Article Text

Abstract
Background and purpose Intrasaccular flow disruption using the Woven EndoBridge (WEB) is a safe and effective method to treat intracranial aneurysms, particularly wide neck bifurcation aneurysms. However mid term and long term follow-up imaging can show aneurysm remnant or recanalization, and retreatment is therefore sometimes necessary. In most cases, retreatment is performed using an endovascular approach. The present series reports and analyzes aneurysm clipping of recanalized or incompletely occluded aneurysms following WEB treatment.
Methods All patients treated with the WEB device since the beginning of our experience in June 2011 were prospectively collected in a local database. Among them, patients who were retreated by clipping for aneurysm remnants were included in the present series.
Results In the cumulative population of 130 patients with aneurysms treated by the WEB device from June 2011 to February 2019, 4 patients (3.1%) were retreated with surgical clipping due to incomplete occlusion (2 patients) and aneurysm recanalization (2 patients). Three of the four aneurysms retreated (75%) were located in the middle cerebral artery and one in the anterior communicating artery (25.0%). The aneurysm was ruptured in 1 of 4 patients (25%). Clipping was performed 10–54 months after initial treatment with the WEB. Surgical exposure showed that the WEB device was inside the aneurysm sac in all cases. Clipping was easily performed in all but 1 case. Control DSA showed complete occlusion in two aneurysms and a neck remnant in two.
Conclusion Clipping is a feasible option for treating aneurysm remnants following initial treatment with intrasaccular flow disruption using the WEB.
- aneurysms
- WEB device
- clipping
- endovascular treatment
- flow disruption
Statistics from Altmetric.com
Introduction
Endovascular treatment is the firstline treatment for intracranial aneurysms but it still has some limitations, including complex aneurysms (large and giant, and wide neck aneurysms) and recanalization.1–4 Because of these limitations, innovative treatments have been developed, singularly flow diversion and flow disruption.3–21 Flow disruption consists of placement of a device in the aneurysm sac that will disrupt the flow at the level of the neck, creating an intrasaccular (and intra-device) thrombosis. As of now, only the the Woven EndoBridge (WEB) device is available for this clinical application. Other devices have been evaluated (Luna/Artisse, Medtronic, Irvine, California, USA) but are not clinically available.22
In contrast with flow diversion (placement of a dense mesh stent in the parent artery in front of the aneurysm neck), flow disruption is not associated with placement of any material in the parent artery. For this reason, dual antiplatelet treatment is not needed and the WEB can be used for the treatment of unruptured and ruptured aneurysms.
Flow disruption with the WEB has a high safety profile, as shown in the Good Clinical Practice (GCP) studies conducted in Europe and the USA.20 23 In the recent analysis of the cumulative populations of the three European GCP studies, morbidity at 30 days was 3.0% (related to the device or the procedure in 1.2%) whereas mortality was 0.0%.20 Similar results were observed in the WEB-IT study conducted in the USA with 30 day morbidity of 0.7% and no mortality.23 Similar results were also reported in large single center series.24 25
WEB aneurysm treatment results in good effectiveness outcomes at 1 year, with complete aneurysm occlusion in 52.9% and adequate occlusion (complete occlusion with neck remnant) in 79.1%.20 Despite this good efficacy, aneurysm remnants or aneurysm recanalization can be observed in the follow-up period and retreatment is sometimes necessary. In the three European GCP studies, the rate of retreatment at 1 year was 6.9%; various endovascular retreatment modalities, including stent assisted coiling, flow diverter, WEB, WEB+stent, and stent, were used in these studies. Open surgical clipping, however, was not used for retreatment. In a recent series dedicated to the treatment strategies for recurrent and residual aneurysms after WEB treatment, several modalities were also reported, but not clipping.26
Recanalized aneurysms after coiling may also be treated with various endovascular options in addition to clipping.27 28 The use of clipping in cases of recanalized aneurysms initially treated with the WEB has only been reported in a case report.29
Here we describe a series of four patients with recanalized aneurysms after WEB treatment retreated with clipping. The aim of this report is to analyze the surgical findings, feasibility, potential difficulties, and the safety of this approach.
Materials and methods
According to French law, retrospective studies do not have to be submitted to an ethics committee for approval and written informed consent was waived.
