Article Text

Abstract
Background and purpose Evidence on how to select microcatheters to facilitate aneurysm catheterization during coil embolization is sparse. We developed a new method to define microcatheter tip location inside a patient-specific aneurysm model as a 3-dimensional probability map. We hypothesized that precision and accuracy of microcatheter tip positioning depend on catheter tip shape and aneurysmal geometry.
Materials and methods Under fluoroscopic guidance two to three operators introduced differently shaped microcatheters (straight, 45°, 90°) into eight aneurysm models targeting the anatomic center of the aneurysm. Each microcatheter position was recorded with flat-panel CT, and 3-dimensional probability maps of the microcatheter tip positions were generated. Maps were assessed with histogram analyses and compared between tip shapes, aneurysm locations and operators.
Results Among a total of 530 microcatheter insertions, the precision (mean distance between catheter positions) and accuracy (mean distance to target position) were significantly higher for the 45° tip (1.10±0.64 mm, 3.81±1.41 mm, respectively) than for the 90° tip (1.27±0.57 mm, p=0.010; 4.21±1.60 mm p=0.014, respectively). Accuracy was significantly higher in posterior communicating artery aneurysms (3.38±1.20 mm) than in aneurysms of the internal carotid artery (4.56±1.54 mm, p<0.001).
Conclusion Our method can be used tostatistically describe statistically microcatheter behavior in patient-specific anatomy, which may improve the available evidence guiding microcatheter shape selection. Experience increases the ability to reach the intended position with a microcatheter (accuracy) that is also dependent on the aneurysm location, whereas catheter tip choice determines the variability of catheter tip placements versus each other (precision). Clinical validation is required.
- aneurysm
- catheter
- intervention
Statistics from Altmetric.com
Introduction
Endovascular treatment is a widespread therapeutic option for intracranial aneurysms with continuous development of new techniques and devices.1–4 Various options including coil embolization, flow disruption and coil-assisted stent or flow diverter placement are available and require aneurysm probing with a microcatheter.5–7 For intracranial aneurysms needing sole flow diverter treatment without adjunctive coiling, microcatheter selection of the aneurysmal sac is not necessary.8 9 Safe microcatheter navigation within the parent vessel and the aneurysmal sac is therefore required to avoid complications such as aneurysmal perforation, thrombus formation or prolapse of implants into adjacent vessels.10 The ease and safety of aneurysm probing is remarkably dependent on the anatomy, with some aneurysm locations and shapes having greater problems of access than others.11–13 To facilitate navigation into the aneurysmal sac and subsequent coil embolization, differently shaped microcatheter tips are available which are designed to avoid problems in crossing the aneurysm neck or vascular ostia or avoid advancing coils directly against the aneurysm wall.11 14 15 There is, however, little evidence to guide operators when choosing between microcatheter tip shapes. Previous authors have suggested that custom shaping of microcatheters according to a patient-specific aneurysm model can be performed.7 12 Lee and colleagues described the utility of z-shaping catheters for accessing proximal anterior cerebral artery aneurysms.16 These analyses, however, did not directly compare these approaches to more conventional microcatheter shapes. To our knowledge, no study has directly compared the different tip shapes available for aneurysm selection.
We developed a method to statistically describe microcatheter tip location in aneurysm models that are based on real patient anatomy. We hypothesized that the microcatheter tip position, with its parameters positional precision and positional accuracy as well as the duration of probing depends on the tip shape, aneurysm location and the operator’s experience. We tested these hypotheses to see whether our method for describing microcatheter positioning is valid. For this initial study, eight patient-specific aneurysm models were fabricated using a 3D printer and were repeatedly catheterized in vitro by one to three independent operators.
Materials and methods
Data selection
This was a single-center study approved by an institutional review board, which waived the requirement for individual consent owing to anonymized analysis. We retrospectively selected 3D rotational angiography data (Allura Clarity FD 20/20 angiography system, Philips Healthcare, Best, the Netherlands) from eight patients with four incidental internal carotid artery (ICA) aneurysms (two paraophthalmic and two near the carotid ‘T’), one incidental aneurysm of the posterior communicating artery (PcomA) and three patients with aneurysms of the PcomA presenting in the setting of subarachnoid hemorrhage, respectively. These data were acquired with the following parameters: 5 s rotational acquisition, 220° rotation, 150 single frames at a frame rate of 30/s, 27 cm detector field of view (FOV), 512 acquisition matrix. Images were reconstructed using an intermediate kernel with an isotropic voxel size (0.08 mm). All image data were anonymized before being used in this study. Dimensions, clinical treatment and 3D CAD (computer-aided design) aneurysm models of all eight aneurysms are described in figure 1.
