Article Text

Abstract
Background Tigertriever (Rapid Medical, Yoqneam, Israel) is a new design of stent retriever.
Purpose To evaluate the feasibility, safety, and efficacy of the Tigertriever in patients with acute ischemic stroke who have undergone mechanical thrombectomy.
Materials and methods Two different techniques—namely, standard unsheathing (SUT) and repetitive inflation-deflation (RID) techniques, were used. Modified Thrombolysis in Cerebral Infarction (mTICI) scores of 2b and 3 were considered as successful recanalization.
Results A total of 61 thrombectomy procedures with Tigertriever were retrospectively evaluated. The mean age of patients was 60.7 years and their National Institutes of Health Stroke Scale score was 14.7. Overall, the percentage of patients with a mTICI score of 0, 2b, and 3 was 24.6, 26.2, and 49.2, respectively. Successful recanalization and first-pass success rates were 75.4% and 37.7%, respectively. There were no statistical differences between the results of the SUT and RID techniques. No vessel rupture, dissection, or device detachment was observed. The number of patients with a good clinical outcome (modified Rankin Scale score 0–2) was 17 (27.9%).
Conclusion Our results showed that the Tigertriever device is safe and efficient for mechanical thrombectomy.
- stroke
- thrombectomy
Statistics from Altmetric.com
Introduction
Following the MR CLEAN study, the endovascular recanalization of large vessel occlusions (LVOs) has gained a crucially important position in the treatment of acute ischemic stroke.1 This, and further trials, have led to the introduction of mechanical thrombectomy using stent retriever devices in addition to intravenous thrombolysis as the recommended treatment for acute ischemic stroke in patients with LVO of the anterior circulation based on class I level A evidence.2 However, the extent of revascularization is still not 100%, being in the range 58.7–88% in different trials.1–6 Among several factors, such as the neurointerventionalist’s experience and use of different techniques, the technical properties of thrombectomy devices may also contribute to the angiographic results. Therefore, a variety of devices have been developed by the manufacturers. The Tigertriever (Rapid Medical, Yoqneam, Israel) is a new design of stent retriever comprising a collapsible, fully retrievable, fine-wire braided construction mounted on a wire shaft that expands to conform to the vessel diameter.7 The aim of this study is to report single-center results in patients with acute ischemic stroke who had undergone mechanical thrombectomy using the Tigertriever device.
Material and methods
Between February 2016 and December 2017, 61 patients with acute ischemic stroke who underwent mechanical thrombectomy using the Tigertriever device were evaluated retrospectively.
The device
The Tigertriever (Rapid Medical, Yoqneam, Israel) is a new design of stent retriever. After unsheathing the device from the delivery microcatheter, it is expanded by pulling a core wire, which is connected to the distal end of the mesh. The proximal end of the core wire is connected to a slider in the handle, which is pulled by the operator (figure 1). This mechanism makes the device adjustable so that after the device is unsheathed from the delivery microcatheter, the physician can expand and contract the mesh to conform to the diameter of the affected vessel. Because the wires of the mesh are completely radiopaque, the device can be seen in its entirety under fluoroscopy. Two versions of the device are available. The standard version (Tigertriever) has a net length of 32 mm (unexpanded form) and can expand up to 6 mm. It is delivered through a microcatheter with an internal diameter of 0.021 inches. A shorter version (Tigertriever 17) has a net length of 23 mm (unexpanded form) and it is delivered through a microcatheter with an internal diameter of 0.017 inches. It can expand up to 3 mm.
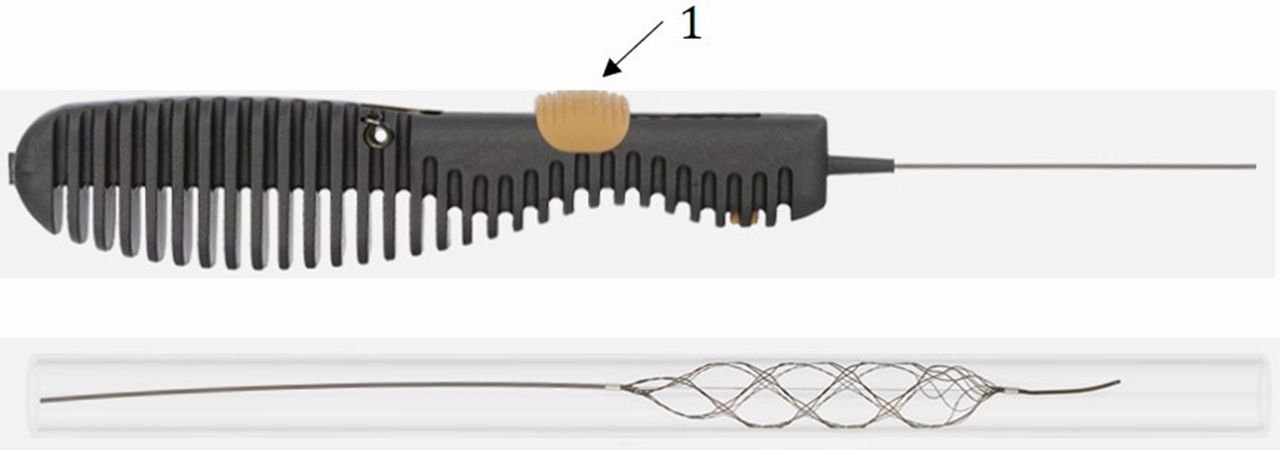
Tigertriever revascularization device with integrated handle slider (1).
