Article Text

Abstract
Background The Woven EndoBridge (WEB) device is a novel endovascular tool for the treatment of wide-necked intracranial aneurysms.
Objective To evaluate factors influencing aneurysm occlusion and aneurysm recurrence after WEB embolization.
Methods A total of 113 patients (mean age 58.9±11.9 years) with 114 aneurysms (mean size 8.6±4.6 mm) were successfully treated with the WEB device at three German tertiary care centers between May 2011 and February 2018. Aneurysm occlusion was evaluated using the Raymond-Roy occlusion classification. We retrospectively collected patient characteristics, anatomical details, and procedural aspects and evaluated their impact on aneurysm occlusion and recurrence.
Results Of 98 patients available for a 6-month angiographic follow-up, complete occlusion was achieved in 62.2%, neck remnants in 21.4%, and aneurysm remnants in 16.3%. Aneurysm recurrence occurred in 15.3%. Initial partial aneurysm thrombosis, recurrent aneurysms, aneurysm size, and simultaneous treatment by WEB and coil were associated with aneurysm remnants (p<0.05). Initial partial aneurysm thrombosis, increasing aneurysm size, and treatment by WEB and coil also predicted aneurysm recurrence (p<0.05).
In the subgroup analysis of 71 aneurysms treated with WEB only, initial incomplete occlusion and male sex were associated with aneurysm remnants (p<0.05), while aneurysm height correlated with aneurysm recurrence (p=0.008).
Conclusions The WEB provides a high rate of adequate occlusion even in a subset of complex wide-necked intracranial aneurysms. Anatomic results tend to be less favourable in large and partially thrombosed aneurysms and after treatment with WEB and coil.
- aneurysm
- coil
- device
- intervention
Statistics from Altmetric.com
Introduction
The Woven EndoBridge device (WEB, Sequent Medical, Aliso Viejo, California, USA) is an intra-aneurysmal flow disruptor that has been designed for the treatment of wide-necked and bifurcation aneurysms, which are typically challenging to treat by endovascular means.1–3 The WEB is placed within the aneurysm sac where it seals the aneurysm neck leaving the parent artery unaffected.4 Hence, long-term antiplatelet therapy is not crucial and the WEB can be used for the treatment of both unruptured and ruptured aneurysms.5–8
Since its introduction in 2011, the safety and efficacy of the WEB has been evaluated by several multicenter studies.6 9 Mid-term adequate occlusion rates in Good Clinical Practice trials have been shown to exceed those of conventional coiling or stent-assisted coiling in similar subsets of aneurysms.9 However, aneurysm recurrence may occur.10 Furthermore, it is not yet fully understood which aneurysms are more likely to recanalize. Recently, Limbucci et al identified large neck width as a potential risk factor for inadequate occlusion after treatment of unruptured aneurysms with the WEB in a single-center series of 24 patients.11 Owing to the novelty of the WEB, further risk factors for aneurysm recurrence determined by a larger series are not available.
The objective of this multicenter study was to analyze retrospectively mid-term occlusion rates after WEB implantation and to identify potential factors that influence aneurysm occlusion and recurrence.
Methods
A retrospective, observational study of consecutive patients who underwent the WEB procedure at three German high-volume neurovascular centers between May 2011 and February 2018 was carried out. All patients with successful WEB embolization of the target aneurysm were included in this study. Some of the data have been previously reported in two articles that focused on the use of WEB for large, partially thrombosed aneurysms, and on re-treatment strategies after WEB implantation, respectively.12 13 According to the institutional guidelines, ethics committee approval was not required owing to the retrospective nature of this observational study.
Data collection
The following data were obtained from the medical records: patient age, sex, aneurysm rupture status, aneurysm location, previous aneurysm treatment, WEB type, and use of additional devices or coiling.