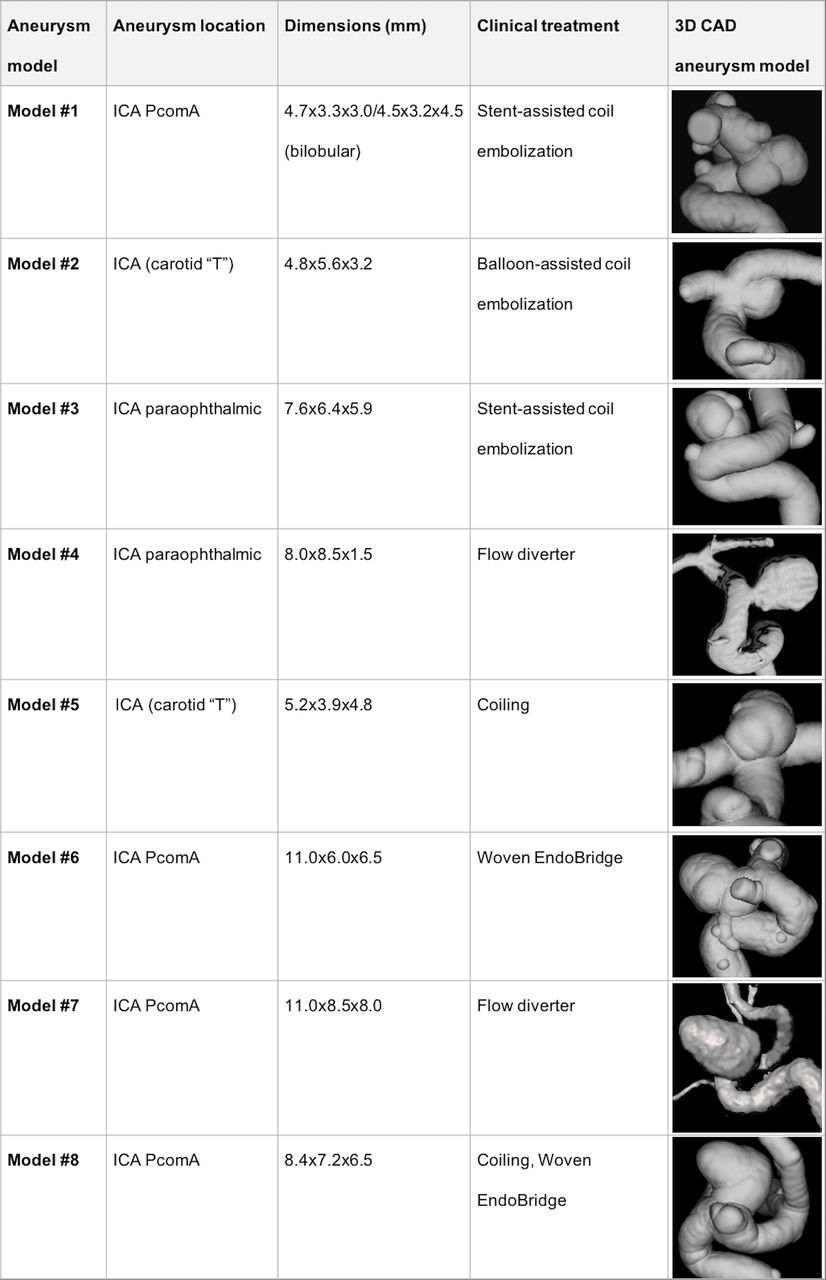
Characteristics of experimental set-up and provision including 3D computer-aided design (CAD) illustration of all eight aneurysm models. ICA, internal carotid artery; PcomA, posterior communicating artery.
Aneurysm models and experimental set-up
Volumetric surface data of a hollow aneurysm models suitable for additive manufacturing were obtained from 3D rotational angiography data after processing with Analyze 11.0 (AnalyzeDirect, Inc, Overland Park, Kansas, USA) and CATIA V5 (Dassault Systèmes SA, Vélizy-Villacoublay, France), as previously described.17 The wall thickness of the hollow models was 1.0 mm. The models depicted patient anatomy starting at the petrous portion of the ICA and reaching distally to the middle cerebral artery bifurcation. Models were produced by an external manufacturer (TBKO - Thomas Bengel Konstruktion+Prototypen, Messstetten, Germany) using a commercially available machine (OBJET Connex, Stratasys Ltd, Eden Prairie, Minnesota, USA) with an elastic, semitransparent building material (TangoPlus FLX930 27 Shore A).17 Several examples of each aneurysm model were obtained.