Patients
A database that includes all patients with aneurysms treated in the Interventional Neuroradiology Department, Reims University Hospital, is maintained prospectively. All patients treated with a WEB device were extracted and those having a recanalized aneurysm or aneurysm remnant treated with clipping were analyzed. In our center, treatment decisions for ruptured, unruptured, and recanalized aneurysms are made by a local multidisciplinary team that includes neurosurgeons and neuroradiologists. In this series, the initial decision for treatment with a WEB device as well as the decision for retreatment by clipping was made by the same multidisciplinary group.
WEB device
The WEB is a self-expanding, retrievable, electrothermally detachable, nitinol braided device, which is placed within the aneurysm sac. There have been several WEB device iterations over time. The WEB DL was initially used and contains a second nitinol braid. From November 2013, the WEB DL was replaced by a WEB with a single braid (WEB SL and WEB SLS have a barrel and a spherical shape, respectively). The most recent evolution of the device has been enhanced visualization (WEB EV) that incorporates composite wire strands made from nitinol and platinum. In parallel, the microcatheters used to deliver these devices have changed with progressive reductions in size, from 27 to 17 microcatheters.
WEB procedure
WEB procedures were performed under general anesthesia and heparin. In ruptured aneurysms, no antiplatelet treatment is given before or during the procedure. In unruptured aneurysms, the protocol evolved with time. Initially, no antiplatelet treatment was given before the WEB procedure and IV aspirin was given during the procedure. Over time, premedication with clopidogrel (Sanofi-Aventis, Gentilly, France) for 5 days or subsequently ticagrelor (AstraZeneca, Courbevoie, France) for 2 days was used as wide necked aneurysms treated were frequently associated with thromboembolic complications, and because stent assisted coiling is a potential alternative in this subgroup of patients.
Clipping procedure
Clipping procedures were performed under general anesthesia. The head was placed in a three pin skull fixation device attached to the table to stabilize the head position during surgery. A craniotomy was made in the skull after skin incision (bone flap lifted and temporally removed). The dura was opened to expose the brain. Retractors gently opened a surgical corridor to locate the artery and follow it to the aneurysm under microscopic control. Intraoperative indocyanine green angiography was performed for all patients before and after the clipping procedure. The clip (Yasargil Aneurysm Clip System, Aesculap AG, Tuttlingen, Germany) was held open with a tweezer-like applier and placed across the aneurysm neck. Once released, the jaws of the clip closed, pinching off the aneurysm and WEB device from the parent artery. Multiple and temporary clips were used when necessary.
Data collection
The following data were collected:
Patient: age and gender.
Aneurysm: location, status (ruptured/unruptured), size (before WEB treatment), and neck size.
WEB procedure: date, type, and size of device used, complications if any, and use of additional device.
Follow-up imaging after WEB procedure: date, imaging type (MR angiography or DSA), and aneurysm occlusion.
Clipping procedure: date, WEB location (in the aneurysm, in the subarachnoid space, or in both), type and number of clips, need to remove the WEB, and complications.
Follow-up imaging after clipping procedure: date, imaging type (MR angiography or DSA), and aneurysm occlusion. Aneurysm occlusion was evaluated using a three grade scale: complete occlusion, neck remnant, and aneurysm remnant.
Results
Patients and aneurysms
Patients, aneurysms, the Woven EndoBridge procedures, and clipping procedures
Of 130 patients treated from June 2011 to February 2019, 4 patients (3.1%) had recanalized aneurysms treated with surgical clipping (table 1). All patients were middle-aged women. Initial status of the recanalized aneurysms was ruptured in 1 (patient No 1) and unruptured in 3 (patient Nos 2, 3, and 4).
Aneurysm location was the anterior communicating artery (Acom) in one patient (patient No 1, figure 1) and the middle cerebral artery (MCA) in three patients (patient Nos 2, 3 and 4, figure 2). Aneurysm size (transverse diameter) was 5.6 mm (patient No 1), 6.8 mm (patient No 2), 7.4 mm (patient No 3), and 4.2 mm (patient No 4). Three aneurysms (patient Nos 1, 3 and 4) had a narrow neck (3.2 mm, 2.3 mm, and 3.8 mm) and one (patient No 2) a wide neck (5.5 mm).

