Article Text

Abstract
Background and purpose Inter-hospital transfer for mechanical thrombectomy (MT) might result in the transfer of patients who finally will not undergo MT (ie, futile transfers [FT]). This study evaluated FT frequency in a primary stroke center (PSC) in a semi-rural area and at 156 km from the comprehensive stroke center (CSC).
Methodology Retrospective analysis of data collected in a 6-year prospective registry concerning patients admitted to our PSC within 4.5 hours of acute ischemic stroke (AIS) symptom onset, with MR angiography indicating the presence of large vessel occlusion (LVO) without large cerebral infarction (DWI-ASPECT ≥5), and selected for transfer to the CSC to undergo MT. Futile transfer rate and reasons were determined, and the relevant time measures recorded.
Results Among the 529 patients screened for MT, 278 (52.6%) were transferred to the CSC. Futile transfer rate was 45% (n=125/278) and the three main reasons for FT were: clinical improvement and reperfusion on MRI on arrival at the CSC (58.4% of FT); clinical worsening and/or infarct growth (16.8%); and longer than expected inter-hospital transfer time (11.2%). Predictive factors of FT due to clinical improvement/reperfusion on MRI could not be identified. Baseline higher NIHSS (21 vs 17; P=0.01) and lower DWI-ASPECT score (5 vs 7; P=0.001) were associated with FT due to clinical worsening/infarct growth on MRI.
Conclusions In our setting, 45% of transfers for MT were futile. None of the baseline factors could predict FT, but the initial symptom severity was associated with FT caused byclinical worsening/infarct growth.
- stroke
- thrombectomy
Statistics from Altmetric.com
Introduction
After demonstration of the clinical benefit of mechanical thrombectomy (MT),1–6 the focused update of the American Heart Association/American Stroke Association guidelines7 suggested that MT should be offered to patients with acute ischemic stroke (AIS) due to large artery occlusion (LVO) and a favorable imaging profile, and who can be treated within 6 hours of symptom onset. In 2018, this time window was extended for selected patients to 24 hours,8 after the positive results of the Dawn and Defuse 3 trials.9 10 Such guidelines also advocated the implementation of stroke networks7 to provide high-quality care for patients with stroke in settings with a distant comprehensive stroke center (CSC). To date, these stroke care networks have been implemented regionally to connect a CSC to primary stroke centers (PSC). This approach (the so-called drip-and-ship model) has been designed mainly to improve the rate and reduce the delay of intravenous thrombolysis (IVT) with recombinant tissue plasminogen activator (rtPA).However, it also plays an important role in the selection of patients eligible for MT. Patients may receive IVT at the PSC but IVT efficacy is limited in about 30% of patients with LVO.11 12 Thus, eligible patients require urgent transfer to CSC for consideration of MT. However, this approach might result in the transfer of patients who finally will not undergo MT (ie, futile transfer [FT]). In this study, we wanted to determine FT frequency and reasons in a PSC in a semi-rural area and far away from the CSC, and to identify potential FT predictors and associated factors.