The experimental set-up consisted of a dedicated experimental angiography system (Allura Clarity FD 20 angiography system, Philips Healthcare, Best, the Netherlands). Aneurysm models were connected to a flow circuit and a pump, continuously providing water at room temperature in the system. A straight silicone tube was used to replace the aortic and cervical access route. Contrast medium diluted to 100 g iodine/L (Imeron, Bracco Imaging S.p.A., Milano, Italy) was added to enable visualization of the lumen under fluoroscopy.
Table 1 shows the characteristics of the experimental design. Under fluoroscopic guidance, two operators with various levels of experience in aneurysm embolization ranging from 0 to 3 years independently introduced three differently shaped microcatheters (Excelsior 1018 straight, preshaped 45° tip and preshaped 90° tip; Stryker Neurovascular, Fremont, California, USA) into aneurysm model #1 and #2, while the third operator introduced two differently shaped microcatheters (Excelsior 1018 straight and preshaped 45° tip, Stryker Neurovascular, Fremont, California, USA) into aneurysm model #1 and three differently shaped microcatheters (Excelsior 1018 straight, preshaped 45° tip and preshaped 90° tip, Stryker Neurovascular, Fremont, California, USA) into aneurysm model #2. All three differently shaped microcatheters were additionally introduced into aneurysm models #3 to #8 by operators 1 and 2, respectively. Each microcatheter tip shape was used a total of 10 times by one operator, completing all 10 insertions into one aneurysm model. A new catheter was subsequently provided for the next operator. The aneurysm sac was catheterized with the help of a 0.014" microwire (Traxcess, MicroVention, Tustin, California, USA). Guidewires were exchanged for new wires at the operator’s discretion.
Characteristics of experimental setup and provision
Operators were asked to position the microcatheter tip as close to the center of the aneurysm as possible and to stop when they achieved a position suitable for starting coil embolization. The time needed from the start of microcatheter navigation to the final position was recorded in each instance.
After each microcatheter placement, the microwire was removed and we obtained a flat-panel CT scan (VasoCT; 220° rotation, 617 single frames at a frame rate of 30/s, 22 cm detector FOV and 512 acquisition matrix). The aneurysm and surrounding vessels were reconstructed using a 17% FOV, sharp kernel, isotropic voxel size (0.1 mm).
Imaging analysis and statistics
All reconstructed flat-panel CT images were processed by rigid affine intramodal coregistration.18 The results of coregistration were visually verified. Density thresholding and subsequent binarization were performed to exclude everything but the high-density microcatheter markers from the image volume. Masking of the proximal microcatheter marker to visualize only the distal marker inside the aneurysmal sac was performed (MATLAB R2014b, The MathWorks Inc., Natick, Massachusetts, USA; 2014). The resulting volume thus contained voxels with a value of ‘1’ corresponding to the distal microcatheter tip with all other voxels containing a value of ‘0’. Three-dimensional probability maps of all microcatheter tip positions were generated by adding the resulting binary positional maps of each microcatheter placement and dividing by the number of placements performed using MATLAB and MRIcron software (University of South Carolina, Columbia, South Carolina, USA). Analyses for positional accuracy and precision for all microcatheters and operators were performed using MATLAB. Continuous variables were compared using Student’s t-test and analysis of variance with MedCalc Statistical Software version 17.5 (MedCalc Software bvba, Ostend, Belgium; http://www.medcalc.org; 2017) and IBM SPSS Statistics 24 (SPSS Statistical Software; IBM, Armonk, USA).
