Article Text

Abstract
Background Initial clinical experience with Squid shows subjectively reduced artifacts on post-embolization CT scans compared with Onyx. To further investigate these observations, we aimed to perform a comparison of artifacts between Squid and Onyx in a controlled in vitro model.
Materials and methods Onyx 18 and all four variants of Squid (Squid 18, Squid 18 low density (LD), Squid 12, Squid 12 LD) were each injected in dimethylsulfoxide (DMSO) compatible test tubes. The tubes containing precipitated embolic material were inserted in a CT phantom for conventional and flat panel CT acquisitions. Beam hardening artifacts were quantified using objective and subjective measurements.
Results Objective evaluation of artifacts within regions of interest (ROIs) placed around the embolic material on CT and flat panel CT images demonstrated significantly lower noise and Hounsfield unit (HU) range values for all four Squid products compared with Onyx 18. On both CT and flat panel CT, LD variants of Squid 18 and Squid 12 had significantly lower noise and HU range values than their normal density counterparts on longitudinal ROIs. When using subjective measures for diagnostic value within ROIs placed around the embolic material on both CT and flat panel CT images, the number of non-diagnostic ROIs was significantly higher for Onyx 18 than for all four Squid variants.
Conclusion All four variants of Squid induced fewer beam hardening artifacts than Onyx 18 on CT and flat panel CT acquisitions. LD variants of Squid induced fewer artifacts than their normal density counterparts.
- arteriovenous malformation
- ct
- liquid embolic material
Statistics from Altmetric.com
Introduction
Liquid embolic agents are widely used in interventional neuroradiology for the treatment of brain arteriovenous malformations, dural arteriovenous fistulas,1–5 and presurgical tumor embolizations.6 Most procedures are now performed using precipitating agents, which contain a polymer that precipitates in contact with blood. Onyx (Medtronic, Dublin, Ireland) is the most widely used product; it contains ethylene vinyl alcohol (EVOH) as the active ingredient.
EVOH liquid embolic agents are rendered radiopaque by addition of tantalum powder in the initial solution. To obtain suspension of tantalum within the solution to be injected, the vials need to be agitated prior to use. After injection, tantalum is fixed in the solidified EVOH cast after precipitation and thus the final embolic mass remains radiopaque indefinitely. This induces beam hardening artifacts on CT scans performed after embolization.7 8 Depending on the quantity of embolic agent, these artifacts can severely impair diagnosis of hemorrhage and/or ischemia in the proximity of the malformation.
Until recently, Onyx was the only EVOH embolic agent available. From 2012, a new product became available—Squid (Balt, Montomorency, France)—in certain countries, following expiration of initial proprietary patents. Initial experience with Squid shows subjectively reduced artifacts on post-embolization CT scans. To further investigate these observations, we aimed to perform a comparison of artifacts between Squid and Onyx in a controlled in vitro model.
Materials and methods
Onyx 18 and all preparations of Squid (Squid 18, Squid 18 low density (LD), Squid 12, Squid 12 LD) were each injected in dimethylsulfoxide (DMSO) compatible test tubes. The tubes containing precipitated embolic material were inserted in a CT phantom for conventional and flat panel CT acquisitions. Beam hardening artifacts were quantified using objective and subjective measurements.
Injection procedure
The embolic products were placed in an agitator for a minimum of 20 min and then aspirated in 1 mL DMSO compatible syringes. One phial of embolic agent (1.5 mL) was injected through a Sonic 1.5 F microcatheter (Balt Extrusion, Montmorency, France) with the tip placed at the bottom of a vertically positioned test tube filled with saline solution. During injection of the embolic product, the tube was continuously flushed with saline solution through a long 18 gauge needle placed at the bottom of the test tube, next to the tip of the microcatheter. Injection of embolic and the saline flush were performed at a constant rate over 2 min; a total volume of 100 mL of saline was used for the flush. The microcatheter was cut at 40 cm for easier manipulation and to decrease deadspace volume. The saline solution was warmed to 37°C prior to use.
The continuous saline flush during injection was necessary to ensure clearance of DMSO liberated from the embolic solution during precipitation. During initial exploratory experiments, we observed that, in absence of a continuous flush, as DMSO is heavier than saline, it forms a layer between the EVOH (inferior) and the saline (superior) solution. This layer isolates EVOH from the saline solution and subsequently impairs correct precipitation.
