Article Text

Abstract
Background The efficacy of SILK flow diverters (SFD) in the management of cerebral aneurysms has been established. However, the risk of complications with parent artery occlusion (PAO) remains to be fully elucidated. The purpose of our study was to analyze intracranial aneurysms treated with SFDs and assess for occurrences and potential risk factors for PAO.
Materials and methods Between September 2010 and September 2017, 34 patients were treated for intracranial aneurysms using SFDs at a Canadian institution. This database was retrospectively analyzed for frequency of PAOs and statistical analysis performed for potential contributing factors.
Results Following treatment with SFDs, average clinical and imaging follow-ups were 31 and 22 months, respectively. PAOs were identified in 21% (7/34) of patients and occurred between 8 days and 1.5 years from intervention but only in 11.8% in those compliant to anti-platelet medications. These were all associated with anterior circulation aneurysms (P=0.131) and had no associated neurological deficits. Of these, 57% (4/7) had a fusiform morphology compared with only 19% (5/27) in non-occluded patients (P=0.039). The presence of clinical symptoms at the time of initial SFD intervention was significantly associated with PAO (P=0.021).
Conclusion Delayed PAO is not an uncommon outcome of flow diverter deployment and could be seen up to 1.5 years after treatment with no associated neurological deficits. Anti-platelet non-adherence remains a risk factor for PAO. Fusiform morphology of the aneurysm and symptoms at the time of intervention were associated with subsequent occlusion.
- aneurysm
- brain
- device
Statistics from Altmetric.com
Introduction
Flow diverters are an important tool in the treatment of complex intracranial aneurysms. Traditional approaches, such as coil embolization or vascular clipping, are quite challenging for aneurysms that are typically larger, fusiform in shape, or have wide necks.1 2 In this respect, the class of flow diverters are flexible stents that self-expand, conform to the native vessel, and divert blood flow away from the aneurysm sac.3 Subsequently, blood flow in the aneurysms treated with flow diverters will become stagnant and thrombose over time. There are a number of flow diverters in clinical use including the SILK stent (Balt Extrusion, Montmorency, France), Pipeline device (Medtronic, Minneapolis, MN), SURPASS (Stryker, Kalamazoo, MI), FRED (MicroVention, Aliso Viejo, CA), and p64 (Phenox, Bochum, Germany). The efficacy of flow diverters in the management of cerebral aneurysms has been established4–14 with grading schemes proposed for the degree of aneurysm occlusion after deployment.15 16 However, complications are a central issue in the use of flow diverters for the treatment of complex intracranial aneurysms and have slowed widespread adoption of these interventions.6
Flow diverter devices are composed of braided strands that form a high coverage mesh when expanded and come usually in various diameters (2–5 mm) and lengths (15–40 mm) depending on the target aneurysm characteristics and location. Technical differences exist between devices, for example the SILK allows re-sheathing and repositioning even when up to 90% of the length has been deployed. In contrast, the differing materials in the various flow diverters may contribute to the observation that SILK may have higher rates of incomplete opening when deployed.17 18 Complications of flow diverter intervention can include delayed aneurysm rupture, distal intracerebral hemorrhage, in-stent thrombosis, and stent migration. Furthermore, these events are generally unpredictable and poorly understood.19 20 Complication rates between devices remains uncertain as some studies suggest similar rates21 while others suggest advantages of certain flow diverters.22 In addition, as flow diverter technology continues to improve, it may be challenging to extrapolate from older studies using previous generations of devices.23 Parent artery occlusion (PAO) following treatment with flow diverting devices is a particular phenomenon reported in 2% to 14% of procedures7 13 17 18 23–26 and may be even higher in certain series.7 In PAO, blood flow to the aneurysm is stopped after device deployment, however upstream and downstream native artery flow is also completely obstructed. Furthermore, several studies have determined that in-stent thrombosis and parent artery stenosis, in which blood flow is impaired but not completely obstructed, occurs in up to 57%23 and 33%24 of patients, respectively. Despite previous literature reports, the timing of PAO, clinical impact, and risk factors have not been fully elucidated. It is important to note that PAO has been one of the accepted treatments for large fusiform aneurysms.27 The purpose of our study was to analyze our single center database of intracranial aneurysms treated with SILK flow diverters (SFDs) and assess for occurrences, clinical outcomes, and contributing risk factors for PAO.