Positional accuracy and precision
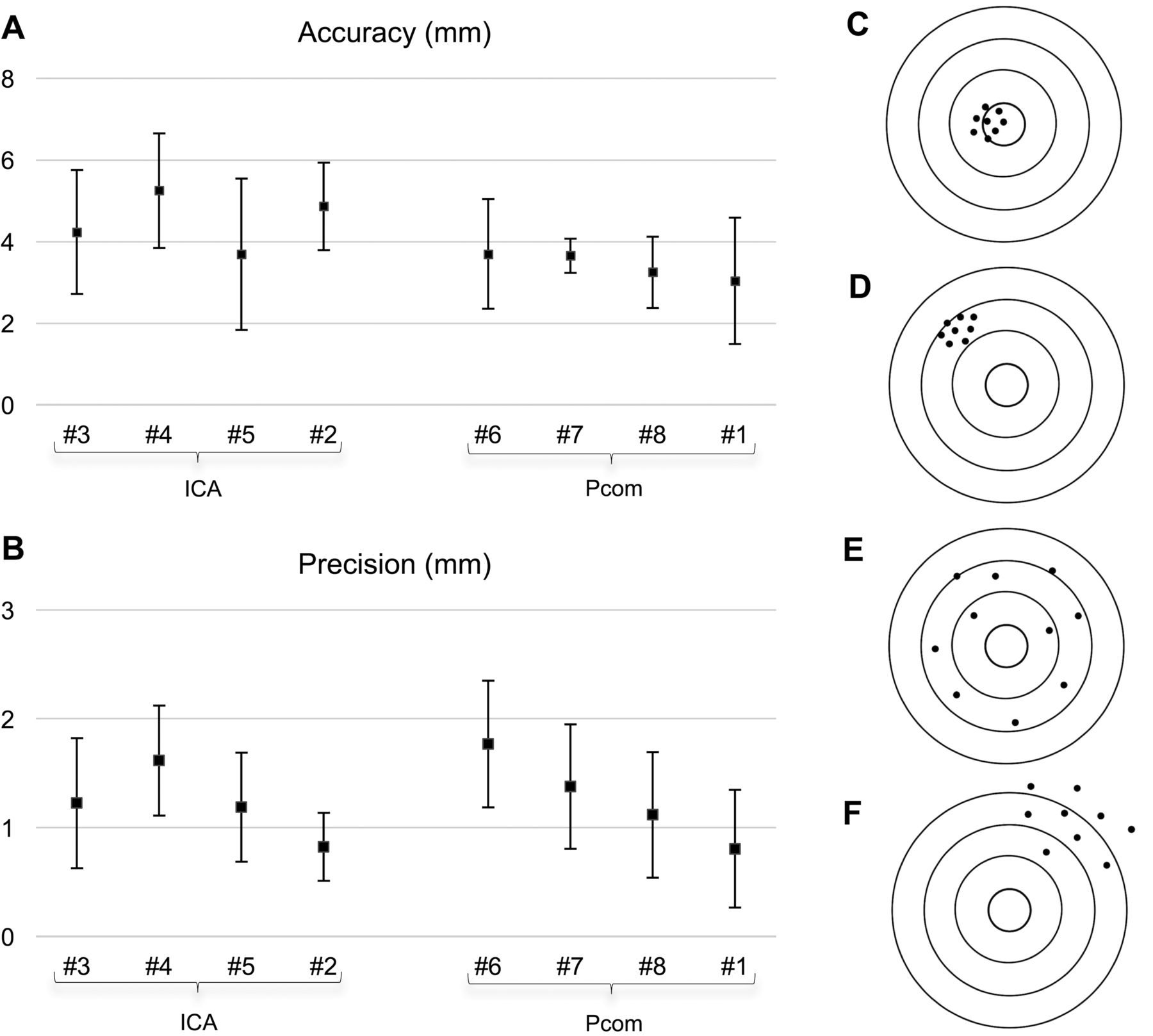
The target position was defined arbitrarily as the anatomic center of the aneurysm. The target position was manually defined once for each aneurysm model by operator 2 using a multiplanar reformation in three orthogonal planes with MRIcron software (University of South Carolina, Columbia, South Carolina, USA). Distances of the microcatheter tip from the target position were calculated using MATLAB. Three-dimensional microcatheter tip accuracy was defined as the average distance (mm) between the microcatheter tip and target position.19–21 Precision as a measure of variability of positioning was defined as the distribution of distances between the different final microcatheter tip positions.19–21 Accuracy and precision are illustrated in figure 3 (see ’Results').