Baseline aneurysm characteristics were evaluated by conventional four-vessel digital subtraction angiography (DSA) with three-dimensional reconstructions of rotational angiography datasets. Aneurysm width, height, and neck width were determined for all aneurysms. The dome-to-neck (D/N) ratio, aspect ratio, and width-to-height (W/H) ratio were calculated. An aneurysm was considered to be wide-necked, when the neck width was >4 mm and/or the D/N ratio was up to 2. The presence of initial, pre-existing intrasaccular aneurysm thrombosis was determined based on CT angiography and DSA. Aneurysm shape was determined using volume-rendered images of 3D rotational angiography datasets. Lobular shape was defined as the presence of an additional aneurysm sac next to the main aneurysm sac.
Functional outcome was evaluated by the modified Rankin scale (mRS) score at the 6-month follow-up. Unfavorable outcome was defined as mRS score >2.
WEB treatment
All procedures were performed via a transfemoral approach with the patient under general anesthesia in a biplane angiosuite (Philips, Best, the Netherlands and Siemens, Erlangen, Germany). In the majority of cases, the WEB was delivered through the dedicated VIA microcatheter (VIA 21, 27, or 33, Sequent Medical, Aliso Viejo, California, USA).
At our institutions we used the single-layer (SL), double-layer (DL), and single-layer sphere (SLS) WEBs. The appropriate WEB size was selected according to the aneurysm width and height as measured on two-dimensional DSA images. Implant sizes were chosen to be slightly larger than the aneurysm equator diameter as recommended in the instructions for use. The use of additional devices was left to the neurointerventionalist’s discretion. If optimal placement of the WEB within the aneurysm sac could not be guaranteed and WEB protrusion was expected, a stent was implanted for prevention. In some aneurysms with atypical configuration for the WEB, additional coiling was performed in a single session in order to provide adequate occlusion of the aneurysm. Aneurysms that were pretreated by coiling or another modality were subsumed as recurrent aneurysms. We also included large aneurysms, in which the WEB was used as part of a multimodal treatment approach. These aneurysms exceeded the largest available WEB, and are also difficult to treat by other modalities. If multiple devices were used, the WEB was used to seal the aneurysm neck off from the parent vessel in all cases.
Anti-aggregation therapy
A bolus of heparin (5000 IU) was administered after groin puncture, followed by aliquots of 1000 IU/h. Heparin was discontinued at the end of the procedure. For WEB implantation, all patients received acetylsalicylic acid (ASA) 100 mg/day starting 5–7 days before the procedure, and ASA monotherapy was continued for a minimum of 4 weeks. In cases of additional stent implantation or flow diversion, a daily dual antiplatelet regimen with ASA 100 mg and clopidogrel 75 mg was administered for at least 4 months after the intervention, starting 5–7 days before the procedure. Thereafter, ASA monotherapy was continued. Platelet inhibition was tested in all patients with ASA and additionally, P2Y12 assays where required (VerifyNow, Accumetric, San Diego, California, USA). A platelet inhibition level of 350–550 aspirin response units and 30–90% for clopidogrel was required. An insufficient response to either drug was counteracted by dose escalation (eg, clopidogrel 150 mg/day) or substitution with prasugrel (60 mg bolus, 10 mg/day).
Angiographic control and re-treatment
Angiographic follow-up was routinely performed 6 and 24 months after the procedure by DSA, magnetic resonance angiography, or CT angiography.
Aneurysm occlusion was evaluated immediately at the end of the procedure and at follow-up imaging using the Raymond-Roy occlusion classification (RROC): 1, complete occlusion, 2, neck remnant, 3, aneurysm remnant. Complete occlusion and neck remnants were considered as adequate occlusion.
Independent of aneurysm occlusion, aneurysm recurrence was defined as any increase on the RROC scale at the 6- month angiographic follow-up in comparison with immediate angiographic results after WEB deployment (ie, from RROC 1 to RROC 2 or 3, or from RROC 2 to RROC 3). RROC 2 was considered a minor recurrence, while RROC 3 was defined as a major recurrence.
