Article Text

Abstract
Background The crucial role of thrombectomy in the management of emergent large vessel occlusive stroke is not disputed but there is a technical failure rate in a significant minority of patients whose outcomes are often poor. Our objective was to perform a systematic review and meta-analysis to assess the safety and efficacy of permanent self-expandable stent deployment as a bailout procedure in cases of failed anterior circulation thrombectomy.
Methods Two independent reviewers searched the Pubmed (Medline) database for studies reporting outcomes following failed endovascular thrombectomy with subsequent rescue therapy employing self-expandable stents.
Results Eight studies (one prospective, seven retrospective) originating from Europe, Asia, and America comprising 160 patients met the inclusion criteria. Estimated baseline National Institutes of Health Stroke Scale score was 17.1 (95% CI 15.7 to 18.4). Following failed thrombetcomy and stent deployment, the rate of favorable outcome (modified Rankin Scale score 0–2) was 43% (95% CI 34% to 53%). Pooled mortality was 21% (95% CI 13% to 33%). Successful recanalization (Thrombolysis in Cerebral Infarction (TICI) 2b–3 or Thrombolysis in Myocardial Infarction (TIMI) 2–3) was 71% (95% CI 63% to 77%). Symptomatic intracerebral hemorrhage was seen in 12% (95% CI 7% to 18%). The Solitaire stent (Medtronic) was the most commonly deployed stent following failed thrombectomy attempts (66%; 95% CI 31% to 89%). Pre- or post-stent angioplasty was performed in 39%of patients (95% CI 29% to 48%). Glycoprotein IIb/IIIa inhibitors were used in 89% (95% CI 71% to 97%). 95% of patients received postprocedural antiplatelet therapy.
Conclusion A rescue stent procedure seems reasonable as a last resort following failed thrombectomy but currently the level of evidence is limited. Prospective registries may aid in guiding future recommendations.
- stent
- stroke
- thrombectomy
- technique
- intervention
Statistics from Altmetric.com
Multiple randomized controlled trials have demonstrated the efficacy of mechanical thrombectomy for the treatment of stroke due to emergent large vessel occlusion (ELVO)1–10 with more recent studies also demonstrating improved outcomes for selected patients last seen well up to 24 hours prior to presentation.9 10 The critical role of thrombectomy is not disputed but there is a technical failure rate in a significant minority of patients1–12 whether using a stent retriever with balloon guide catheter, distal aspiration catheter, or a combination of techniques. Importantly, the clinical outcome for patients with failed recanalization and persisting arterial occlusion is inferior, and the infarct volumes are greater.13–15 A number of factors impact on technical success, including intracranial access failure and thrombus extraction failure. The latter has been shown to be responsible for nearly half of unsuccessful procedures.16 Multiple variables are likely to govern device–thrombus interaction17 but patient factors associated with thrombectomy failure include fibrin rich18 or calcific emboli,19 intracranial atherosclerotic disease (ICAD),20 and vessel morphology.21
Prior to the publication of the battery of randomized trials investigating the efficacy of stent retriever thrombectomy, a number of preliminary studies were published assessing the efficacy of primary self-expandable stent placement in the setting of proximal occlusive stroke.22–24 These studies showed an acceptable safety profile and comparable rate of recanalization to that seen in the thrombectomy trials. Permanent stent placement has now been described as a bailout or rescue procedure in cases where thrombectomy procedures fail.25–32 Stent deployment seems an attractive option as it may maintain vessel patency where otherwise there may be persistent occlusion and a higher likelihood of a poor clinical outcome but deployment may necessitate the use of antiplatelet agents and/or angioplasty which could increase the risk of bleeding.
We chose to investigate the available evidence (in terms of safety and technical and clinical efficacy) for the use of self-expandable stents as a bailout procedure for anterior circulation ELVO through a systematic review of the literature.
Methods
Literature search strategy
Two independent reviewers systematically searched PubMed from June 2003 to June 2018. To maximize sensitivity, a detailed search strategy was employed using the following search terms: intracranial, thrombectomy, stent retriever, aspiration, large vessel, ischemic, stroke, occlusion, bailout, rescue, and endovascular. Reference lists of all retrieved articles were reviewed for further identification of potentially relevant studies.