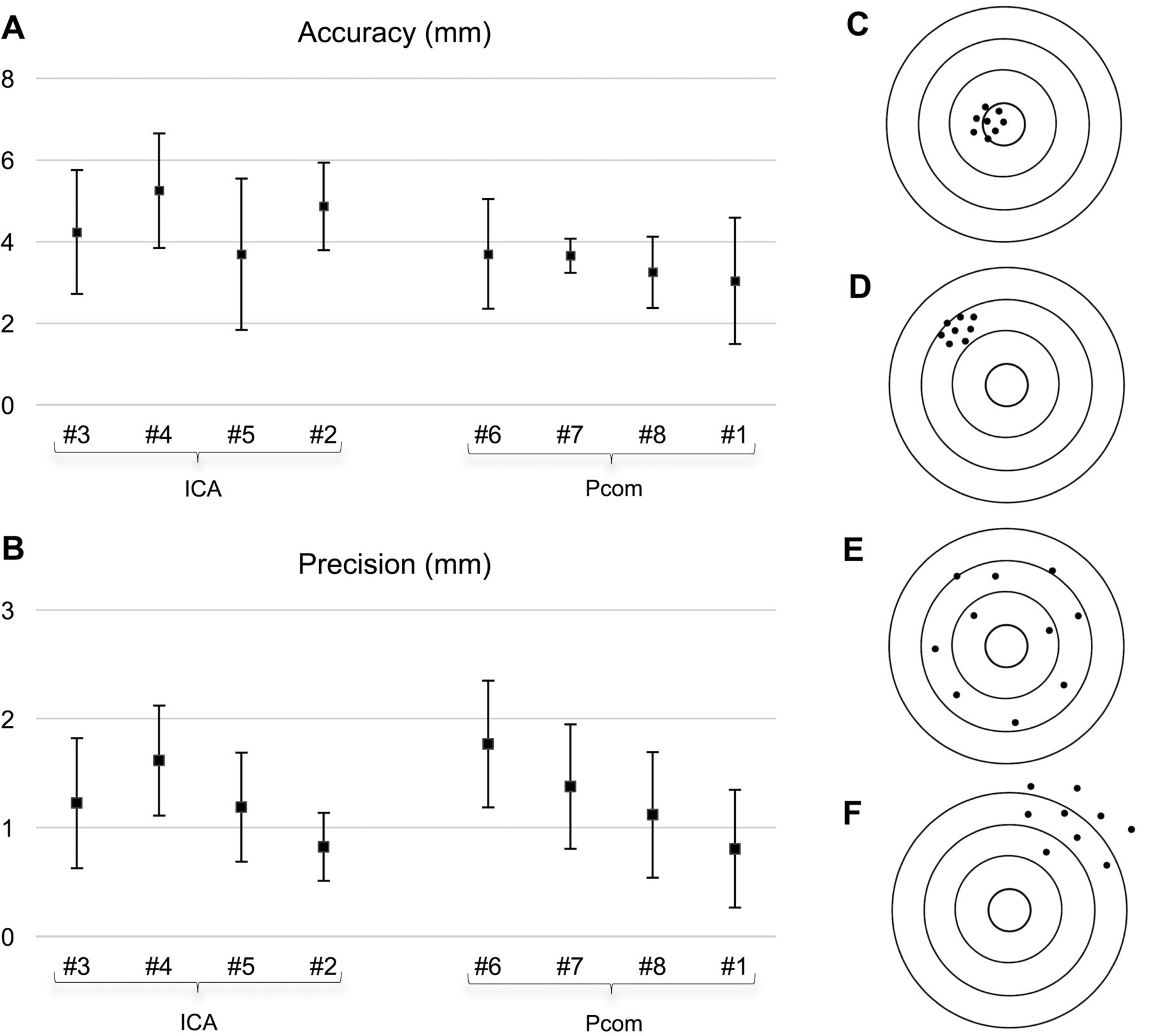
Illustration of accuracy and precision for all measurements in eight aneurysm models divided by aneurysm location; means shown by squares and columns representing standard deviations. (A) Accuracy was higher (smaller values) for posterior cerebral artery aneurysms compared with internal carotid artery aneurysms. (B) Precision displayed higher variabilities within the different aneurysm groups. (C) High accuracy, high precision. (D) Low accuracy, high precision. (E) High accuracy, low precision. (F) Low accuracy, low precision.
Results
Probability maps of the microcatheter tip position
A total of 530 microcatheter insertions were successfully performed in all eight aneurysm models. Six out of 530 flat-panel CT acquisitions had to be excluded owing to inaccurate coregistration. From the 524 flat-panel CT datasets, probability maps were successfully generated for each aneurysm model, operatorand tip shape.