In cases of incomplete aneurysm occlusion at follow-up, the decision for re-treatment was made by consensus during a neurovascular conference among neurointerventionalists and neurosurgeons. The endovascular re-treatment method was left to the discretion of the operator.
Statistical analysis
Categorical variables are presented as numbers and percentages and groups were compared using the χ2 and Fisher’s exact test, as appropriate. Continuous variables are presented as mean and SD and compared using the two-sided unpaired t-test. Patient age, sex, ruptured aneurysm status, aneurysm recurrence, aneurysm location, aneurysm size, aneurysm morphology, additional coiling, use of additional devices, WEB type, and initial incomplete occlusion were considered as factors potentially influencing immediate aneurysm occlusion, aneurysm occlusion at the 6-month follow-up, and aneurysm recurrence. Factors predictive in the univariate analysis (p<0.05) were entered into a binary logistic regression model to identify independent factors for these outcome measures. Statistical analysis was performed using SPSS software (IBM SPSS Statistics for Windows, Version 25.0, Armonk, New York, USA). A p value <0.05 was considered as statistically significant.
Results
Patient and aneurysm characteristics
A total of 121 patients (mean age: 58.5±11.9 years, 81 female) with 122 aneurysms were treated with the WEB device within the study period. After exclusion of eight aneurysms (6.6%), in which WEB implantation failed, the study cohort consisted of 113 patients with 114 aneurysms. The mean patient age was 58.9±11.9 years and 75 patients (66.4%) were female. Thirty-six patients (36/114 (31.6%) aneurysms) were treated for a ruptured aneurysm during the acute phase of subarachnoid haemorrhage (within 24 hours after ictus). Ten patients had recurrent aneurysms (8.8%) that were previously treated with other modalities. Seven aneurysms (6.1%) were partially thrombosed and 13 (11.4%) had a lobular shape. The majority of aneurysms were located at the basilar tip (34.2%), the anterior communicating artery (28.1%), and the middle cerebral artery bifurcation (14.0%). Ninety-one (79.8%) aneurysms were located at a bifurcation, and 23 (20.2%) were sidewall aneurysms. The maximum aneurysm diameter ranged from 3 to 27.2 mm (mean diameter 8.6±4.6 mm). The mean dome width was 7.3±3.6 mm, the mean aneurysm height 7.9±4.4 mm, the mean neck width 4.6±1.8 mm, and the mean D/N ratio 1.7±0.8. A total of 104 aneurysms (91.2%) were classified as wide-necked. Baseline patient and aneurysm characteristics are presented in table 1.
Baseline patient and aneurysm characteristics
Procedural details
Procedural details of the WEB treatment are summarized in table 2. Eighty-eight aneurysms were treated by WEB only (77.2%) and 26 aneurysms (22.8%) were treated in conjunction with coiling or additional devices (stents or flow diverters). For these, additional stents were used for 16 aneurysms, additional flow diverters for three, and one complex aneurysm was treated in conjunction with stenting and flow diversion. Additional coiling was performed in 11 patients (9.6%), and in these cases ancillary stents were used for five aneurysms (4.4%).
Initial treatment strategies and immediate angiographic results
Immediate complete aneurysm occlusion after WEB placement was obtained in 65 aneurysms (57.0%), neck remnants in 22 (19.3%) and aneurysm remnants in 27 (23.7%). We did not identify any significant factors that were predictive for immediate aneurysm occlusion in the univariate analysis (data not shown).
Clinical outcome
At the 6-month clinical follow-up, 92 of 113 patients (81.4%) attained favourable outcome (mRS score ≤2) and three deaths occurred, of which one was procedure related. Favourable outcome was achieved by 75 of 78 patients (96.2%) in the subgroup with unruptured aneurysms and 17 of 35 patients (48.6%) in the subgroup with ruptured aneurysms. In patients with ruptured aneurysms, unfavourable outcome was procedure related in one case (2.9%) and related to subarachnoid haemorrhage itself in the remaining patients.