Selection criteria
Predefined criteria were selected prior to study review. Eligible studies were those that reported outcomes after permanent stent deployment used as a rescue technique following failed mechanical thrombectomy for anterior circulation ischemic stroke. All publications were limited to those involving human subjects and published in the English Language.
Baseline demographics of the studies were extracted along with site of occlusion, use of bridging intravenous thrombolysis, type of permanent stent used, use of pre-/post-angioplasty, choice of procedural and postprocedural antiplatelets, rate of recanalization (Thrombolysis in Cerebral Infarction (TICI) score ≥2 b and Thrombolysis in Myocardial Infarction (TIMI) score ≥2), favorable clinical outcome (with a modified Rankin Scale (mRS) score ≤2 at 3 months), mortality (discharge and 3 month follow-up), and symptomatic intracerebral hemorrhage (SICH). When institutions published duplicate studies with accumulating numbers of patients or increasing lengths of follow-up, only the most complete reports were included.
Data extraction and critical appraisal
Two investigators independently reviewed each retrieved article and tabulated the data. Data were extracted from tables, figures, text, and supplementary material available from each study. If the study provided medians and IQR instead of means and SDs, we imputed the means and SDs, as described by Hozo et al.33 Attempts were made to include more studies through contact with authors to obtain subgroup data. Discrepancies between the two reviewers were resolved by discussion and consensus. Papers were quantified for bias using the Newcastle–Ottowa Assessment Scale. However, as quality scoring is controversial in meta-analyses of observational studies, the two reviewers independently appraised each article according to the Dutch Cochrane Center checklist proposed by the Meta-analysis of Observational Studies in Epidemiology (MOOSE) group. The key points of this checklist include: (i) clear definition of the study population; (ii) clear definition of outcomes and outcome assessment; (iii) independent assessment of outcome parameters; (iv) sufficient duration of follow-up; (v) no selective loss during follow-up; and (vi) important confounders and prognostic factors identified.
Statistical analysis