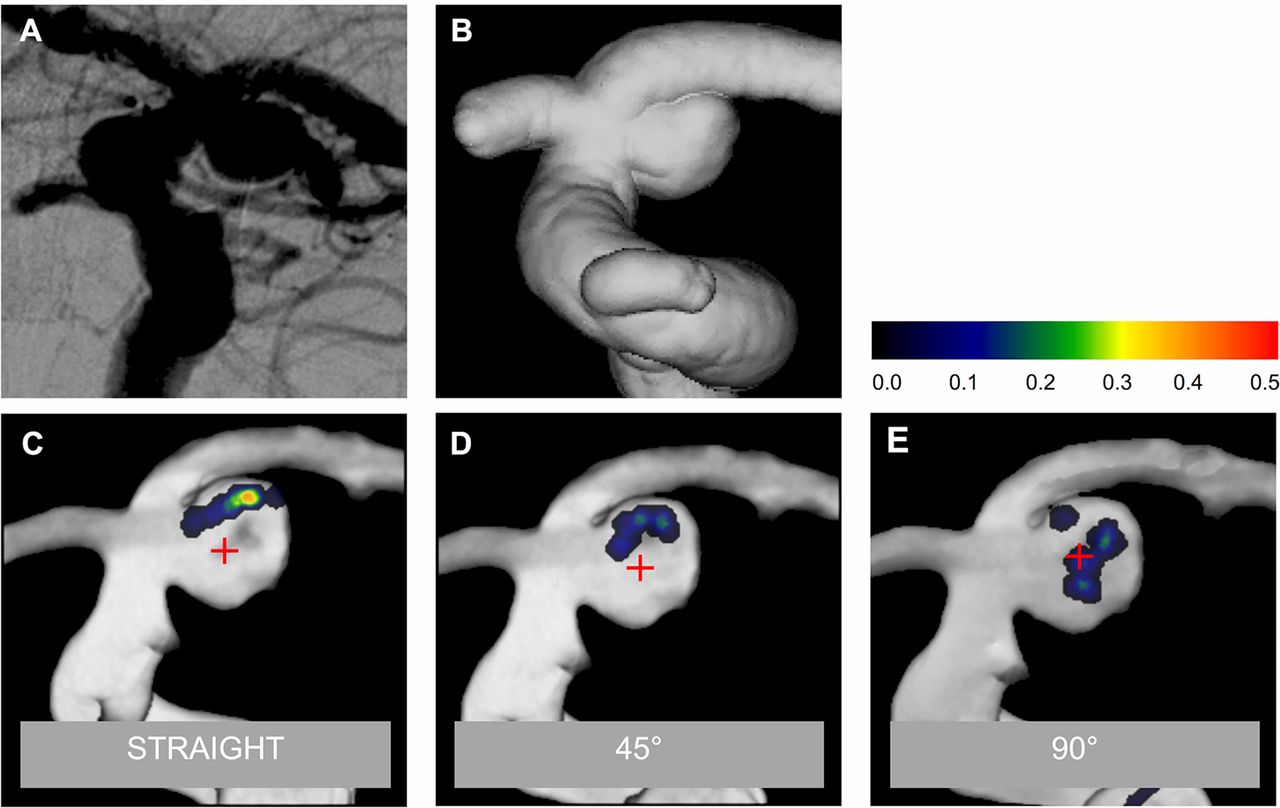
Figure 2 shows the probability maps of three different microcatheters (Excelsior-1018 straight and Excelsior-1018 with a preshaped 45°or 90° tip) from all operators in aneurysm model #2.

Distinct 3D probability maps for aneurysm model #2 projected onto a volume rendering. Colored areas demonstrate the distal marker of the microcatheter. Color scale showing tiered probabilities of microcatheter tip positions of the 30 insertions for each catheter shape by all three operators (value of 0.5 resembling a microcatheter tip probability of 50%). (A) Pretreatment DSA working view. (B) Image of the aneurysm model before 3D printing. (C) Excelsior-1018 straight. (D) Excelsior-1018 45° tip. (E) Excelsior-1018 90° tip.
Accuracy and precision
Online supplemental table 2 displays the accuracy and precision for all aneurysms considering all measurements and microcatheters as variables. Comparison of different tip shapes showed that precision was significantly higher for the 45° shaped microcatheter (1.10±0.64 mm) than for the 90° shaped microcatheter (1.27±0.57 mm, p=0.010). Positional accuracy was significantly higher for the 45° tip shaped microcatheter (3.81±1.41 mm) than for the 90° shaped microcatheter (4.21±1.60 mm, p=0.014).
Supplemental material
For comparison of precision and positional accuracy between operators, only operator 1 (0 years of experience) and operator 2 (3 years of experience) were considered for evaluation. No significant difference in accuracy was detected between operator 1 (4.13±1.7 mm) and operator 2 (3.95±1.2 mm, p=0.167). Precision was significantly higher for the unexperienced operator 1 (1.18±0.6 mm) than for the more experienced operator 2 (1.32±0.6 mm, p=0.013). Results are shown in online supplemental table 3.