Angiographic outcome
A total of 98 aneurysms (86.0%) were available for the 6-month angiographic follow-up. Complete aneurysm occlusion was achieved in 61 cases (62.2%), neck remnants in 21 (21.4%) and aneurysm remnants in 16 (16.3%). Hence, adequate occlusion was obtained in 83.7%.
The results of the univariate analysis for aneurysm occlusion are given in table 3. Patient demographics, ruptured aneurysm status, and aneurysm location were not significantly associated with aneurysm occlusion. Adequate occlusion was obtained in two of six thrombosed aneurysms (33.3%) and in 87% of non-thrombosed aneurysms (p=0.004). Similarly, four of 8 recurrent aneurysms (50.0%) showed adequate occlusion, compared with 86.7% in the remaining population (p=0.023). The mean maximum aneurysm diameter of adequately and inadequately occluded aneurysms was 8.0±3.4 mm and 13.3±8.0 mm, respectively (p=0.019). Aneurysms treated by a combination of WEB and coils carried an increased risk of inadequate occlusion (50.0%, p=0.002), whereas treatment with WEB only was associated with a low rate of aneurysm remnants (p=0.026). In the multivariate analysis, aneurysm size (OR=1.2, 95% CI 1.01 to 1.38; p=0.034) was an independent morphological risk factor for aneurysm remnants. Among the procedure-related factors, recurrent aneurysms (OR=7.5, 95% CI 1.5 to 37.3; p=0.013) and treatment by WEB and coiling (OR=7.9, 95% CI 1.8 to 33.9; p=0.005) were independently associated with aneurysm remnants.
Factors influencing aneurysm occlusion
For the subgroup analysis of aneurysms treated with WEB only, we excluded aneurysms treated simultaneously by WEB and coiling, WEB and other devices as well as recurrent aneurysms that had been previously treated by another modality. Complete occlusion was achieved in 48 of 71 aneurysms (67.6%), neck remnants in 16 (22.5%) and aneurysm remnants in 7 (9.9%). The rate of adequate aneurysm occlusion was 90.1%. Aneurysm remnants were more often observed in male patients (21.9%) than in female patients (0%, p=0.003). Moreover, the rate of adequate occlusion in patients with immediate complete aneurysm occlusion (100%) was significantly higher than in patients with incomplete aneurysm occlusion after deployment (78.1%; p=0.003) (table 3). In the multivariate analysis, none of these factors remained significant.
In the overall study population, aneurysm recurrence (ie, increase on the RROC scale at the 6-month follow-up) occurred in 15 cases (15.3%). Of these, seven aneurysms presented with minor recurrence (RROC 2) and eight aneurysms with major recurrence (RROC 3).
Factors influencing aneurysm recurrence are evaluated in table 4. Recurrence was significantly associated with partial intrasaccular thrombosis (p<0.001), increasing aneurysm size (p=0.005), and additional coiling (p=0.001). In the multivariate analysis, aneurysm size (OR=1.2, 95% CI 1.02 to 1.41; p=0.032) and additional coiling (OR=7.8, 95% CI 1.9 to 31.7; p=0.004) remained as independent predictors of recurrence.
Factors influencing aneurysm recurrence
In the subgroup analysis of aneurysms treated with the WEB only, aneurysm recurrence was observed in 8 of 71 aneurysms (11.3%), including six minor recurrences and two major recurrences. Recurrent aneurysms had a larger aneurysm height (p=0.008) and aspect ratio (p=0.012) than aneurysms without recurrence. These factors were dependent in the multivariate analysis.