We initially considered using swine blood for the flush, in order to better replicate in vivo conditions. We chose to use saline because there are no known differences in the process of precipitation, which only requires contact with an ionic solution, and also to comply with the guiding principles underpinning the humane use of animals in scientific research (the three Rs—reduce, replace, refine). The use of a large volume of animal blood for this purpose would not have been ethically justified in this context.
Image acquisition
The tubes with the precipitated embolic products were inserted successively in the central slot of an adult head CT phantom (model 007TE-2; CIRS Tissue Simulation Technology, Norfolk, Virginia, USA). Prior to insertion, the tubes and the slot were coated in ultrasound gel to eliminate air pockets. Each product underwent a CT scan (Somatom Definition AS; Siemens AG, Germany; 1 s gantry rotation time, 128×0.6 mm section collimation using a z flying focal spot, and 601 reference milliampere-second tube current with automatic exposure control at a tube voltage of 120 kV) and a flat panel CT scan (DynaCT Head, Artis Zeego, Siemens AG, Germany; 10 s rotation time, 70 kV).
Objective evaluation of artifacts
Objective evaluation of artifacts was performed on axial and longitudinal planes. The methodology was similar for CT and flat panel CT acquisitions.
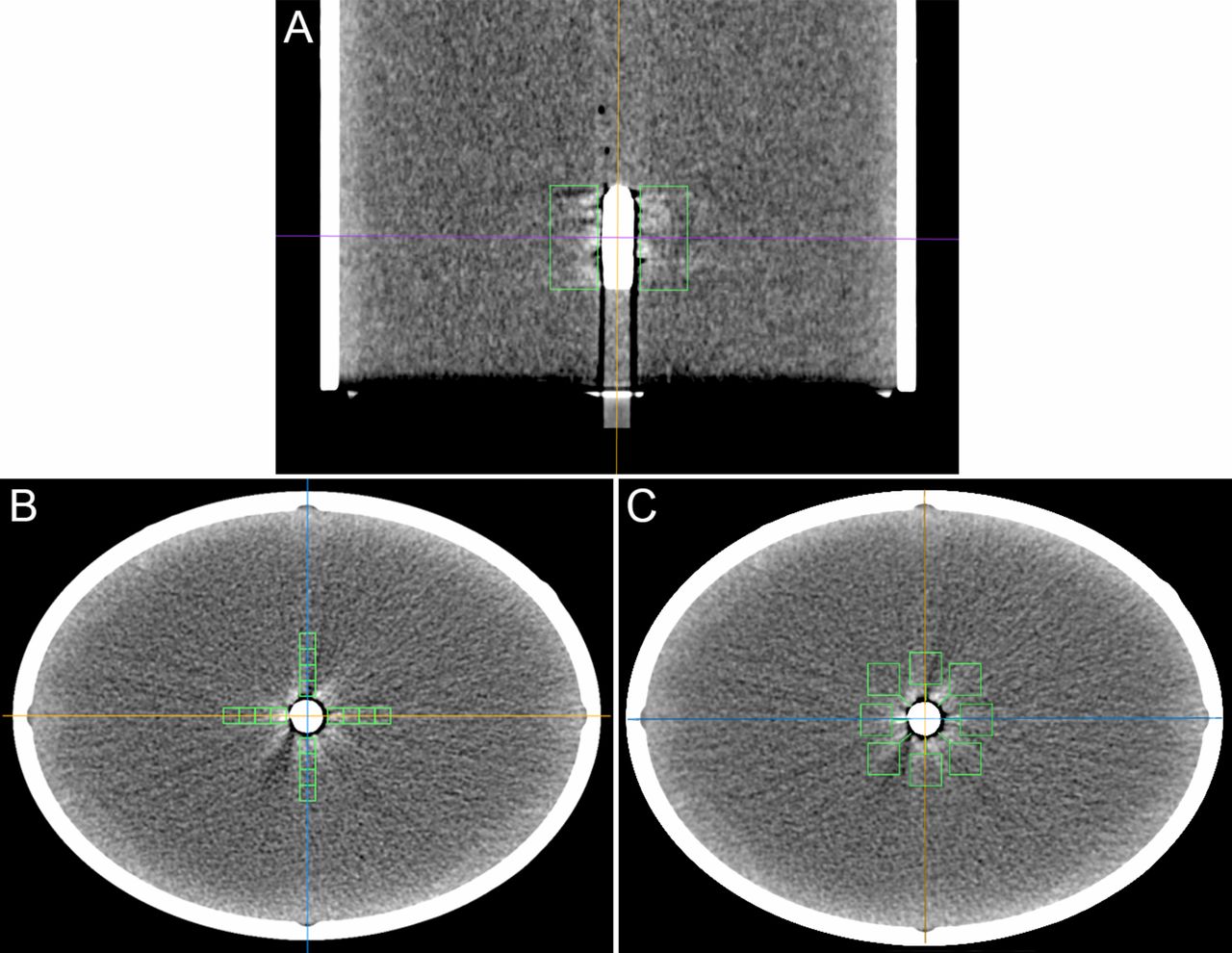
In the axial plane, one representative axial image was generated using multiplanar reconstructions. A 1 mm thick slice was placed in the middle of the embolic cast, perpendicular to the long axis of the test tube (see figure 1A). On this axial image, regions of interest (ROIs) measuring 0.5×0.5 cm were placed concentrically on the vertical and horizontal axis at a distance of 0 cm, 0.5 cm, 1 cm, and 1.5 cm from the embolic material respectively (see figure 1B).