Online supplemental table 4 shows the accuracy and precision for all three differently shaped microcatheters dependent on all aneurysm models. Significant differences in accuracy and precision were observed between the different aneurysms (p<0.001). Aneurysm models were subsequently sorted by anatomical location (group 1=ICA aneurysms, group 2=PcomA aneurysms). Mean aneurysm volume was not significantly different between these groups (ICA: 74.8±50.3 mm³, PcomA: 211.8±150.5 mm³; p=0.135). Accuracy was significantly higher for the PcomA aneurysms (3.38±1.20 mm) than for the ICA aneurysms (4.56±1.54 mm, P<0.001). Precision showed no significant difference between the two groups (ICA: 1.17±0.55 mm, PcomA: 1.23±0.67 mm, p=0.297).
Figure 3 shows the positional accuracy and precision for all eight aneurysms, subdivided according to one of the aneurysm groups (ICA and PcomA).
Figure 4 visualizes the positional accuracy and precision for two selected aneurysms treated by the same operator, comprising all three different microcatheter tip shapes (straight, preshaped 45° tip and preshaped 90° tip). Aneurysm #2 displayed a fairly high precision and a poor accuracy. The accuracy appeared high in aneurysm #6 whereas precision simultaneously was rather low.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of microcatheter accuracy and precision for two aneurysms, green color illustrating straight microcatheter, blue color representing 45° tip shaped microcatheter and red color showing 90° tip shaped microcatheter placements. (A) Aneurysm #2 showed a high precision (0.82±0.31 mm). (B) In aneurysm #6 the precision was lower (1.77±0.58 mm).
Catheterization times
We observed no significant difference in catheterization times between the straight microcatheter (40.3±28.0 s), the 45° shaped microcatheter (34.6±19.7 s) and the 90° shaped microcatheter (34.7±28.2 s, p=0.056). Probing times for PcomA aneurysms were significantly shorter (32.3±20.8 s) than for ICA aneurysms (40.6±29.1 s, p<0.001).
Comparison of probing times of operator 1 and operator 2, considering all aneurysms, showed significantly shorter times for the more experienced operator (23.9±10.0 s) than for the inexperienced operator (49.5±31.8, p<0.001).
Discussion
We developed a method to describe statistically the location of a microcatheter tip inside a patient-specific aneurysm model as a 3D probability map. This tool thus allows characterization of microcatheter behavior in a defined in vitro setting. The method can be used to gather evidence on the behavior of different microcatheter shapes, sizes, and operators. As a precise microcatheter location inside the aneurysm sac distant from the vessel wall has been shown to reduce the risk of intraprocedural aneurysm rupture, we assessed the parameters accuracy and precision in our experimental setup.22 23 If a sufficient number of different aneurysms and catheter shapes are tested, such data may reveal general principles about the optimal shape of microcatheters for specific anatomic locations, directionalities or shapes.
With the initial application of this new method in eight aneurysms, we observed that microcatheter precision and accuracy depend on the microcatheter tip shape, showing lower values for the 45° shaped microcatheter than for the straight and the 90° shaped microcatheters, although the overall differences were small. Positioning the straight microcatheter seems to be more imprecise as the microcatheter tip has a relatively wide margin pointing in one direction. The greater positional variability of the 90° tip can be explained as a result of the influence of rotation of the microcatheter. As microcatheter rotation is difficult to control, the 90° tip may point in various directions as illustrated in our probability maps (figure 2). Our initial results, therefore, support the hypothesis that the final position of a 45° tip is more precise and accurate, or easier to predict, than that of a straight or 90° tip.
Accuracy, as defined by our method, seems to be highly dependent on the anatomy, as categorization of all aneurysm models into subgroups according to their anatomical location showed significantly lower values for PcomA aneurysms than for other aneurysms of the ICA. This might result from a more straightforward access into PcomA aneurysms due to better alignment of the microcatheter axis and aneurysm axis. In contrast, terminal ICA and paraophthalmic ICA aneurysms may present more difficulties of access and unfavorable anatomies, which may increase probing times. Furthermore, additional conditions such as blebs in the aneurysm model or in the afferent vessels, aneurysm size, and neck diameter might influence accuracy and precision and must be considered for evaluation and further clinical implementation.
Our method might also be used to assess an operator’s ability to catheterize an aneurysm precisely and accurately. However, no significant difference in accuracy was detected between operator 1 and operator 2, when all aneurysm models were compared. Precision was significantly higher for operator 1 (the least experienced operator) than for the more experienced operator 2. This slight difference was associated with longer probing times of the inexperienced operator. Certainly, accuracy, precision and catheterization time are highly selective variables that incompletely reflect operator skill. Assessment of further variables, such as wire movement, force, or interaction with the aneurysm wall may improve this aspect. Furthermore, we observed shorter aneurysm selection times for PcomA aneurysms than for ICA aneurysms, which again supports the hypothesis that PcomA aneurysms are easier to access than other ICA aneurysms.
