogenic WEB dislocation causing hemorrhagic or ischemic complications or even aneurysm rupture were not justified. Furthermore, we did not observe any delayed adverse events or morbidity during a cumulative follow-up of 10.5 patient-years. As has been shown for recoiling in the past, endovascular retreatment after initial WEB placement also carries a low risk of complications, explicitly lower than that of the initial aneurysm obliteration.20 The results of our series confirm a good safety profile for the retreatment of aneurysms after initial WEB embolization, even for complex aneurysms that are wide-necked or pretreated with multiple devices.
Study limitations
The limitations of this study are mainly related to its retrospective design and the limited number of included patients. The aneurysms were heterogenous in size and configuration and different treatment methods were used, both for initial WEB embolization and for retreatment. These limitations make a general recommendation on aneurysm retreatment after WEB embolization difficult. Being aware of these limitations, we believe that our study provides valuable information for the management of aneurysm remnants after WEB implantation, which may facilitate the decision-making process of other neurointerventionalists. Further studies with a more homogenous patient sample will be necessary to confirm our results and to identify the best suited retreatment strategies for residual and recurrent aneurysms after WEB implantation.
Conclusions
The current series shows that retreatment of recurrent and residual aneurysms after initial WEB implantation can be accomplished with a high degree of technical success and with low morbidity. The efficacy of endovascular aneurysm retreatment is good, with adequate aneurysm occlusion seen in all of our cases at mid-term follow-up. Larger studies will be helpful to develop individualized management strategies for treatment of recurrent and residual aneurysms after WEB embolization.
References
Footnotes
CK and LG contributed equally.
Contributors LG, CK, ES, MH, CH, AM and FD acquired the data. CK, LG and TL developed the project, analyzed the data and drafted the manuscript. All authors revised the paper critically for important intellectual content and provided final approval of the version published. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. CK and LG contributed equally as first authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests CK and FD serve as consultants for Acandis GmbH (Pforzheim, Germany). TL serves as proctor for MicroVention Inc/Sequent Medical (Aliso Viejo, California, USA). The other authors declare that they have no competing interests.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data will be made available upon request in an anonymized manner.