A meta-analysis of proportions was conducted for the available main peri-intervention and post-intervention variables. First, to establish variance of raw proportions, a logit transformation was applied. To incorporate heterogeneity (expected among the included studies), transformed proportions were combined using the DerSimonian–Laird random effects model. Finally, the pooled estimates were back transformed. Heterogeneity was evaluated using Cochran Q and I2 test. Weighted means were calculated as the total number of events divided by the total sample size. Subgroup analyses were additionally conducted to determine potential sources of heterogeneity. All analyses were performed using the metafor package for R V.3.01. A P value <0.05 was considered statistically significant.
Results
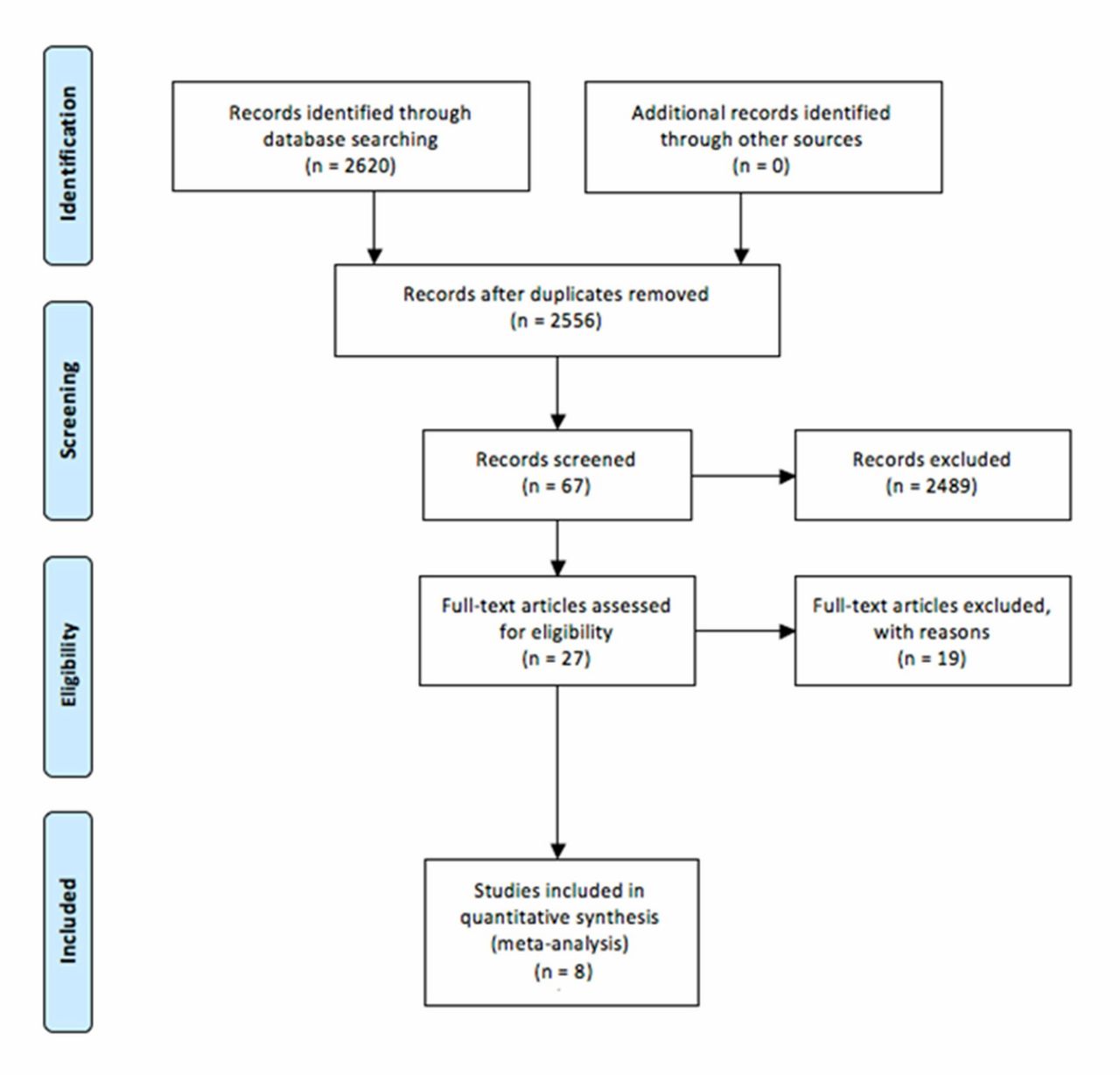
Following the removal of duplicates, a total of 2556 articles were identified from the PubMed electronic database (figure 1). After excluding all articles/letters/meta-analyses/systematic reviews, and papers not relating to cerebrovascular disease, 67 remained eligible for assessment. The abstracts of these articles were assessed by both reviewers. Forty of these were deemed not relevant and the remaining 27 were selected for full article review. Of the remaining 27, 8 met the predefined inclusion criteria and 19 were excluded for the following reasons:
Reported on primary stenting instead of rescue stenting.
Rescue stenting not preceded by thrombectomy (eg, prior use of intra-arterial thrombolytics or mechanical disruption only prior to stenting).
Mixed cohort where data could not be separated (eg, mixture of primary stenting and rescue stenting patients or mixture of anterior and posterior circulation stroke patients).

PRISMA (preferred reporting items for systematic review and meta-analysis) flowchart of the search strategy of the present systematic review.
The excluded studies are summarized in online supplement 1. Of the final eight included studies,25–32 six were retrospective single center studies, one was a retrospective multicenter study, and one was a prospective single center study. All papers scored ‘fair’ or ‘good’ using the Newcastle–Ottawa Quality Assessment Form. Study characteristics are presented in table 1. A total of 160 patients were included in the analysis.