Three-dimensional printing of intracranial aneurysms offers the possibility to test different endovascular devices in a preoperative setting and enables the operator to work on patient-specific anatomy. Previous studies have emphasized the benefits of such models for surgical planning and education,11 24–26 but there are few data on how to select the microcatheter in advanceand the operator’s preference is mostly based on individual experience.16 Namba and colleagues and Ishibashi and colleagues previously described microcatheter shaping in a preoperative setting using 3D printing technology.7 12 The microcatheter shape was determined by the patient’s anatomy and configuration of the aneurysm and the preshaped mandrel was then applied in the following endovascular procedure.7 12 Microcatheter position was evaluated by Namba and colleagues as the alignment of the microcatheter with the aneurysm axis, showing satisfying results.7 Kwon and colleagues retrospectively investigated 122 patients with paraclinoid aneurysms who underwent endovascular treatment, reporting that different microcatheter shapes were used for aneurysm selection depending on the direction of the aneurysm (superior, medial, other).11 Their data also support the concept that the optimal microcatheter shape depends on aneurysm anatomy.
Beyond a retrospective assessment, our method can now be applied to objectively compare the use of such shaping techniques with conventional microcatheter shapes to assess the success and speed of aneurysm access and the resulting microcatheter positions. This may help to reach a better understanding of which tip shape might be favorable for selecting different anatomical groups of aneurysms. Thus, the most relevant application of our method is to provide objective evidence of microcatheter behavior to facilitate microcatheter selection before endovascular treatment. In addition, our method could possibly be expanded to statistically describe the behavior of other devices or implants—for example flow diverter and stents in real patient anatomy. It might be useful to gather information about the statistical likelihood of the final flow diverter position within a vessel section before performing the endovascular procedure. Such results could therefore help to predict the reproducibility of certain implants.
Since we have not yet systematically validated our model against clinical data, the degree to which the behavior of microcatheters may differ in vivo compared with our model remains uncertain. More data are needed to assess how well the model reproduces clinical conditions. An ideal clinical validation may be hard to achieve as it would require several catheterizations in a single aneurysm with all its associated perforation risk and radiation exposure.
An important limitation of our method is the omission of a complete, patient-specific cervical and thoracoabdominal access route. We chose the starting point of patient-specific anatomy at the petrous portion of the ICA as a compromise between the models’ complexity and anatomic validity, realizing fully that the course of the cervical vessels probably would have changed our results. In clinical practice, aortic configuration and cervical vessel curvature strongly affect the ability to navigate the intracranial vessels. Other limitations include the limited number and locations of aneurysms, which was too small to draw final conclusions on microcatheter behavior. Furthermore, the use of adjunctive techniques, such as balloon-remodeling, may alter microcatheter behavior. We employed only models made from one material with one manufacturing approach at room temperature. This influences the surface friction of the model, thus affecting microcatheter navigation. Applying each microcatheter 10 times to probe one aneurysm might affect both accuracy and precision owing to deformation of the tip shape. Furthermore, a learning effect might have taken place as the operators become used to the anatomy over time. We have not yet tested custom-shaped catheters12 as this might also influence the operators’ technique. In our opinion, our model is well suited to compare the use of custom-shaped catheters with standard shapes. Furthermore, our method could not be externally validated owing to the absence of a ’gold standard' with which to compare it. Nevertheless, data validation is required and should be performed in future studies.
Conclusion
We developed a new method to objectively characterize microcatheter tip behavior in vitro. With this method, we quantified the association of positional accuracy and precision according to the microcatheter tip shape and the operators’ experience. The method thus has potential for gathering evidence to guide microcatheter tip selection and might also be useful for training. In our small cohort, selection of a 45° tip microcatheter resulted in the highest average precision and accuracy. Assessment of more aneurysms and catheters as well as clinical validation are required.
Acknowledgments
The authors thank Philips Healthcare for the support and realization of the ’Hermann Zeumer Research Laboratory', including a Philips AlluraClarity angiography system.
References
Footnotes
Contributors Conception/design of work – AMF, JHB. Data collection – AMF, JHB. Data analysis and interpretation – JHB, AMF, JF. Drafting the article – AMF. Critical revision of the article – SG, JS, JHB, AMF, JF. Final approval of the version to be published – JHB, AMF, JF. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved – SG, JS, JHB, AMF, JF.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.