Evaluation of artifacts. (A) A representative axial image was generated on multiplanar reconstructions—1 mm thick slice placed in the middle of the embolic cast, perpendicular to its long axis. In addition, 1.5 cm wide regions of interest (ROIs) were placed on each side of the embolic material in coronal and sagittal planes. (B) On the axial image, 0.5×0.5 cm ROIs measuring 0.5×0.5 cm were placed concentrically on the vertical and horizontal axis at distances of 0 cm, 0.5 cm, 1 cm, and 1.5 cm from the embolic material. ROIs from (A) and (B) were used for objective artifact quantification. (C) For subjective evaluation of artifacts, eight ROIs measuring 1×1 cm were placed at a distance of 0.5 cm around the embolic material.
For longitudinal planes, one ROI was placed on each side of the embolic material both in coronal and sagittal reconstructions (total of four longitudinal ROIs per product, ROI length equivalent to the length of the embolic cast, ROI width 1.5 cm) (figure 1A).
The range of Hounsfield unit (HU) values in the ROI was defined as the difference in maximal and minimal values; noise was defined as the SD of HU values in the ROI. Images were processed using Horos software V.3.1.2 (Horosproject.org).
Subjective evaluation of CT artifacts
Subjective evaluation of artifacts was performed using one representative axial image for each product. The methodology was similar for CT and flat panel CT acquisitions.
The images were reviewed in soft tissue window (CT—window level 20 HU, window width 90 HU; flat panel CT— window level 40 HU; window width 400 HU). Eight ROIs measuring 1×1 cm were placed at a distance of 0.5 cm around the embolic material (figure 1C). Two readers (reader 1 was a diagnostic neuroradiologist with 15 years of experience and reader 2 was an interventional neuroradiologist with 23 years of experience) performed a blinded interpretation of images quantifying artifacts in each of the eight ROIs using a five point Likert scale9 (1=severe artifacts, largely not diagnostic; 2=poor image quality, partly non-diagnostic; 3=moderate image quality, limited diagnostic confidence; 4=good image quality, sufficient for diagnosis; and 5=excellent image quality, no artifacts). ROIs with a score of 1 or 2 were considered non-diagnostic; ROIs scoring 3–5 were considered diagnostic. Inter-rater agreement for the diagnostic value of ROIs was quantified between the two readers. The proportion of non-diagnostic ROIs for reader 1 was compared between Onyx 18 and each of the four Squid products.