Supplemental material
Summary of studies included in the final analysis
Baseline characteristics
The weighted mean age of all patients was 66 years (range 63–99) and 55% were men. A majority had hypertension 61% (95% CI 51% to 70%). The pooled weighted prevalence of hypercholesterolemia was 28% (95% CI 14% to 49%), atrial fibrillation 27% (95% CI 17% to 40%), diabetes mellitus type 2 30% (95% CI 19% to 43%), and ischemic heart disease 18% (95% CI 10% to 30%). The proportion of smokers was 29% (95% CI 23% to 38%). Baseline variables such as National Institutes of Health Stroke Scale (NIHSS) score, Alberta Stroke Program Early CT Score (ASPECTS), and onset to puncture time are shown in table 2. Estimated mean NIHSS was 17.1 (95% CI 15.7 to 18.4).
Baseline criteria for the patients included in each study
Site of occlusion and treatment modality employed
The majority of occlusions exclusively occurred in the middle cerebral artery (61%; 95% CI 49% to 71%). The remaining 39% involved the internal carotid artery. No cases of posterior circulation ischemia were included in the study cohort. Bridging intravenous thrombolysis was employed in 32% (95% CI 21% to 42%). The initial thrombectomy procedures employed are summarized in table 3.
Summary of the interventional techniques prior to rescue stenting
The Solitaire AB or FR stent (Medtronic) was the most commonly deployed permanent stent following failed thrombectomy attempts (66%; 95% CI 31% to 89%). The remaining stents used included the Enterprise stent (Codman) in 9% (95% CI 2% to 39%), Wingspan stent (Stryker) in 10.8% (95% CI 4% to 26%), Vision stent (Abbott-vascular) in 5% (95% CI 1% to 19%), and Neuroform stent (Stryker) in 9.4% (95% CI 1.6% to 39%) of cases.
Pre- or post-stent angioplasty was performed in 39% (95% CI 29% to 48%) of cases. Periprocedural glycoprotein IIb/IIIa inhibitors were used in 89% (95% CI 71% to 97%). The vast majority of patients (152/160, 95%) received postprocedural antiplatelet therapy (aspirin and/or clopidogrel) as the postprocedural regimen, with 112 patients receiving dual antiplatelets as standard in five of the six studies.25–28 30–32 Where clearly stated, aspirin or clopidogrel administration prior to stent implantation was rarely used. Delgado Acosta et al 28 described preprocedural aspirin use in 3/20 patients and preprocedural clopidogrel use in 6/20 patients. Chang et al 29 employed differing strategies with variable timing of aspirin or clopidogrel administration in the periprocedural period. The details of the antiplatelet regimens included in each study are summarized in table 4.
Antiplatelet regimen employed in each study
Procedural success
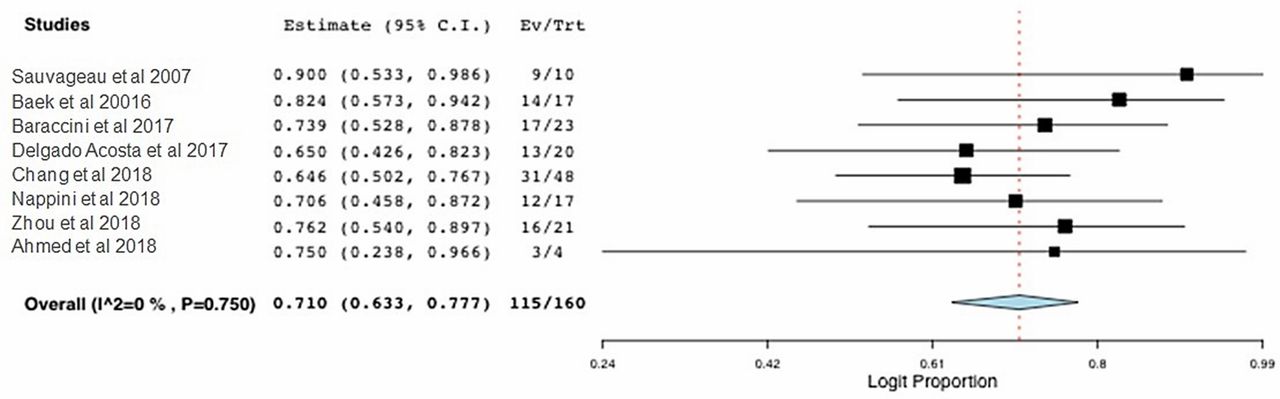
Weighted pooled estimate of successful recanalization (TICI 2b–3 or TIMI 2–3) was 71% (95% CI 63% to 77%) (see figure 2). The weighted pooled estimate of procedural related symptomatic intracerebral hemorrhage was 12% (95% CI 7% to 18%) (see figure 3). Other non-intracranial complications including groin hematoma or infection occurred in 15%.