Methodology
Geographical and organizational considerations
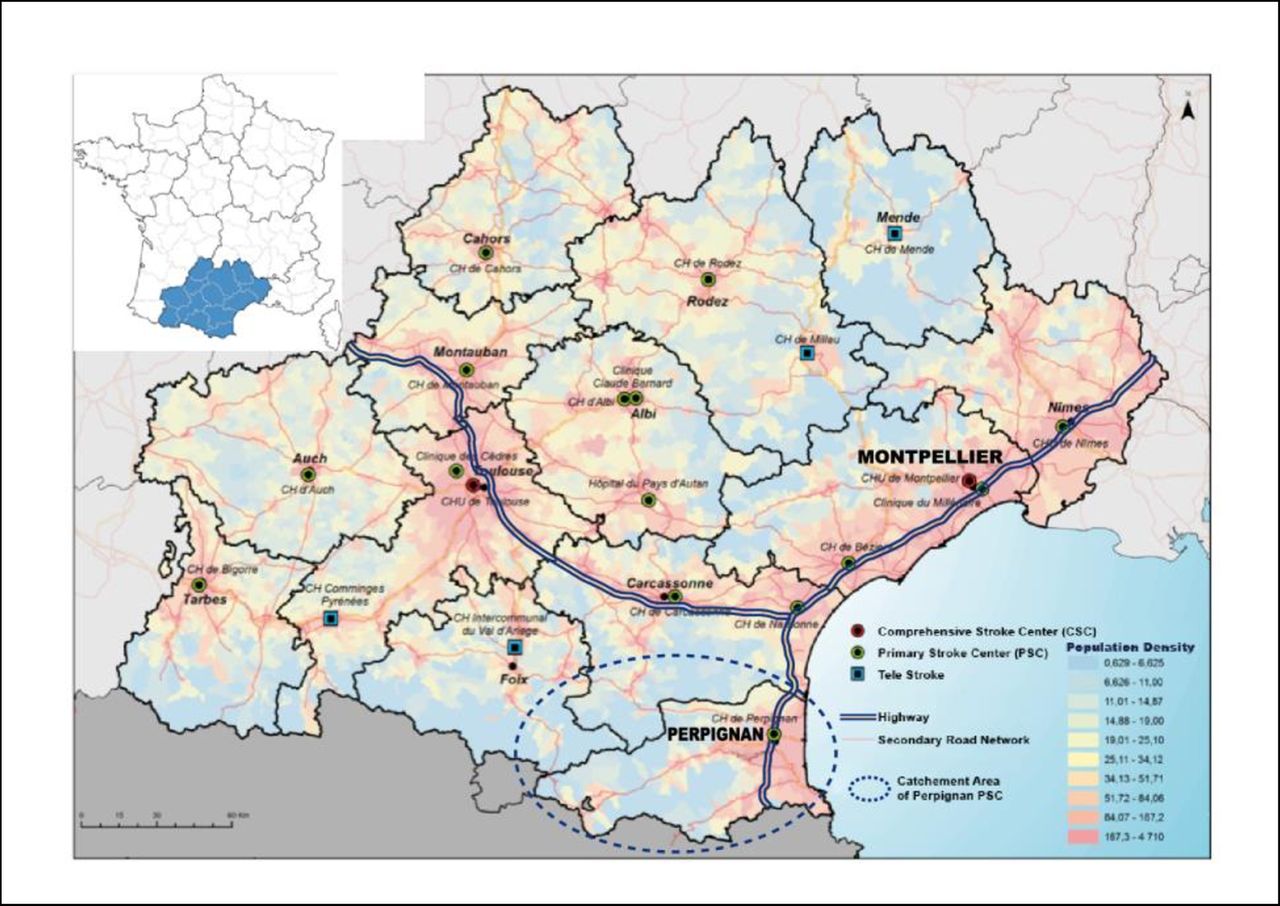
The Perpignan General Hospital (Perpignan-GH) is 156 km from the closest regional CSC in Montpellier, where there is a state-of-the-art interventional neuroradiology department. The catchment area of Perpignan-GH is a large, semi-rural, and mountainous region with approximatively 450 000 inhabitants (600 000 in summer). Perpignan-GH is the closest point to Montpellier CSC (figure 1), and virtually all villages and towns in its catchment area are further away from Montpellier. This means that direct transfer to the CSC without stopping at Perpignan-GH PSC (mothership model) would result in a time loss of approximately 2 hours for patients with IVT indication. Consequently, we opted for primary admission to Perpignan-GH PSC, with a secondary transfer to the CSC for patients with LVO. A team of 12 senior neurologists on duty 24/7 delivers IVT to >150 patients/year within 4.5 hours of symptom onset. MRI data are acquired using a 1.5T MRI scanner (TwinSpeed; General Electric, Waukesha, WI). Image sequences include diffusion-weighted images (DWI), fluid-attenuated inversion recovery (FLAIR), T2 gradient echo, three-dimensional intra-cranial time-of-flight magnetic resonance angiography centered in the region of the circle of Willis, and/or T1 MRI and/or perfusion-weighted images after injection of gadolinium in elective cases. Patients with a contraindication to MRI (eg, medically unstable, pacemaker, severe claustrophobia) are screened using computed tomographic angiography.