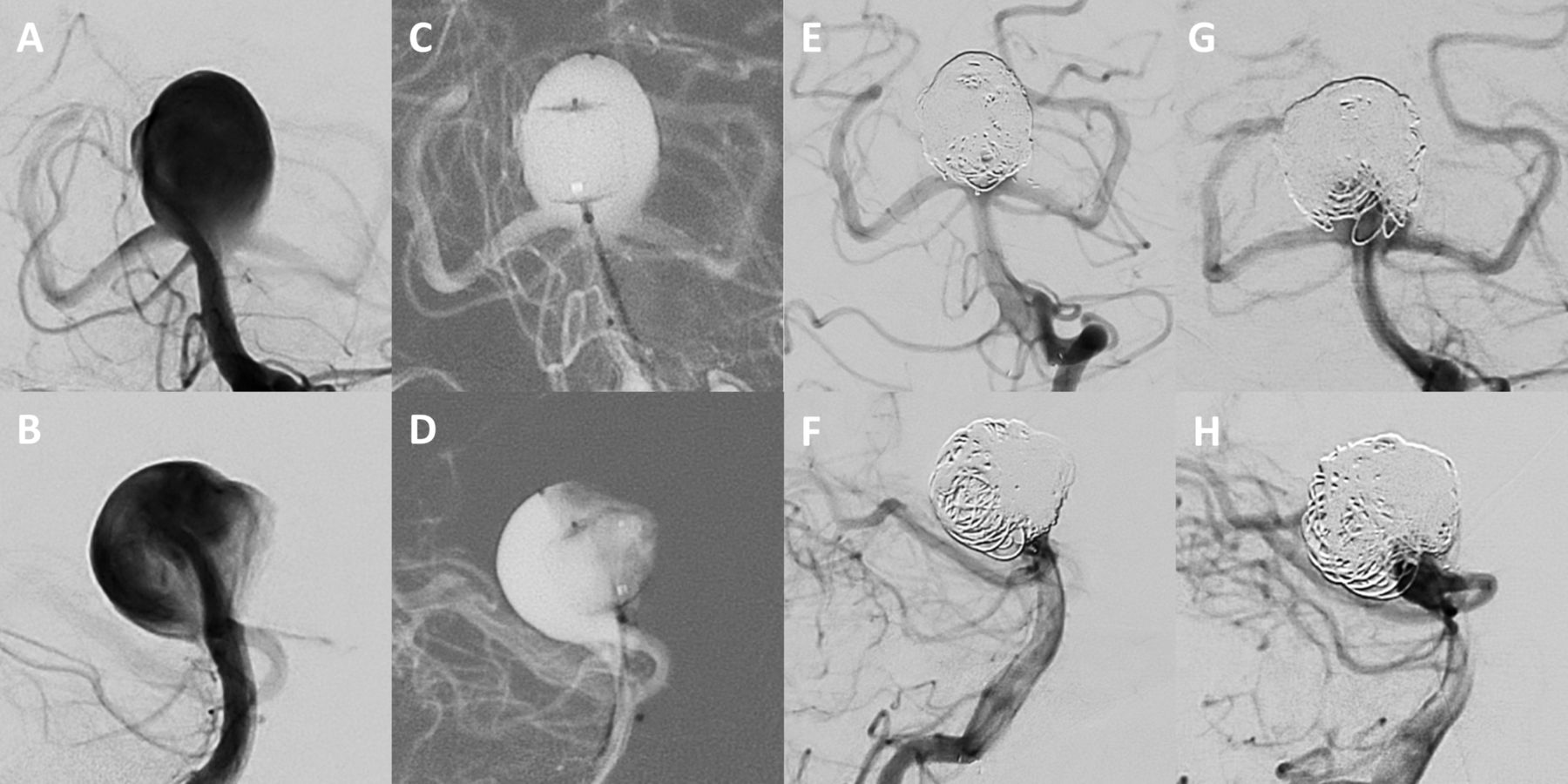
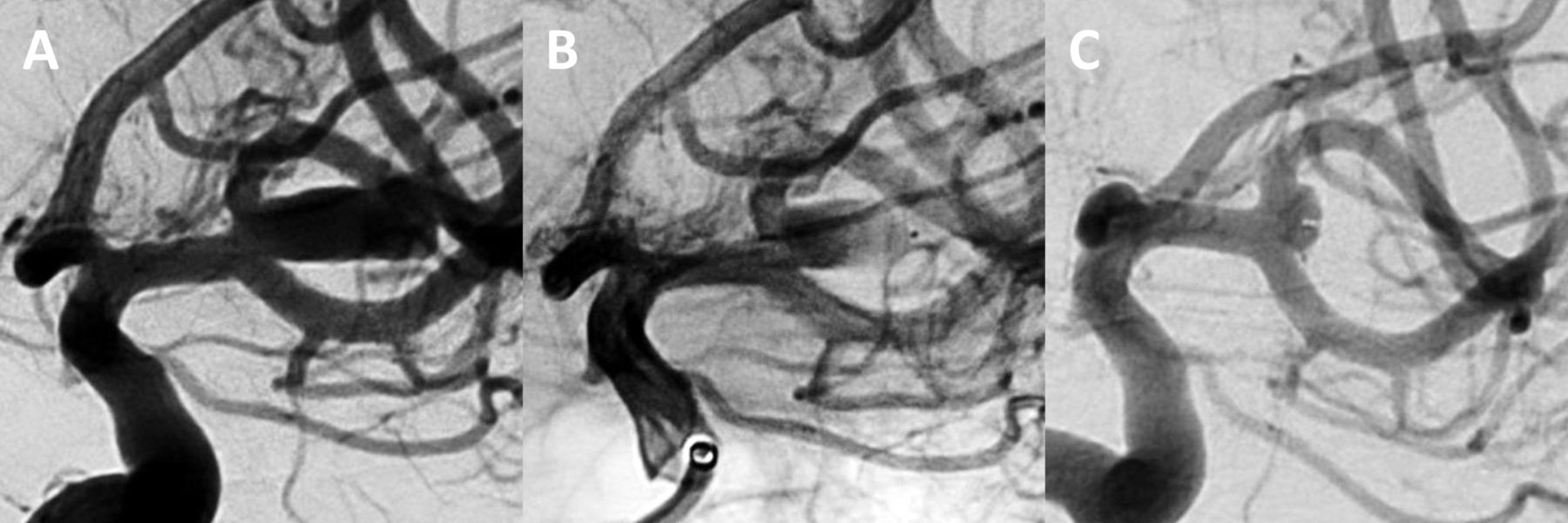
Figures 1 and 2 illustrate cases of a large aneurysm treated by WEB and coiling and an aneurysm treated by WEB only, respectively.

Digital subtraction angiography shows a large, unruptured aneurysm at the basilar tip (17×17 mm, neck width 10 mm) (A, B). Owing to the large neck width and irregular shape of the aneurysm, the WEB was used as part of a multimodal treatment approach for this aneurysm. After deployment of a WEB SL 11×8 mm (C, D), the WEB position was secured by additional implantation of coils and a Neuroform stent, achieving immediate complete aneurysm occlusion (E, F). After 6 months, angiographic follow-up shows a large aneurysm remnant (8×8 mm) due to coil compaction and subsequent migration of the WEB into the aneurysm sac (G, H).

{kind=link}
{kind=link}
A patient presented with an unruptured middle cerebral artery bifurcation aneurysm (12×6 mm). The aneurysm was treated by a WEB SL 6×4 mm, achieving complete sealing of the aneurysm neck and immediate contrast stasis within the aneurysm sac (B). Seven-month angiographic follow-up shows a neck remnant due to WEB compression, which did not require re-treatment (C).
Re-treatment
Fifteen aneurysms were re-treated after previous WEB implantation (15.3%). Re-treatment strategies included coiling in four patients, stent-assisted coiling in seven, flow diversion in three, and placement of an additional WEB in one. Re-treatment was feasible in all cases. No morbidity or mortality was associated with re-treatment.