Forest plot of rates of successful recanalization (Thrombolysis in Cerebral Infarction (TICI) 2b–3 and Thrombolysis in Myocardial Infarction (TIMI) 2–3).

Forest plot for rates of symptomatic intracerebral hemorrhage.
Functional outcome and mortality
The rate of favorable outcome (mRS score 0–2) was 43% (95% CI 34% to 53%). Pooled mortality was 21% (95% CI 13% to 33%) (see figures 4 and 5).

Forest plot of independent outcome rates (modified Rankin Scale score 0–2).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of mortality.
Discussion
It is well established that successful recanalization is associated with favorable outcome for ELVO.34 However, recanalization failure is not uncommon during thrombectomy. Trial and observational evidence suggests that there is a technical failure rate (TICI 0–2a) of 14–41% whether using a stent retriever and balloon guide catheter, distal aspiration catheter, or a combination of techniques.1–12 As well as intracranial access failure, thrombus extraction failure is responsible in approximately 40% of unsuccessful procedures.16 The natural history of non-recanalized ELVO stroke is poor,35 and equally, those patients suffering procedural failure commonly fair poorly also. In the Solitaire With the Intention For Thrombectomy as Primary Endovascular Treatment (SWIFT PRIME) trial,15 70% of patients with successful reperfusion assessed at 27 hours achieved functional independence compared with only 18% without successful reperfusion. Similarly, in the Endovascular Revascularization With Solitaire Device Versus Best Medical Therapy in Anterior Circulation Stroke Within 8 Hours (REVASCAT) trial, arterial patency (modified arterial occlusive lesion grade (mAOL) 3) at 24 hours was associated with functional independence in 54% compared with 29% in those with lesser degrees of patency (mAOL 0–2).14 A number of studies have assessed outcome in cohorts of patients with thrombectomy failure and for these patients the favorable outcome rate lies in the order of 16.6–22%.26 27 It is well recognized that longer procedural times and multiple device passes are associated with worse outcomes.36 37 Additionally, data from the North American Solitaire Stent Retriever Acute Stroke registry suggests that ‘rescue therapy’ (although a very non-specific term that can encompass multiple maneuvers) is an independent predictor of poor outcome.37
In contrast, the results of this analysis suggest that in cases of failed thrombectomy, rescue deployment of self-expandable stents is associated with successful recanalization in 71% and favorable clinical outcome in 43%. These results are encouraging considering that this population have selected themselves as the most difficult to treat. Although not directly comparable, these results are somewhat supported by the results of the small but prospective Stent-Assisted Recanalization in acute ischemic Stroke (SARIS) trial22 that investigated the efficacy of primary stenting (primarily with the Wingspan device; Stryker) in cases of ELVO. In 20 patients, TIMI 3 recanalization was achieved in 60% and a favorable outcome rate (mRS 0–1) in 40% and (mRS 0–3) in 60%. Early recognition that the thrombectomy procedure is failing and that an alternative approach (such as permanent stenting) is required may be crucial in achieving a favorable outcome in some patients. Protracted unsuccessful procedures with multiple passes may render rescue therapy futile37 .There is insufficient evidence to create a guideline currently but it may be prudent to contemplate stenting if the procedural time is extending beyond 90 min or over three passes with no progress,36 37 but size of core infarct and time from ictus should be considered.