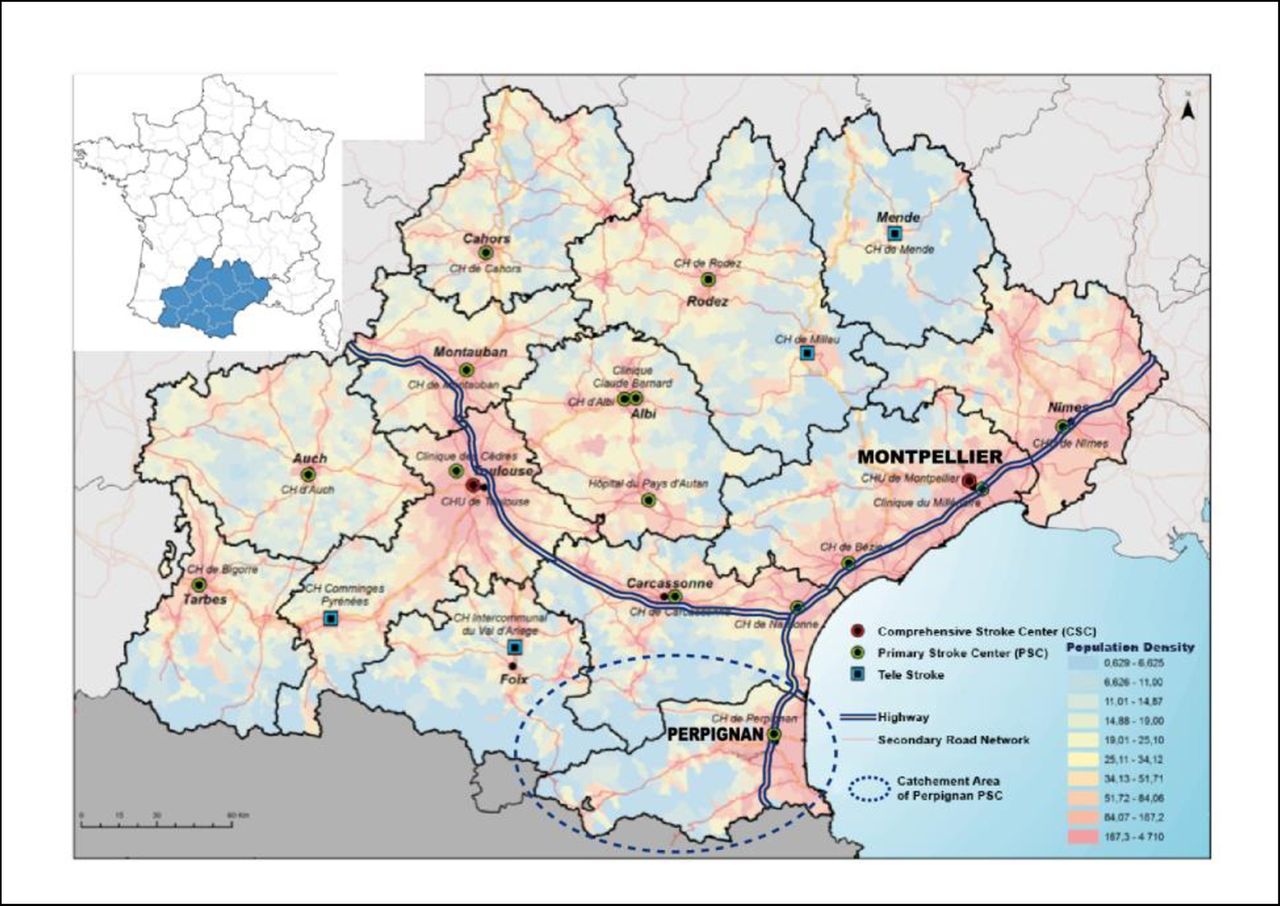
Map of the regional stroke network. The primary stroke center (PSC) catchment area is highlighted by the dotted-line circle; Montpellier: comprehensive stroke center (CSC).