Statistical analysis
Continuous variables are presented as median (range) and compared using the Mann–Whitney test after assessment of the normality of the distribution. Categorical variables are presented as numbers (percentages) and compared using the Fisher exact test. Inter-rater agreement was calculated using raw statistics, and the reliability of the agreement was analyzed using Cohen k coefficient. Statistical data were analyzed using GraphPad Prism V.6.0 (GraphPad Software, La Jolla, California, USA) and SPSS software V.20.0 (IBM Corp, Armonk, New York, USA). The significance level was established at P<0.05.
Results
The representative axial images for each product are displayed in figure 2 (CT images) and figure 3 (flat panel CT images).
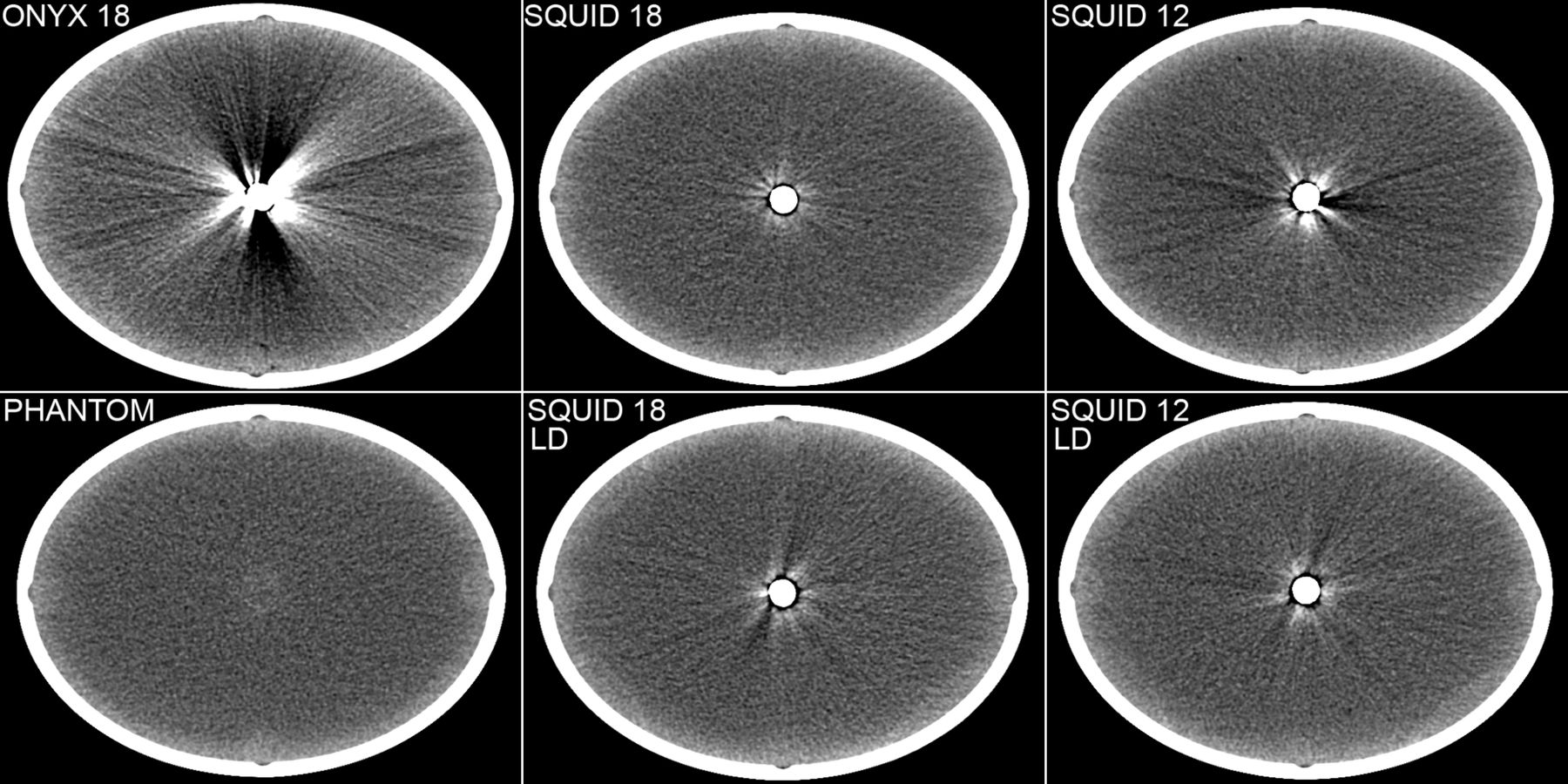
Representative axial CT images.