Patient factors which may govern thrombectomy failure include thrombi rich in fibrin or calcium.18 19 The resistance of calcific emboli to thrombus extraction has previously been described in detail.19 In addition, recanalization failure or arterial re-occlusion post-thrombectomy is well recognized in cases of ICAD.20 Although this is relatively rare in Caucasian populations, it may account for a third of proximal intracranial occlusions in Asian populations.38 39 The etiology of the occlusions in this study were likely diverse as the populations included were from European, American, and Asian countries, and there is some justification for including all causes of thrombectomy failure in a single analysis as the etiology of the resistant occlusions in all populations may be multifactorial and may only become apparent after commencing the procedure.
As well as permanent stent deployment, other rescue techniques that have been described include catheter delivery of thrombolytics and glycoprotein IIb/IIIa inhibitors, angioplasty,17 or use of double or Y stent retriever approaches, the latter for bifurcation lesions.40 Data regarding the efficacy of these approaches are sparse and limited to case reports or small series. The Interventional Management of Stroke (IMS) 1 and 2 trials41 42 gave relatively reliable data on the efficacy and safety of intra-arterial alteplase administration with SICH rates of 6.3–9.9% but the efficacy for thrombectomy resistant thrombi must be questioned. Additionally, rescue intra-arterial infusion of tirofiban alone was shown to be relatively ineffective by Barranchini et al 27 who demonstrated in a European population that only 3 of 19 patients attained successful reperfusion with intra-arterial tirofiban infusion after failed thrombectomy. Just as stent retrievers represented an evolutionary leap in the treatment of ELVO over the Merci device,43 44 more recently a newer generation of devices, including Embotrap (Ceronovus), have been developed with the aim of facilitating the removal of more resistant thrombi but the real world efficacy compared with traditional stent retrievers is as yet untested. In a recent prospective trial, the failure rate (TICI 0–2a) after three passes was still 20%, suggesting a persisting need for an efficient bailout technique.45 Registry data suggest that use of balloon guide catheters does lessen the need for rescue treatments.46
A real fear when deploying a stent in the setting of ELVO is the associated bleeding risk when using antiplatelet therapy. The SICH rate in this study was 12% (95% CI 8% to 17%). This is similar to recent real world published rates of SICH in stent retriever registries47 but higher than that seen in the randomized trials, which was of the order of 0–8%.1–10 Many patients were treated with thrombolytics prior to stent deployment which may have increased the bleeding rate. Eighty-nine per cent of patients were treated with glycoprotein IIb/IIIa inhibitors and the vast majority had dual antiplatelet therapy with aspirin and clopidogrel postprocedure. The evidence regarding the safety of glycoprotein IIb/IIIa inhibitors is controversial. An earlier study48 described a doubling of the SICH rate with its use in the anterior circulation (20% vs 10%) but overall recanalization rates TICI 2b/3 were low (60%) which may have contributed to greater infarct volumes and bleeding risk. Conversely, Woo et al 49 specifically analyzed SICH in those who had undergone angioplasty and stenting for ELVO with and without glycoprotein IIb/IIIa inhibitors. The SICH rate was 5.6% when treated with glycoprotein IIb/IIIa inhibitors versus 22.2% without. Acute stent re-stenosis was also 50% at discharge when treated without the drug but when glycoprotein IIb/IIIa inhibitors were used there was no acute re-stenosis demonstrated. The results imply that maintaining vessel patency and lowering infarct core volume may lessen bleed risk. It should be mentioned, however, that overall numbers in this study were small. The question remains as to whether the risk of glycoprotein IIb/IIIa inhibitors is justified but large prospective registries could give an answer. Recent registry data suggest that postprocedural dual antiplatelet treatment is safe in the context of ELVO and cervical internal carotid artery stenting50 with no significant increase in SICH but with more favorable recanalization rates. In the authors’ experience, use of Dyna CT to assess for contrast staining in areas of core infarct postprocedure could guide the use of or extent of antiplatelet therapy.