Discussion
In this study we analyzed mid-term angiographic results after WEB implantation in a cohort of 113 patients with 114 aneurysms. We identified several risk factors that might interfere with aneurysm occlusion and result in aneurysm recurrence following WEB embolization. To the best of our knowledge, this is the first study to analyze factors that may determine incomplete aneurysm occlusion in a larger patient cohort.
Since the introduction of the WEB device in 2011, intrasaccular flow disruption has caused a fundamental change in the endovascular treatment of wide-necked and bifurcation aneurysms, which are otherwise difficult to treat by conventional endovascular means. In our series, the rates of complete and adequate aneurysm occlusion at the 6-month follow-up were 62.2% and 83.7%, respectively, which is within the range cited in the literature. A summary of aneurysm occlusion rates of previously published studies is provided in table 5. Aneurysm recurrence (defined as any increase on the RROC scale) occurred in 15.3%, including seven minor recurrences and eight major recurrences. These data collectively suggest the efficacy of the WEB for endovascular treatment of wide-necked bifurcation aneurysms. Moreover, the occlusion rates of the WEB compare favourably with conventional endovascular methods, which are associated with recurrence rates of approximately 25% at mid-term follow-up.14 15 Considering that the morphology of aneurysms typically treated by the WEB device is more complex than that of aneurysms treated by regular coiling, these occlusion rates appear promising.
Overview of published studies (≥30 included patients) that report aneurysm occlusion rates after Woven EndoBridge treatment
To date, only one published study has evaluated the potential risk factors for inadequate aneurysm occlusion at mid- and long-term follow-up. In their single-center analysis, Limbucci et al included 24 patients with 24 aneurysms, of whom 21 were treated by WEB only.11 The authors showed that large neck width and an unfavourable D/N ratio were potential risk factors of aneurysm remnants at follow-up. In our study we were unable to confirm this association of neck width and aneurysm occlusion, as reported by Limbucci et al.11 However, we found a significant association between aneurysm occlusion and initial partial aneurysm thrombosis, recurrent aneurysms, aneurysm size, and treatment by WEB and coil.
In our study, aneurysms treated by a combination of WEB and coiling carried a high risk of aneurysm recurrence. This becomes particularly evident in the treatment of large and also partially thrombosed aneurysms that exceeded the size of the largest available WEB and were treated in multimodal approach using coiling and other endovascular devices, as reported in a previous publication.12 These types of aneurysm are also exceptionally challenging to treat by either endovascular or surgical methods and, independent of the treatment strategy, they are known to carry a high risk of recurrence.16 17 Furthermore, large aneurysm size represents a significant risk factor for recanalization after conventional coiling and stent-assisted coiling.15 18 Conceding that these aneurysms do not represent the typical indication for WEB implantation, we expected that sealing the aneurysm neck with a WEB would minimize the risk of aneurysm recurrence, thus constituting an advantage over established coiling techniques. However, 50% of aneurysms treated by WEB and coil and 83.3% of partially thrombosed aneurysms recurred at the 6-month follow-up. In the majority of these cases, coil compaction within the aneurysm cavity, or migration of the coils into the intrasaccular thrombus, left a free space in the aneurysm sac. Therefore, the WEB was pushed distally into the aneurysm sac by the blood flow, leading to WEB device migration. Based on the results of our study, treatment of large and partially thrombosed aneurysms by WEB and coil was not associated with more favourable occlusion rates than the use of conventional coiling or stent-assisted coiling. Hence, the combined, extraordinary treatment of WEB and coil for large aneurysms that exceed the size of the largest available WEB should be carefully deliberated and this approach should be reserved for selected cases.