Patients’ selection
Since 2010, selected patients with AIS and evidence of intracranial LVO have been transferred from Perpignan-GH to the Montpellier CSC for MT. The selection criteria for patient transfer were defined in 2010 as follows: time after AIS symptom onset <4.5 hours, or, if unknown, no visible brain infarction on T2-FLAIR sequences of the initial MRI; clinically significant neurological deficit, as indicated by a National Institutes of Health Stroke Scale (NIHSS) score ≥8; and imaging-based evidence of proximal occlusion: M1 or M1-M2 segment of the middle cerebral artery, with or without concomitant occlusion of the internal carotid artery or basilar artery occlusion. For patients with occlusion of the M2 segment of the middle cerebral artery, of the P1 segment of the posterior cerebral artery, of the A1 segment of the anterior cerebral artery, and V4 segment of the predominant vertebral artery, MT indication is discussed on a case-by-case basis. Patients with a large ischemic core on DWI, as indicated by an Alberta Stroke Program Early Computed Tomography (DWI-ASPECT) score <5, are excluded from transfer.
After agreement between the CSC team and the PSC stroke neurologist, patients are transferred as quickly as possible by the Perpignan-GH medical emergency mobile unit using air transport if available, otherwise by road. On arrival at the CSC, MRI is repeated in the case of clinical worsening or improvement during transfer (NIHSS score increase or decrease of more than four points compared with the initial score), or when the transfer time is longer than 90 min. Patients do not undergo MT when the new MRI data suggest a low likelihood of clinical improvement, according to the imaging criteria described in previous clinical trials2 4 (DWI-ASPECT score <5 and poor collateral circulation distal to the occlusion).
During the 6-year study period, some procedures were modified in the protocol. After the positive results of randomized clinical trials1–5 in 2015, patients with NIHSS <8 or DWI-ASPECT score <5 awere selected for MT on a case-by-case basis. Moreover, patients with occlusion of the M2 segment of the middle cerebral artery were systematically transferred. After February 2015, a quality improvement program to reduce door-to-needle time and door-in-door-out time was implemented at the PSC for all AIS cases.13 14 After January 2016, imaging data was systematically transmitted to the CSC using a regional digital image transfer program. After March 2016, patients with IVT contra-indications were directly admitted to the CSC (mothership model) and, from May 2017, also patients with wake-up stroke. After the publication of the meta-analysis by Saver et al in 2016,15 selected patients (based on criteria of good clinical outcome) could be transferred for MT also when the time to treatment was expected to be longer than 6 hours. The Dawn and Defuse three trials,9 10 which defined the new standard of care in the AHA/ASA guidelines,8 were posterior to our study.
Study design
This observational, single-center study (from January 1, 2012 to December 31, 2017) evaluated data concerning patients transferred from our PSC to the CSC who finally did not undergo MT. These data were collected in a prospective registry of patients admitted to Perpignan-GH PSC for AIS due to LVO within 4.5 hours of symptom onset. Patients admitted after 4.5 hours were considered ineligible for transfer because of the anticipated transport time that would have made MT impossible within 6 hours of symptom onset. The evaluated parameters were: transport modalities; FT ratio and reasons; and relevant time measurements and outcome at 3 months using the modified Rakin Scale (mRS). The outcome of the subgroup of patients who had a FT due to clinical improvement and arterial recanalization was analyzed separately. Prospective data collection via a specific stroke database was organized under the supervision of dedicated clinical research assistants, and only anonymized information was included in the analysis. The study was approved by the institutional ethics committee of Perpignan and Montpellier hospitals.