Representative axial flat panel CT images.
Objective evaluation
On CT and flat panel CT images, for both axial and longitudinal ROIs, noise and HU range values were significantly lower for all Squid products (Squid 18, Squid 18 LD, Squid 12, and Squid 12 LD) compared with Onyx 18.
When grouping axial ROIs according to distance from the embolic product (at 0 cm, 0.5 cm, 1 cm, and 1.5 cm), noise and HU range values for Squid 18 and Squid 18 LD were significantly lower than that for Onyx 18 at all points. For Squid 12 and Squid 12 LD, most values were significantly lower except in a few areas where, although numerically lower, the difference failed to reach statistical significance.
On both CT and flat panel CT, LD variants of Squid 18 and Squid 12 had significantly lower noise and HU range values than their normal density counterparts on longitudinal ROIs. On axial ROIs the difference was not statistically significant. There were no significant differences between Squid 18 and Squid 12, although values for Squid 18 were numerically lower.
The data are detailed in the online supplementary tables 1–6. Figure 4 illustrates the differences in median values of noise and HU range for axial and longitudinal ROIs on CT images. The online supplementary figure 1 illustrates differences at respective concentric points on axial CT images.
Supplemental material

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Median values of noise and Hounsfield unit (HU) range for axial and longitudinal regions of interest (ROIs) on CT images. LD, low density.
Subjective evaluation
On CT images, the number of non-diagnostic ROIs was significantly higher for Onyx 18 (7/8 ROIs) than for Squid 18 (0/8, P=0.001), Squid 18 LD (0/8, P=0.001), Squid 12 (1/8, P=0.01), and Squid 12 LD (0/8, P=0.001).
On flat panel CT images, the number of non-diagnostic ROIs was significantly higher for Onyx 18 (8/8 ROIs) than for Squid 18 (1/8, P=0.001), Squid 18 LD (2/8, P=0.007), Squid 12 (2/8, P=0.007), and Squid 12 LD (2/8, P=0.007).
Inter-observer agreement for diagnostic value of ROIs was excellent on CT images (overall agreement 95%, Cohen k=0.84, P<0.005) and slightly lower on flat panel CT images (overall agreement 90%, Cohen k=0.79, P<0.005).
Discussion
In this experimental phantom study, Squid embolic agents were associated with fewer artifacts than Onyx on CT and flat panel CT acquisitions.
In particular, there was a significant difference between Onyx 18 and Squid 18, despite the fact that the two products allegedly contain similar quantities of EVOH (6%), DMSO, and tantalum powder. Moreover, initial experience demonstrated similar behavior of the two products during embolizations in a clinical setting.10 According to the Squid and Onyx product brochures, the main difference is the smaller size of tantalum particles in Squid products. However, it must be said that the quantity and size of tantalum particles are not specified in the two brochures. Additionally, the exact percentage of EVOH is not listed in the Squid brochure.
The smaller size of tantalum particles could influence the formation of beam hardening artifacts in two ways. First, the smaller size of the particles should lead to improved distribution of tantalum within a given volume of solution. Smaller and more evenly distributed particles could lead to less X-ray diffraction and thus reduced beam hardening artifacts.
Second, smaller particle size leads to prolonged suspension of the tantalum powder in the embolic solution. A recent article11 quantified the speed of tantalum deposition once the vials of embolic agent are taken out of the agitator. During 30 min of observation, sedimentation in Onyx 18 occurred nearly three times faster compared with Squid 18 and 1.5 times faster compared with Squid 12. Given that in a clinical setting injections can last up to 45 min or longer,12 we can assume that by the time it precipitates, Onyx will contain more areas of concentrated tantalum powder as a result of faster deposition. Concentration of tantalum in certain areas of the embolic cast leads to an exponential local increase in radiopacity and subsequently to more beam hardening artifacts.