Patient selection
The decision about endovascular treatment for each individual patient with anterior circulation ischemic stroke was based on the patient selection criteria of the MR CLEAN study. Inclusion criteria for patients with posterior circulation stroke were as follows: (1) clinical findings consistent with posterior circulation ischemic stroke; (2) durations of symptoms <48 hours; (3) National Institutes of Health Stroke Scale (NIHSS) score >5; (4) exclusion of hemorrhage on cranial CT or MRI; (5) basilar artery occlusion observed on CT angiography or MR angiography. Written consent was received from all patients or their relatives. The patients who were eligible for intravenous thrombolysis were treated with IV recombinant tissue-type plasminogen activator (rtPA) before the endovascular procedure. On admission of the patient, neurologists evaluated the NIHSS score. The modified Rankin Scale (mRS) score was assessed by an experienced stroke neurologist at 90 days after treatment. CT and intracranial CT angiography or diffusion-weighted MRI and intracranial MR angiography were performed immediately after neurological examination. Control CT and/or MRI scans were acquired 24 hours after treatment or when the patient’s symptoms worsened.
Endovascular procedure
All procedures were performed on a biplane flat-panel digital subtraction angiography unit (Allura FD 20×20, Philips Healthcare, The Netherlands). A 6F introducer was placed in the right femoral artery and diagnostic runs were obtained using a 5F catheter. After demonstrating the occlusion of the target vessel, the 5F diagnostic catheter was exchanged for a 6F guiding catheter over a 0.035 inch exchange guidewire. The guiding catheter was placed either in the proximal internal carotid artery (ICA) or in the vertebral artery, according to the circulation affected. The occluded segment was bypassed with a Vasco 10 (in middle cerebral artery (MCA) M2 occlusions) or a Vasco 21 (in an ICA terminus, MCA M1, and basilar artery occlusions) catheter (Balt, Montmorency, France) over a 0.014 inch Hybrid microguidewire (Balt, Montmorency, France). The position of the microcatheter was then verified with contrast medium passed through it. In the ICA terminus, MCA M1, and basilar artery occlusions, a standard version of the device was used. For MCA M2 occlusions, Tigertriever 17 was chosen.
After advancing the Tigertriever device through the microcatheter into the occluded segment, two different techniques were used. In the standard unsheathing technique (SUT), the Tigertriever was unsheathed by pulling back on the microcatheter while keeping the delivery wire of the device steady. It was then carefully opened under roadmap guidance so that the stent was apposed to the walls of the affected artery (figure 2). After waiting 4 min, the Tigertriever device was minimally or partially deflated and slowly withdrawn with the microcatheter as a unit. Alternatively, the so-called repetitive inflation–deflation (RID) technique was used in 23 patients. In this technique, the Tigertriever was placed so that the proximal one-third of the device covered the proximal part of the clot after unsheathing. Then, it was gently inflated and deflated about 20 times and finally, retrieved as in the standard unsheathing technique (online supplementary Multimedia 1). Neither a balloon-guiding catheter (BGC) nor aspiration during device retrieval was used with either of the techniques.
Supplementary file 1

An example of standard unsheathing. DSA shows occlusion of the left middle cerebral artery M1 segment (A). Control injection immediately after unsheathing and inflation of the device demonstrates partial recanalization of the occlusion (B). The final angiogram after retrieval of the device depicts complete recanalization (C).