Methods
This study used a database of consecutive patients treated with SFDs between September 2010 and September 2017. All patients were treated by an experienced interventional neuroradiologist. The study was approved by the Nova Scotia Health Authority research ethics board.
Patients were followed routinely in clinic and with post-procedure imaging at 3 months, 6 months, 1 year, and beyond. This database collected patient metrics on age, sex, location of aneurysm, diameter of aneurysm, aneurysm neck type and size, indication that led to diagnosis, imaging modality of diagnosis, and whether alternative treatment options to SFDs (such as micro-surgical clipping or conventional or assisted coiling) were considered (table 1). Procedure metrics such as numbers and size of SFDs used, duration of procedure, whether adjuvant tools (for example hyperglide or enterprise stents) were used, and any technical problems reported. Outcome metrics included months of clinical and imaging follow-up, aneurysm occlusion, PAO, clinical outcome, and patient deaths at follow-up. This database was retrospectively analyzed for frequency of PAO and for potential contributing factors. All patients were started with dual antiplatelet therapy with Aspirin and Plavix at least 5 days prior to the treatment and they continued the dual antiplatelet therapy for 3 months and Aspirin only thereafter for the rest of their life.
Demographics and aneurysm characteristics
All data were analyzed using SPSS statistics 24 software package (IBM Corporation, Somers, NY). t-test and chi-squared tests were performed where appropriate. Statistical significance was concluded at P≤0.05 without using a multiple testing correction.
Results
A total of 35 patients underwent treatment of intracranial aneurysms using SFDs in this study duration. One procedure was excluded from our analysis as it was an intra-procedural occlusion rather than delayed PAO. Patient demographics, clinical measures, procedural measures, and aneurysm characteristics between occluded and non-occluded parent artery patients following SFD intervention are represented in table 1. Patients treated with SFDs that had PAO did not have a significant difference with respect to their age or sex compared with non-occluded patients. Following treatment with SFDs, average clinical and imaging follow-up was 31 (range 0–83) and 22 (range 0–82) months, respectively. Aneurysms were located in the anterior circulation in 27 patients and in the posterior circulation in seven patients. PAOs were identified in 21% (7/34) of patients and all were located in anterior circulation aneurysms. It is important to note that three out of these seven patients were known to be non-compliant or known to have discontinued their anti-platelet medications. After removing these, the actual incidence of PAO was only 11.8% (4/34). Notably, the presence of clinical symptoms, which most commonly was reported as headache (3/7, 43%) but also included diplopia (1/7, 14%), at the time of aneurysm diagnosis and SFD intervention was significantly associated with subsequent PAO (P=0.021). Of aneurysms associated with PAO, 57% (4/7) had a fusiform shape compared with only 19% (5/27) in non-occluded patients (P=0.039). PAO predominantly involved the internal carotid artery (figure 1), however 71.4% (5/7) were asymptomatic in clinical follow-up. In the seven occurrences of PAO, two patients were non-compliant with their post-op anticoagulation regimen (occlusions noted on 4.5, and 6-month follow-up imaging, respectively). Another patient developed a left middle cerebral artery territory infarct with identified occlusion during an unrelated general surgery procedure 4 months after SFD deployment. The remaining four patients did not have clear inciting events for occlusion on clinical history and were demonstrated on follow-up imaging between 8 days and 1.5 years post -intervention.