Another factor which may influence the results is choice of stent. In two-thirds of patients treated in this analysis, the Solitaire device was used. This closed cell stent is an attractive option as it is easy to deploy and can be re-sheathed and re-sited if necessary. However, if the radial force of this stent is insufficient to maintain patency, re-crossing the stent and performing an angioplasty can be challenging. Indeed, angioplasty was performed in 39% of cases in this study and whether performed before or after stent deployment, particularly in the setting of ICAD, is likely to be an important facet of the treatment as suboptimal angioplasty has been shown to be associated with early stent re-occlusion.20 The radial force of the stent may govern the need to angioplasty or even repeat angioplasty after deployment. When comparing stents, in vitro testing shows variable results dependent on the technique used, but irrespective of technique, the Wingspan stent (with open cell design) shows greater force compared with the Enterprise (closed cell), Solitaire, and Neuroform (opened cell) stents.51 Solitaire and Neuroform radial force relative to each other is dependent on the test method but at higher oversizing, the Solitaire shows greater radial force whereas the Neuroform shows greater radial force at lower oversizing.51 Generally, the Wingspan stent is less commonly used following the results of Stenting and Aggressive Medical Management for Preventing Recurrent Stroke in Intracranial Stenosis (SAMMPRIS) trial.52 The system has been criticized for being cumbersome and requiring a multistep deployment53 54 employing initial angioplasty, microwire exchange, stent placement, and possible further exchange for re-angioplasty. This has led some authors to advocate the use of balloon mounted stents.55 However, in the Vitesse Intracranial Stent Study for Ischemic Stroke Therapy (VISSIT) randomized trial,56 that employed balloon mounted stents in the setting of ICAD, successful stent placement was achieved in only 54% of patients, perhaps a reflection of the more rigid stent deployment systems. It appears that the neurointerventional community does not yet have an optimal device for this scenario. A novel approach to ICAD stenting using the Atlas device (Stryker) delivered directly through an angioplasty balloon catheter lumen has been described, obviating the need for an exchange but maintaining access with a stent delivery wire.57 This could be an elegant solution in this situation.
Long term stent patency is also a concern and necessitates follow-up. Although data governing this cannot be gleaned from the studies included in this analysis, mid-term angiographic follow-up was obtained following the SARIS trial.58 In all survivors, none developed an in-stent stenosis of >50% but again it should be reiterated that numbers in the trial were small. Similar findings have been demonstrated by Natarajan et al 59; no in-stent stenosis was demonstrated in 8 of 13 surviving patients who had catheter angiography. They also demonstrated favorable clinical (mRS 0–2) outcomes in 11 (55%) enrolled patients at 2 years. No data are available regarding the long term appearances of thrombus remodeling in rescue stenting, where more resistant thrombus or ICAD may be present.
This analysis is limited by the quality of the studies included, most of which were single center and retrospective in nature. Most studies were small in number. Publication bias could therefore be a significant factor and this could minimize the validity of the results. Studies of better design investigating primary stent placement were available but they did not answer the utility of stenting in a bailout scenario. Many confounding factors which are known to impact on outcome, including baseline core infarction, collateral quality, and time to puncture, were variable as was the initial thrombectomy technique prior to adopting a rescue approach (summarized in table 3) which may limit generalization of results. As mentioned previously, the etiology of the occlusions will differ between populations and it is not possible to elucidate the merits of a stent deployment as a rescue treatment for differing etiologies based on these data.
In conclusion, use of self-expandable stents as a bailout procedure appears to be a reasonable approach bearing in mind the natural history of failed thrombectomy. However, it should be recognized that the level of evidence for this approach is limited and the studies that have described this approach are mostly retrospective and heterogenous in terms of patient inclusion and stroke etiology. Optimal device and antiplatelet regimen remain to be elucidated. A prospective registry of patients undergoing rescue stenting would be a useful project to obtain further evidence to guide future recommendations.
References
Footnotes
Contributors JW and RF: drafting/revising the manuscript, study concept or design, analysis or interpretation of the data, and acquisition of the data. KP: drafting/revising the manuscript, analysis or interpretation of the data, and statistical analysis. RC and AM: drafting/revising the manuscript, study concept or design, analysis or interpretation of the data, and study supervision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests RC: consultancy for Microvention and speaking honorarium for Stryker.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data are available in the manuscript.