When we started using the Tigertriever we used only the SUT as this was recommended. After gaining experience of using it, we thought that cases that ended with unsuccessful recanalization might be related to poor clot–stent interaction secondary to incomplete dilatation of the device in the thrombus (ie, <50% of the affected vessel’s diameter). To overcome this, we started using the device in a similar way to a balloon catheter with repetitive inflation–deflation, which resulted in better clot capture. After seeing that the RID technique was successful in cases in which SUT did not succeed, we used only the RID technique. The cases that led to the development of the RID technique are not included in this study. These cases were initially treated with SUT and including them would have resulted in statistical bias when comparing the two techniques.
There were no selection criteria for the type of stent retriever (ie, Tigertriever vs other stent retrievers). If an indication for mechanical thrombectomy was established, the operators were free to select any of the available devices. But if Tigertriever was chosen, it was used for three attempts to achieve recanalization. If this was unsuccessful after three attempts with the Tigertriever, then we used other stent retrievers. These included Solitaire (Covidien, Irvine, California, USA), Revive SE (Codman Neuro/DePuy Synthes, Johnson and Johnson Raynham, Massachusetts, USA), or Catch (Balt, Montmorency, France) devices as a rescue thrombectomy in three additional attempts. Only the thrombectomy procedures initiated with the use of Tigertriever device have been included in this study.
The success of treatment was evaluated according to the modified Thrombolysis in Cerebral Infarction (mTICI) score.8 The operator who performed the procedure reported the mTICI scores. Scores of 2b and 3 were considered as successful recanalization.
The type of anesthesia was determined based on the presence or absence of comorbidities, NIHSS scores, and cooperation of the patient. Patients with serious comorbidities, higher NIHSS scores, and low levels of cooperation were treated under general anesthesia.
Intravenous rtPA (full dose 0.9 mg/kg) was administered as a bridging therapy in patients eligible for IV thrombolysis. Ten percent of the full dose was given as the loading dose in these patients.
Statistical analysis
Recanalization rates, number of attempts, and first-pass rate were calculated according to the anatomical site of occlusion in both groups. Statistical comparison of overall recanalization rates between the SUT and RID technique was done with a X2 test The statistical differences of recanalization rates according to occlusion sites were evaluated with a Fisher-exact test. P values <0.05 were considered to be statistically significant.
The local Institutional review boards approved this study.
Results
A total of 61 thrombectomy procedures with a Tigertriever device were retrospectively evaluated (35 men, 26 women).
Overall results (whole cohort)
The age of the 61 patients ranged between 25 and 84 years (mean 60.7 years). The mean NIHSS score was 14.7 (range 5–30). Seventeen patients received IV rtPA (27.9%). Thirty-three patients (54%) were treated under general anesthesia, whereas 28 patients (46%) had local anesthesia. The percentage of patients with mTICI score of 0, 2b, and 3 was 24.6, 26.2, and 49.2, respectively. No patients had mTICI scores of 1 or 2a. The rate of successful recanalization (mTICI 2b–3) was 75.4% (46/61) (online supplementary Table 1). Successful recanalization at the first attempt was achieved in 37.7% of patients (23/61).
No vessel rupture, dissection or device detachment was observed during retrieval. A mild vasospasm was observed in eight patients (13.1%), which did not require further intervention.
We observed a distal embolus in only one patient.
In our series, 10 deaths occurred within 3 months after the procedure. No death was related to the procedure. Seven of 10 deaths occurred in non-recanalized patients, whereas the other three occurred in recanalized patients. Four deaths were related to pulmonary complications, two due to multisystem organ failure, and two due to cardiac failure. In the other two cases, massive intraparenchymal hematomas led to death. These were thought to be unrelated to the procedure or device, since the CT scan at 24 hours showed no hemorrhage but on the second day after procedure hematomas were seen. Both these patients received a bolus of IV rtPA before the procedure and were treated with SUT.
The mean 3-month postprocedure mRS score was 2.9. The number of patients with a good clinical outcome (mRS score 0–2) was 17 (27.9%).
Standard unsheathing technique results (SUT cohort)
Thirty-eight patients (16 female, 22 male) were treated with this technique. The age of patients varied between 25 and 83 years (mean 59.5 years). The mean NIHSS score was 14.7 (range 5–30). Ten patients received IV rtPA (26.3%). Seventeen patients (45%) were treated under general anesthesia, whereas 21 patients (55%) had local anesthesia. Successful recanalization rate was 71% (27/38). A successful recanalization at first attempt was achieved in 12 patients (31.6%). The recanalization rates, first-pass rates, and mean number of attempts in recanalized patients according to the sites of occlusions are summarized in online supplementary Table 2.