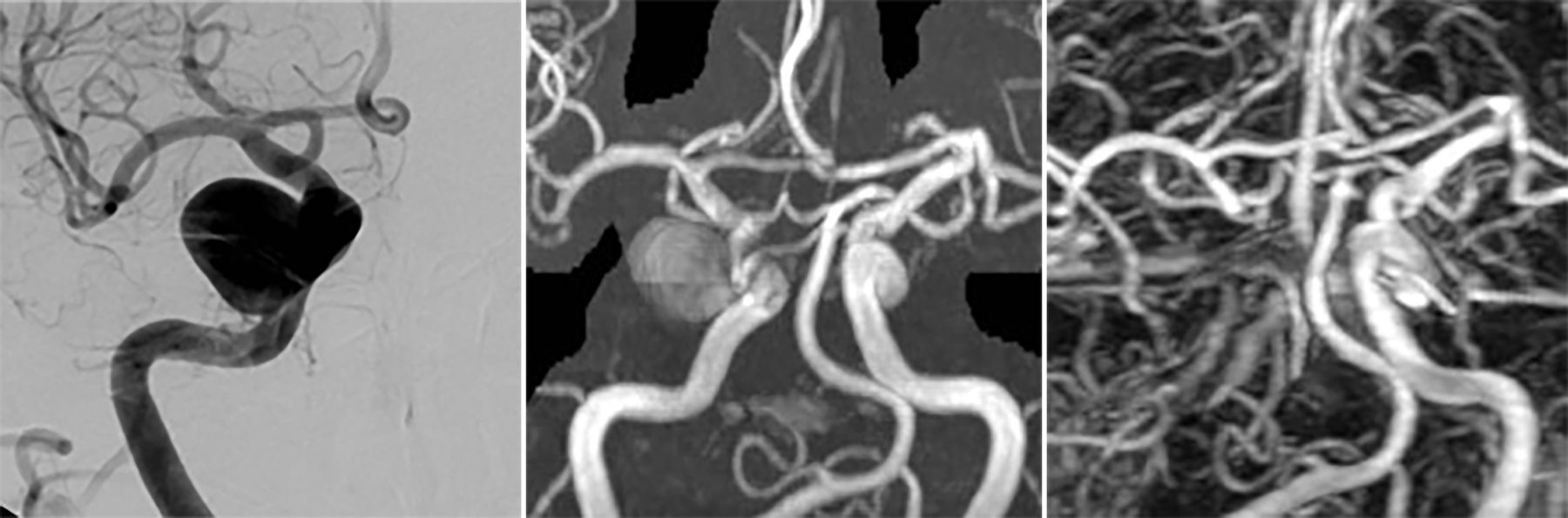
{kind=link}
Example of parent artery occlusion post-SILK deployment. Right cavernous aneurysm as demonstrated on angiography before intervention (Left). MR angiography follow-up 2 months after SILK deployment demonstrated a partially thrombosed aneurysm (Middle). Complete occlusion of the right internal carotid artery was identified at 6-month follow-up and remained occluded at most recent imaging, 6.5 years after SILK deployment (Right). This patient had been non-compliant with Aspirin and Plavix therapies post-intervention, however did not have any neurologic deficits associated with occlusion.
There was no association with characteristics of the SFD procedure such as technical issues during deployment, including the use of balloon dilatation or requiring multiple attempts to access the aneurysm or associated vessel, between the occluded and non-occluded patients. A subjective measure, whether other interventions could have been considered in place of SFD, was determined by a single interventional neuroradiologist. There was no significant difference between the occluded and non-occluded groups.
Patients with PAO had significantly longer clinical follow-up (P=0.015) and a trend toward longer imaging follow-up (P=0.071).
Discussion
Our experience with SFDs represents one of the largest in Canada for the use of this device in the treatment of complex intracranial aneurysms with long-term follow-up. Delayed PAOs were found to occur in 21% of patients treated with SFD but only 11.8% in those who remained compliant to their anti-platelet medications. In our study, the presence of fusiform morphology was significantly associated with PAO (P=0.039), however the relatively small number of patients remains a limitation. Fusiform morphology, in which there is circumferential dilatation over a short arterial segment, presents a unique challenge to SFD deployment.28 Stent anchorage of fusiform aneurysms typically involves a small contact area with the parent artery, thus potentially introducing a conical shape of the SFD or increasing the prolapse risk.29 This may result in altered flow dynamics that contributes to a higher risk for PAO. It is important to note that PAO has been one of the accepted treatments for large fusiform aneurysms although a complication rate of up to 28.6% has been reported.27 Furthermore, SILK intervention for fusiform aneurysms in our study was technically successful at the time of deployment and it is important to note that none of the patients who developed PAO in our series developed neurological deficits immediately after the treatment and/or on follow-up.