Since aneurysms with a size >11 mm do not represent the primary indication for WEB treatment, we performed a subgroup analysis of aneurysms, in which the WEB constituted the unique treatment. As expected, aneurysms treated by WEB only had a more favourable aneurysm occlusion than aneurysms treated by WEB and coil, achieving complete occlusion in 67.6% and adequate occlusion in 90.1%. In this subset of aneurysms, incomplete occlusion during device deployment, aneurysm height, and male sex were associated with aneurysm occlusion or recurrence.
Owing to its spherical shape and its shape memory, the WEB was initially expected to be less prone to compaction than coils. However, several studies described a phenomenon called ‘WEB compression’, which means a decrease in the height of the device due to the deepening of the device recesses at both sides, resulting in partial reperfusion of the sac.10 19 20 According to a recent study with core laboratory evaluation of anatomic results, modification of the WEB shape occurs in approximately 30% of cases and seems not to be related to WEB sizing.19 WEB compression can lead to aneurysm recurrence, mostly small neck remnants, which generally do not require re-treatment.19 Of eight recurrent aneurysms in the WEB only group, only two had a major recurrence, while the other six aneurysms showed minor recurrence as a consequence of WEB compression. Of note, aneurysm recurrence correlated positively with the height of the aneurysm. This may be explained by the fact that the compression effect is more pronounced in large-sized WEBs.
In this study, ruptured and unruptured aneurysms had similar occlusion rates. Therefore, the WEB may represent a promising alternative treatment during the acute phase of subarachnoid haemorrhage, since aneurysm rupture is an established risk factor for recurrence after coiling.15
In our study, seven aneurysms treated by WEB only had aneurysm remnants at follow-up. In all cases, immediate complete aneurysm occlusion could not be achieved during device deployment and thrombosis of the aneurysm neck was not sufficient after 6 months. These results demonstrate that immediate complete aneurysm occlusion should be targeted during WEB treatment. For this purpose, a slight oversizing of the WEB may prove beneficial, as also suggested by other authors.21
Male sex as potential factor influencing aneurysm occlusion is unknown related to WEB treatment, but has already been described for conventional coil embolization.22 The association between gender and aneurysm progression has not yet been studied in detail. However, the authors suggested that the increased estrogen levels in women would have a protective effect against progression of intracranial aneurysms. Since estrogen has a beneficial effect on the function of endothelial cells it might help to preserve the integrity of the vascular wall.23
Limitations
The limitations of this study are mainly related to its retrospective design. The aneurysms were heterogeneous in size and configuration and different treatment methods were used for aneurysm embolization. Although we conducted a multicenter analysis, the sample size was only moderate. Moreover, the angiographic results were bound to a 6-month follow-up period, and factors influencing long-term aneurysm occlusion remain unclear. In view of these limitations, further studies with a larger patient sample will be required to reach a definite conclusion. Nevertheless, we believe that our study provides valuable insight into the mechanism of aneurysm recurrence after WEB embolization.
Conclusions
In this study, we showed that occlusion rates after WEB implantation are strongly dependent on aneurysm size and morphology. Anatomic results may be less favourable in large and thrombosed aneurysms and after combined treatment with WEB and coil. Angiographic outcome was not associated with aneurysm rupture and aneurysm location. Further studies will be necessary to identify factors that influence long-term aneurysm occlusion.
References
Footnotes
CK and LG contributed equally.
Contributors CK, LG, ES, MH, JB, and FD acquired the data. CK, LG and TL developed the project, analyzed the data, and drafted the manuscript. All authors revised the paper critically for important intellectual content and provided final approval of the version published. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. CK and LG contributed equally as first authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests CK and FD serve as consultants for Acandis GmbH (Pforzheim, Germany). TL serves as proctor for MicroVention Inc./Sequent Medical (Aliso Viejo, California, USA).
Patient consent Not required.
Ethics approval According to institutional guidelines, no ethics committee approval was required for this retrospective observational study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data will be made available upon request in an anonymized manner.