Mean time from stroke onset-to-groin puncture, time from groin puncture-to-recanalization, and time from stroke onset-to-recanalization in recanalized patients was 218.1 min, 38.5 min, and 257 min, respectively.
The mean mRS score at the third month was 3.1. The number of patients with a good clinical outcome (mRS score 0–2) was 10 (26.3%).
Repeated inflation–deflation results (RID cohort)
Twenty-three patients (9 female, 14 male) were treated with this technique. The mean age was 62.2 years (range 36–84 years). The NIHSS scores ranged between 5 and 24 (mean 14.8). Seven patients (30%) received IV rtPA. Fifteen patients (65%) were treated under general anesthesia, whereas eight patients (35%) had local anesthesia. Successful recanalization rate was 82.6% (19/23). A successful recanalization at first attempt was achieved in 11 patients (47.8%). The recanalization rates, first-pass rates, and mean number of attempts according to the sites of occlusions are given in online supplementary Table 3.
Mean time from stroke onset-to-groin puncture, time from groin puncture-to-recanalization and time from stroke onset-to-recanalization in recanalized patients was 123.92 min, 43.42 min, and 219.53 min, respectively.
The mean mRS score at the third month was 2.6. The number of patients with a good clinical outcome (mRS 0–2) was 7 (30.4%).
Statistical analysis results
Although the mTICI scores of 2b and 3 were higher with the RID technique, analysis showed that there were no statistical differences between SUT and RID techniques (p=0.31). There were also no statistically significant differences between the two techniques for the sites of occlusions. P values for ICA terminus, MCA M1, MCA M2, and basilar artery occlusions were found to be 0.60, 0.66, 0.57, and 0.72, respectively. Statistical analyses are summarized in online supplementary Table 4.
Discussion
Following the MR CLEAN study, mechanical thrombectomy became a cornerstone in the treatment of acute stroke caused by LVO.1–5 7 In this study we retrospectively evaluated our results with the Tigertriever device in LVOs. Former randomized trials studying the efficacy of endovascular treatment of acute anterior circulation strokes due to LVOs achieved recanalization rates of between 58.7% and 88%. Although our study was retrospective and single arm, we think that our results with the Tigertriever device are comparable to those of former trials, as we achieved an overall rate of successful recanalization of 75.4% and the successful recanalization rates of SUT and RID techniques were 71% and 82.6%, respectively.
The Tigertriever thrombectomy device provides several technical advantages during the thrombectomy procedure. First, after unsheathing the device it does not open immediately as with self-expandable stent retrievers. As long as the operator does not expand the device it can be manipulated for correct positioning, which makes deployment of the device easier and more accurate. Second, the visibility of the Tigertriever can give the operator an indication of stent–clot integration and clot features. In most of the unsuccessful cases we observed that the middle segment of the stent was unable to expand (even if we oversized it), while proximal and distal parts of the stent had a very good vessel wall apposition, giving the device a bow-tie configuration (figure 3). We postulate that the clots in these failed cases had a very firm segment in the middle where the stent could not expand but also had softer parts proximal and distal to it. This central core of the clot was thought to be resistant to thrombectomy and responsible for failed recanalization. In failed Tigertriever cases, we used other conventional thrombectomy devices as the rescue thrombectomy, but none were successful. Therefore, we think that if a bow-tie configuration is seen after proper localization and oversizing the Tigertriever, then the clot should be considered to be resistant to stent retriever thrombectomy. In this case aspiration thrombectomy (alone or combined with a stent retriever) should be performed as the rescue thrombectomy, since our attempts at rescue thrombectomy with other devices failed, in those cases where the Tigertriever was unable to expand and capture the thrombus.

{kind=link}
{kind=link}
{kind=link}
Control injection immediately after unsheathing and inflation of the device shows partial recanalization of the left middle cerebral artery M1 occlusion (A). Owing to a firm clot, the device cannot expand its middle segment. Proximal and distal parts of the stent have very good vessel wall apposition, giving the device a bow-tie configuration (B). The final angiogram depicts failed recanalization (C). Multimedia 1: The movie shows a successful recanalization of the right internal carotid artery terminus occlusion using the repetitive inflation–deflation technique (see online supplementary media 1).