Based on our database, there was a significant association of PAO with the presence of symptoms at time of diagnosis (P=0.021). These ranged from nonspecific, such as headache, to focal neurological changes, such as diplopia. The pathogenesis of this contribution for PAO, however, remains unclear. Furthermore, there were no technical components, such as duration of the procedure or use of adjuvant tools that contributed to the risk of PAO. There has been an association of PAO with iatrogenic dissection at the time of intervention.30 However, dissection was not identified in any of our patients, even in retrospect. It does remain possible that occult dissections may contribute to PAO as previously suggested30 and that these events are not identified on routine imaging follow-up.
Interestingly, in three cases of PAO, there were identified inciting factors such as noncompliance with anti-platelet medications or subsequent surgery. Given the study size limitation, this represents a significant portion of the patients who developed PAO. As has been proposed earlier,19 it remains to be elucidated the optimal agents and duration of anticoagulation therapy post-flow diverter stent deployment. Our study provides further evidence that PAO may be associated with poor adherence to this therapy. One of the limitations of our study, was that none of the patients were tested for resistance to anti-platelet medications before SFD treatment. Such assays were not available in our center at the time of the treatment but may be an important risk stratification for PAO.
In patients without inciting events, there was a relatively wide timeframe for identification of PAO. In one instance this occurred relatively close to initial deployment (8 days) while in another case this was identified after 1.5 years on regular imaging follow-up. Furthermore, the overall incidence of PAO (21%) in our study is higher than that previously reported in the literature on flow diverters. But the incidence was only 11.8% among those who remained compliant to their anti-platelet medications. Although patients with potential inciting events such as antiplatelet non-adherence and subsequent surgery were included in our analysis, these remain PAO risk factors thus, consistent with previous studies,7 13 17 26 are suitable for inclusion in determining complication rates of SILK deployment. One contributing factor to the current PAO prevalence may be the long duration of follow-up required to truly capture PAO events. In addition, PAOs were generally associated with transient symptoms of headache on routine clinical follow-up without focal neurological deficits. This may further suggest that unless prolonged routine imaging follow-up is provided for patients, PAOs are difficult to detect based solely on clinical findings. Of note is that high rates of parent artery stenosis (33%)24 and in-stent thrombosis (57%)23 have been reported in routine follow-up after SILK deployment and while these findings may be transient,13 26 it is conceivable that a subset of these patients may be at risk of progression to PAO as has been previously demonstrated.23 Furthermore, the specific timeframe of progression from parent artery stenosis to occlusion is unclear and may be important in guiding clinical and imaging follow-up. The higher rate of PAO in this study may reflect the true incidence in reporting of complications on long-term follow-up, as opposed to some studies reporting no complications.31
Patients with PAO were followed longer, both in clinic (P=0.015) and with imaging (P=0.071), to monitor symptoms as well as to determine if recanalization of occluded arteries occurred. There was no recanalization in any of the patients. Despite having long-term follow-up, our study is limited due to the small number of patients and relatively limited follow-up. This study highlights the need for long-term clinical, as well as imaging, follow-up of patients treated with flow diverters.
Conclusion
Delayed parent artery occlusion is not an uncommon outcome of flow diverter deployment and could be seen up to 1.5 years after treatment with no associated neurological deficits. Anti-platelet non-adherence remains a risk factor for PAO. Fusiform morphology of the aneurysm and symptoms at the time of intervention were associated with subsequent occlusion.
Acknowledgments
The authors would like to thank Helen Wong for her assistance in the organization and management of the clinical database.
References
Footnotes
Contributors JJSS contributed to the project conception. IRM and JJJS contributed to the acquisition, analysis, and interpretation of data as well as the drafting and final approval of the manuscript. All co-authors are in agreement with the content of this manuscript and it has not been published or under consideration for publication elsewhere.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests JJSS is a proctor for SILK in Canada and has received honorarium from BALT for flow diverter proctorship. IRM has no conflicts of interest.
Patient consent Not required.
Ethics approval Nova Scotia Health Authority research ethics board (Halifax, NS, Canada).
Provenance and peer review Not commissioned; externally peer reviewed.