Statistical analysis
Results were presented using medians, interquartile ranges (IQR), means, and SD for continuous variables, and rates for categorical variables. Univariate comparisons between groups were made using the Student’s t-test or Wilcoxon Mann- Whitney U test for quantitative variables, as appropriate, and with the Fisher’s exact test and X 2 test for qualitative variables. The significance threshold was set at 5%. The statistical analysis was performed using SPSS, version 20.0 (IBM Corp., Armonk, NY) and ‘biostaTGV’ on-line free-access tests (http://marne.u707.jussieu.fr/biostatgv/).
Results
Cohort characteristics
Among the 529 patients who were admitted to the PSC for AIS due to LVO within 4.5 hours of symptom onset, 278 were transferred to the CSC (transfer rate=52.6%). The reasons for non-transfer were multiple and are listed in figure 2. Among the transferred patients, 69.8% had a second MRI scan on arrival at the CSC, and 45% (n=125/278) did not undergo MT (ie, FT group) (figure 2). The median age of the FT group was 68 years (DS=14) and 62.4% were males. Their median initial NIHSS score was 17 (IQR 8–20), median DWI-ASPECT score was 7 (IQR 6–8), and median mRS at 3 months was 3 (IQR 1–5). The baseline characteristics of the FT and MT (ie, patients who underwent MT after transfer) groups are shown in table 1.
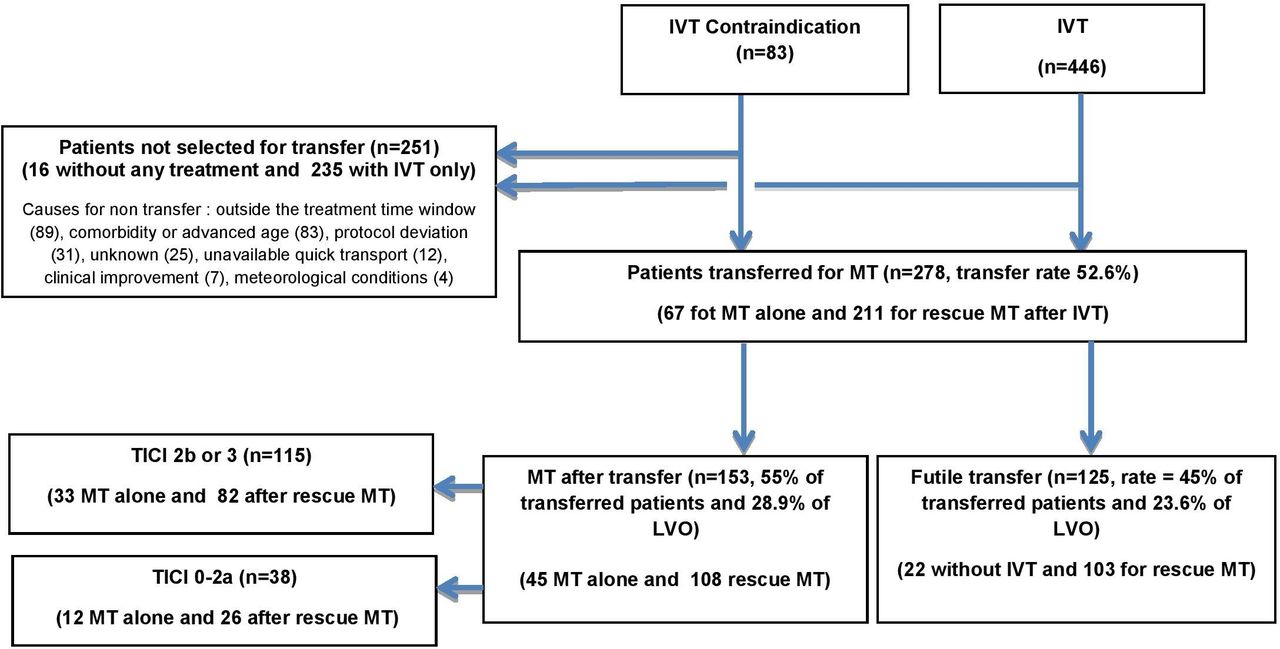
Study flow chart. AIS, acute ischemic stroke; IVT, intravenous thrombolysis; LVO, large vessel occlusion; MT, mechanical thrombectomy; TICI, thrombolysis in cerebral infarction.