Differences between Squid variants
As a secondary finding, we observed differences in artifacts between the four variants of Squid. Squid 12 is a low viscosity variant of Squid 18; it contains less EVOH (4%) which leads to slower precipitation and facilitates deeper penetration in small caliber, tortuous vascular networks. LD variants of Squid 18 and Squid 12 contain 30% less tantalum powder compared with their normal density homologue, in order to reduce radiopacity without influencing embolic properties. As expected, because they contain less radiopaque material, Squid 12 LD and Squid 18 LD induced fewer artifacts than normal density counterparts.
Although not statistically significant, there were numerically more artifacts for Squid 12 compared with Squid 18 on both subjective and objective measurements. This could be partially explained by differences in tantalum deposition rates; the aforementioned study11 found that tantalum deposition occurs almost twice as fast in Squid 12 than in Squid 18. Moreover, as Squid 12 contains less EVOH, the final embolic cast should be slightly smaller in volume but containing the same amount of tantalum. This should result in slightly higher radiopacity and thus more artifacts.
Clinical implications of fewer artifacts
In clinical practice, an embolic agent that induces fewer artifacts has two main advantages. First, reduced artifacts should improve the diagnostic accuracy of hemorrhagic or ischemic complications on post-embolization CT and flat panel CT imaging. In particular, flat panel CT acquired with angiography systems is becoming increasingly useful for early peri-interventional detection of such complications.13
Second, we can hypothesize that performing embolizations with a product which induces less artifacts might improve the results of subsequent stereotactic radiosurgery. Numerous papers have documented reduced nidus obliteration rates for radiosurgery in patients with partially embolized cerebral arteriovenous malformations.14 15 This might be explained at least in part by a reduction of effective dose to the nidus because of absorption or scattering of the radiation beams due to the embolic material16 and by difficulties in target delineation as the embolic material may obscure parts of the nidus.16 17 Given the similarities between the physical mechanism of beam hardening artifacts and absorption/scattering during radiosurgery, we can extrapolate that Squid and especially Squid LD variants might be associated with better nidus obliteration rates after stereotactic radiosurgery. However, further research is needed to confirm this hypothesis.
Limitations
The main limitation of the present study pertains to the experimental setting. Injection of embolic products in a test tube cannot reproduce the complexity of diffusion along the blood flow in a vascular network under varying pressures both at distal and proximal extremities. However, this controlled simplified environment was necessary in order to ensure reproducibility of conditions between the different products tested. Another limitation is the lack of sufficient clinical data to support these experimental findings. Our current clinical experience with Squid is insufficient for a compelling comparison of artifacts and other characteristics.
Conclusion
In this experimental phantom study, all Squid embolic agents were associated with fewer beam hardening artifacts than Onyx 18 on CT and flat panel CT acquisitions. The reduction in artifacts is probably explained at least in part by the smaller size of tantalum particles which leads to better distribution within the embolic solution and decreased speed of sedimentation.
Acknowledgments
The authors are grateful to Mourad Bouhadjar, Gael Fourré, Manon Bequart and the entire team of radiology technicians at IHU Strasbourg Institute, for their valuable assistance in performing the experimental procedures.
References
Footnotes
Twitter @RaoulPop25
Contributors RP: conception or design of the work; acquisition, analysis, and interpretation of the data; drafting the work; final approval of the version to be published; and agreement to be accountable for all aspects of the work. LM: conception or design of the work; analysis and interpretation of the data; revision of the paper for important intellectual content; final approval of the version to be published; and agreement to be accountable for all aspects of the work. AI: acquisition of the data; analysis of the data; revision of the paper for important intellectual content; final approval of the version to be published; and agreement to be accountable for all aspects of the work. DM: acquisition of the data; revision of the paper for important intellectual content; final approval of the version to be published; and agreement to be accountable for all aspects of the work. JSR: acquisition of the data; revision of the paper for important intellectual content; final approval of the version to be published; and agreement to be accountable for all aspects of the work. MM: acquisition of the data; revision of the paper for important intellectual content; final approval of the version to be published; and agreement to be accountable for all aspects of the work. SK: analysis and interpretation of the data; revision of the paper for important intellectual content; final approval of the version to be published; and agreement to be accountable for all aspects of the work. RB: conception or design of the work; interpretation of the data; revision of the paper for important intellectual content; final approval of the version to be published; and agreement to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.