Although not statistically significant, we encountered fewer attempts and higher recanalization rates when the RID technique was used compared with SUT. The study of Haussen et al provides a plausible explanation for this.9 They developed a new technique, in which they maximized expansion of the Trevo 2 (Stryker Neurovascular) device by applying forward tension to the microcatheter while the delivery wire continued to be pushed during deployment of the stent retriever in the affected segment. With this so-called ‘push and fluff’ technique, they achieved better results than with SUT. They proposed that this method enabled increased radial force, better wall apposition, enlarged cell size, and optimized cell configuration, leading to better clot–stent interaction. We think that the RID and push and fluff techniques share similar mechanisms. By pulling the slider gradually, the diameter of the device increases and oversizing the device causes more enlargement of cells, so more clot fragments may prolapse into the stent lumen. The oversizing also causes better apposition of the stent to the vessel wall, which enhances stent–clot interaction. Additionally, the oversizing can be controlled, as necessary, without any pushing or pulling of the device.
Beside embolic occlusions, underlying intracranial atherosclerotic stenosis (ICAS) and in situ thrombo-occlusions are responsible for LVO seen in patients with stroke. A French study showed that patients with underlying ICAS accounted for 5.5% of patients who underwent mechanical thrombectomy.10 Underlying ICAS appears to be more common in Asian countries; a Korean study reported that around 15% of ICAS-related occlusions are found in the anterior circulation.11 Another Korean study demonstrated that ICAS-related occlusion was found in approximately 35% patients with vertebrobasilar artery occlusion.12 However, conventional thrombectomy devices are primarily designed for recanalization of the occluded artery by removing an embolus, and recanalization may not be sufficiently achieved if a significant stenosis, related to intracranial atherosclerosis, is present at the occlusion site. When using the RID technique, the Tigertriever device may have an advantage over other conventional mechanical thrombectomy devices in those cases with in situ thrombo-occlusion. Since the RID technique has an effect on the vessel wall similar to that seen in balloon angioplasty, it is possible to catch the clot and dilate the underlying narrowing at the same time in those patients.
Another interesting observation was that a very low percentage of distal emboli enter previously unaffected territories, although we did not use a balloon-guiding catheter and aspiration during device retrieval. We experienced it only in one patient. There may be two reasons for this. First, most of the patients in our series did not receive IV rtPA. There is a growing concern among neurointerventionalists that giving rtPA may cause fragmentation of the clot, allowing emboli to enter previously unaffected territories. Therefore, some investigators prefer not to use it in candidates for mechanical thrombectomy.2 13 The second reason might be that the closed-mesh design and partial deflation of the device during retrieval enables firm entrapment and en bloc removal of the clot, preventing clot fragmentation and distal emboli if it is captured. We noticed that it was frequently difficult to wipe off the clot particles retained in the lumen of device.
This study has inherent limitations due to the retrospective design and the small number of patients. Another limitation is that we did not use BGC and aspiration during retrieval of the device in any of the cases. There is growing evidence that proximal flow arrest and aspiration may enhance recanalization rates.2 14 Unfortunately, we could not use either in our cohort as they were unavailable in our institution at that time. It is possible that higher recanalization and first-pass rates could be achieved if BGC was used. Additionally, our data are insufficient to reach a conclusion about the efficacy of the two techniques (ie, SUT vs RID) or for comparison of the Tigertriever device with conventional stent retrievers.
Conclusion
Tigertriever is a newly introduced device to the armamentarium of endovascular treatment of acute ischemic stroke. Our initial results showed that it is a safe and efficient device for mechanical thrombectomy. We did not experience any complications related to device during the procedures. Our initial findings indicate that the RID technique can enhance clot–stent integration in comparison with SUT. Considering the RID technique, a Tigertriever device may have an advantage over conventional stent retrievers with in situ thrombo-occlusions due to the underlying atherosclerotic stenosis, since it has an effect similar to that of balloon angioplasty. Multicenter randomized studies with a larger population are needed to determine the efficacy of this new device when combined with the RID technique.
Supplementary file 2
Supplementary file 3
Supplementary file 4
Supplementary file 5
Acknowledgments
We want to thank our devoted nurse Ms Aynur Mucuk for her efforts in the treatment of our patients.
References
Footnotes
B.K., H.H.S, AES, HZ, OY, GG and BB contributed equally.
Contributors BK contributed to the study design and manuscript writing. HHS was responsible for data analysis and manuscript writing. AE contributed to manuscript writing. HZ and OY collected the data. GG evaluated the neurological status of the patients at the third month. BB collected the data and contributed to data analysis.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Patient/guardian consent obtained.
Ethics approval Bakirkoy Dr Sadi Konuk Egitim ve Arastirma Hastanesi.
Provenance and peer review Not commissioned; externally peer reviewed.