Clinical characteristics and main time measures
The three main reasons for FT were: clinical improvement and reperfusion on MRI (n=73; 58.4% of all FT); clinical worsening and/or infarct growth on MRI (n=21; 16.8% of FT); and too long a transfer time (n=14; 11.2% of FT) (see table 1 for other causes). Among the 73 patients with clinical improvement and arterial recanalization on arrival at the CSC, 28.9% received IVT with rtPA before transfer and 17.9% did not (not significantly different). Analysis of the clinical and demographic characteristics did not allow the identification of any factor that could predict clinical improvement during transfer. Conversely, FT due to clinical worsening and/or infarct growth was associated with higher initial NIHSS score (21 vs 17 for all transfer; P=0.01) and lower DWI-ASPECT score (5 vs 7; P=0.001).
Main time parameters
The mean time intervals were not significantly different between the FT and MT groups: 286 vs 271 min for the symptom onset to CSC-door-in time (P=0.92), 94 vs 87 min for PSC door-in to door-out time (P=0.54), and 86 vs 95 min for PSC door-out to CSC door-in (P=0.86) (table 1).
Outcome
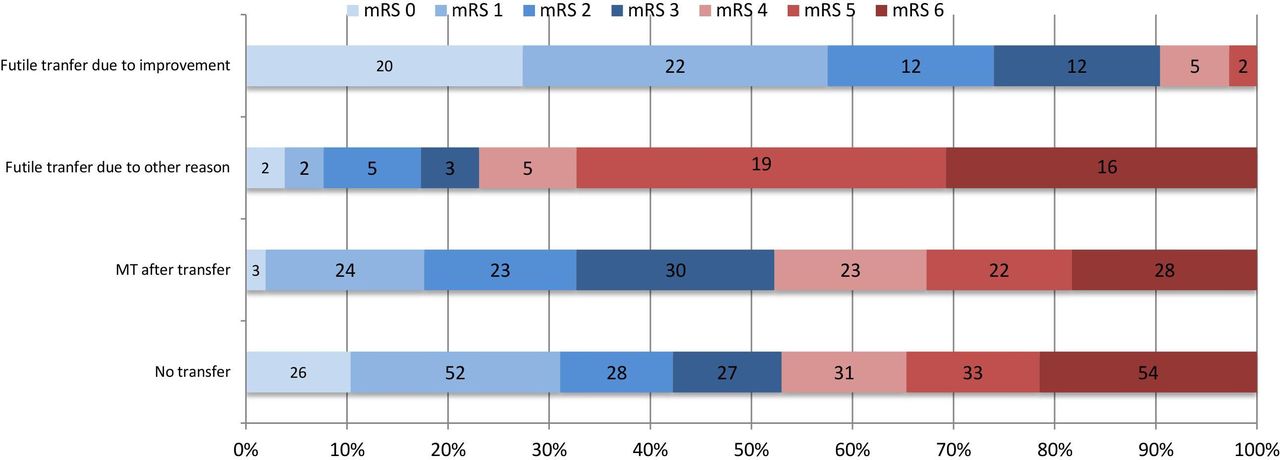
Among the 73 patients with FT due to clinical improvement and arterial recanalization during transfer, 74% had a good outcome (mRS score between 0 and 2 at 3 months). For all the other patients with FT, outcome was significantly worse compared with the MT group (mRS 0–2 at 3 months: 17.3% vs 32.7%, respectively; P=0.04) see Figure 3.

{kind=link}
{kind=link}
{kind=link}
Clinical outcome (modified Rankin Scale score) in the different groups of patients at the 3-month follow-up visit. mRS, modified Rankin Scale; MT, mechanical thrombectomy.
Discussion
The clinical course of patients who finally were excluded from MT after transfer to a CSC has rarely been addressed because these patients are generally not included in the analysis of MT studies.1–6 In our study, at departure from the PSC, all patients had a clear indication for MT, based on complete neuroimaging with adequate sequences for analysis of large vessels. However, this indication could be revised on arrival at the CSC for several reasons, including worsening, too long a transfer time, or other factors (see table 1). Other studies concluded that the absence of LVO is the most common cause of FT,16–19 but they are not comparable with our series because they did not perform pre-transfer vascular imaging to screen for LVO (in a mothership paradigm or drip-and-ship paradigm with non-contrast CT at the PSC).
Nearly half of the transferred patients (45%) did not undergo thrombectomy. This rate is higher than in other series,18 20–22(24.2% to 41%), but the distance and consequently the transfer time were longer in our situation (94 min vs 56 min in the study by Fuentes et al).20 Previous studies showed that inter-hospital transfer delays are a major cause of FT.18 23 Moreover, Prabhakaran et al suggested that MT decreases by 2.5% for every minute of transfer time.18 Thus, in our setting, the long inter-hospital distance could explain the exclusion of some patients. Nevertheless, only 5% of all transferred patients were ineligible for MT because of excessive delay, which is lower than the 14% in the study by Prabhakaran18 in an urban setting with a median inter-hospital distance of 24 km. In our study, many patients, especially those admitted to the PSC more than 4.5 hours after symptom onset, were considered not eligible for transfer because the anticipated transport time would have resulted in a time-out situation on arrival at the CSC. If included, a substantial part of these patients would have increased the FT rate due to time-out. On the other hand, the percentage of time-out cases in our study (5% of all transferred patients, corresponding to 11.2% of all FT) is higher than the 2% reported in the Madrid Stroke Network study.20 In our registry, transfer eligibility was not exclusively linked to time-related factors, and was also influenced by the CSC medical team’s clinical judgement. In the presence of several factors predictive of good outcome, MT could be decided despite the excessive transfer time. This is in agreement with a meta-analysis15 showing positive results for treatment up to 7.3 hours after symptom onset, and also with the Dawn and Defuse three trials9 10 that reported clinical benefits in selected patients with even longer delays. However, if extended to non-selected patients, this increase in treatment delays is likely to have less pronounced effects on the clinical outcome.15 Unfortunately, in our study, other non-time-related predictive factors were not investigated. For instance, the status of collateral arteries was not directly evaluated, and therefore could not be included in the decision-making criteria for MT, although it seems to be one of the most important good outcome predictors.24
In our analysis, most FTs were due to clinical improvement and arterial recanalization (58.4% of FT and 26.3% of all transfers). Although most patients received IVT at the PSC before the transfer to the CSC (28.9% of recanalization among all rtPA-treated patients), thrombolysis does not seem to explain, on its own, these clinical improvements because 17.9% of non-treated patients showed spontaneous recanalization (not significant difference with the recanalization rate of rtPA-treated patients). In fact, intravenous rtPA effectively recanalizes LVOs only in a minority of patients, and pharmaceutical lysis is ineffective in the presence of larger and longer clots.25 26 None of the characteristics at the initial evaluation could predict the spontaneous clinical improvement or arterial recanalization. Further studies with larger samples should address this question to avoid FT.
Although the protocol required a second MRI on arrival at the CSC only for patients with NIHSS score changes of ±4 points from baseline, the CSC neuroradiologist frequently requested a pre-procedure MRI control, even for patients with unchanged NIHSS score. It is unclear whether MRI should be systematically repeated, especially because it further increases the MT delay in patients with otherwise clear intervention criteria. Repeated neuroimaging has been advocated in the case of clinical deterioration during transfer or of a long interval between initial MRI and arrival at the CSC (up to 1 hour according to Fuentes et al20 and Park et al).27 In our setting, inter-hospital transfer took approximately 1.5 hours and always more than 1 hour, and most patients could be recanalized only after more than 6 hours after symptom onset (median=393 min). Several studies have suggested that a decline in the DWI-ASPECT score during transfer is associated with adverse clinical outcome.22 28 Sun et al28 showed that patients with good outcomes after thrombectomy have a lower absolute ASPECT score decrease, with a 23-fold lower probability of a good outcome for every unit of ASPECT score reduction per hour. All patients included in their analysis received IVT, but the authors did not report how many of them were excluded after ASPECT score deterioration during inter-hospital transfer. Mokin et al22 showed that during inter-hospital transfer, approximately 30% of patients with stroke resulting from LVO of the anterior circulation become ineligible for MT, based on ASPECT imaging criteria alone. They did not find any reliable and simple criteria to identify patients at risk for ASPECT score deterioration, except the NIHSS score severity,28 but they did not evaluate the collateral status at PSC, like in our series.
As expected, the group of patients not treated because of clinical improvement and recanalization during transfer had an excellent outcome (74% of patients with mRS=0–2 at 3 months). In the FT subgroup for reasons other than improvement during transfer, the odds for good clinical outcome were almost 1.9 times lower compared with patients who underwent MT (P=0.04). A conservative interpretation of our data suggests that direct access to MT with on-site interventional neuroradiological facilities would have been beneficial for most of these patients, as well as for those excluded from transfer due to too long a time after symptom onset (>4.5 hours) and thus not treated, and for those finally treated but with a transport-linked delay.26 Despite new facilities and networks, MT accessibility rate can be very low in large rural and semi-rural catchment areas that are far away from CSC.29 Therefore, we think that in such areas, conversion of high-volume PSCs into CSCs may be rational and effective in terms of public health.
Our study has several limitations. First, not all potential candidates for MT were included in our analysis, especially patients admitted to the PSC after more than 4.5 hours from symptom onset, although new trials showed that MT can be performed up to 24 hours after symptom onset.9 10 Thus, our cohort only represents a selected group of all patients who could have been eligible for MT. Second, the MRI protocol did not systematically evaluate the existence and quality of collateral arteries, which may be an important protective factor for salvageable tissue and, consequently, could influence the clinical outcome after MT, even for patients with low ASPECT score. Future studies should include this criterion in MT decision-making, and address the question of optimal penumbral tissue sustenance while waiting for MT.30 Third, despite the regional transfer protocol, MT eligibility was based on the on-call neuroradiologist’s clinical judgement. Fourth, MTindications varied during the study period, especially those for the time delay criterion. Fifth, our results concern a setting with a specific stroke network organization that is strongly influenced by local and geographical features. This limits their generalization. Nevertheless, our experience may help to rationalize and develop stroke networks in similar areas to improve MT accessibility for eligible patients in regions with an important distance between PSC and CSC.
Conclusion
Our study suggests that in a PSC located far away from the CSC (156 km), FT frequency is high for inter-hospital transfers in view of MT. Many FTs were explained by clinical improvement and reperfusion during transport. The other FTs resulted in a poor outcome. None of the baseline clinical measurements could predict FT, but the initial symptom severity was associated with FT due to clinical worsening and/or infarct growth during transportation.
Acknowledgments
We thank Corinne Cambus for her contribution to data collection.
References
Footnotes
Contributors DS, GF: conception and design of the work, data collection, analysis, interpretation of data, drafting, writing, and final approval. AD: conception and design of the work, data collection, analysis, interpretation of data, drafting, and writing. FL, AB: conception and design of the work, analysis, interpretation of data, drafting, writing, and final approval. KK: data collection, statistical analysis, interpretation of data, drafting, and final approval. BF, TA, FC, JM, PS, AF-A, AD, MT, SJ, J-MB, NO, SC, FD, LVD, SA, NG, AMM, LN-T, M-JI: data collection, analysis, interpretation of data, drafting, and final approval. IM: interpretation of data, drafting, and final approval. CA, VC: analysis, interpretation of data, drafting, writing, and final approval.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.