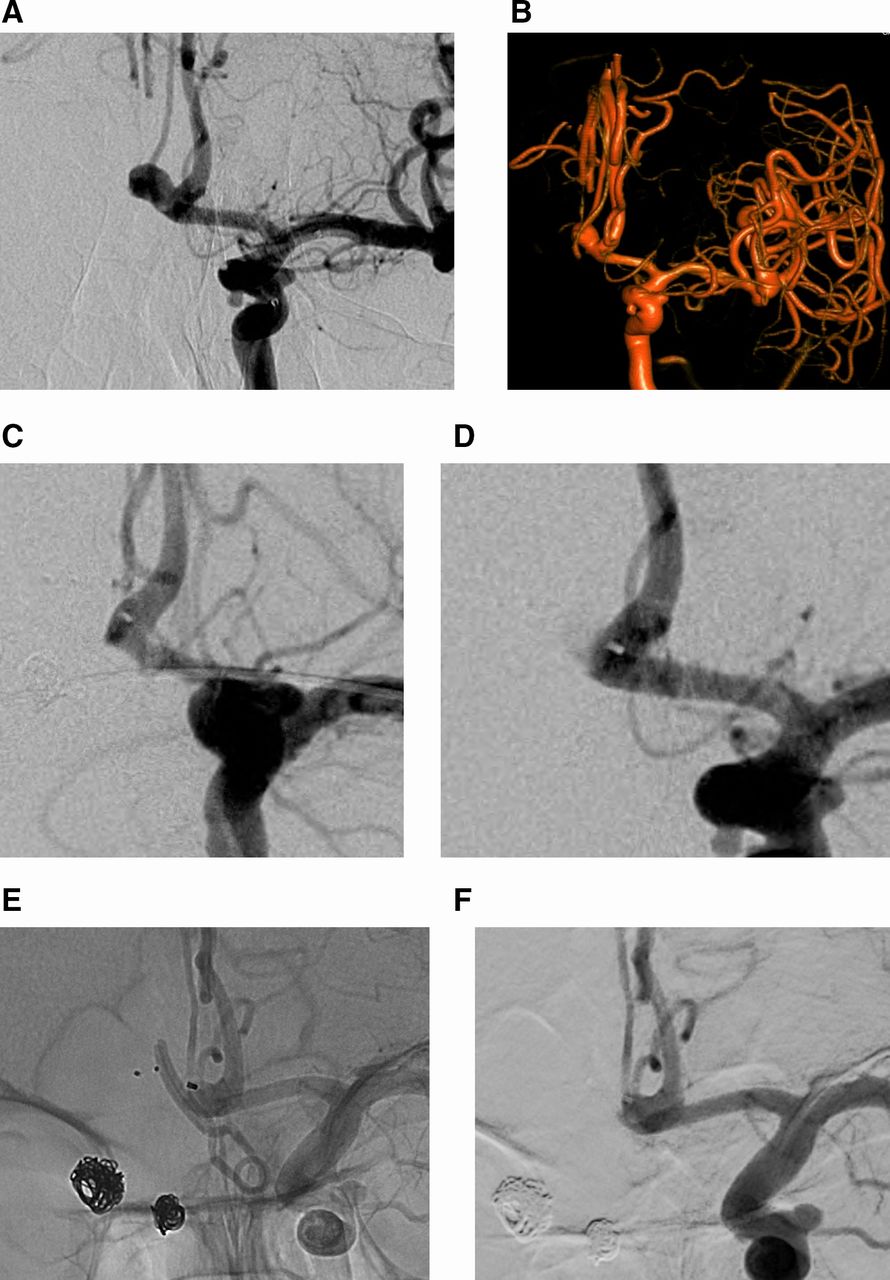
Ruptured left anterior communicating artery aneurysm. (A) DSA, working view. (B) Three-dimensional DSA shows the aneurysm (transverse diameter 5.6 mm; neck 3.2 mm). (C) DSA at the end of the Woven EndoBridge (WEB) procedure shows complete aneurysm occlusion. (D) DSA after 46 months shows detection of aneurysmremnant. (E, F) Twelve months after the clipping procedure, DSA control (unsubstracted and subtracted views).

{kind=link}
{kind=link}
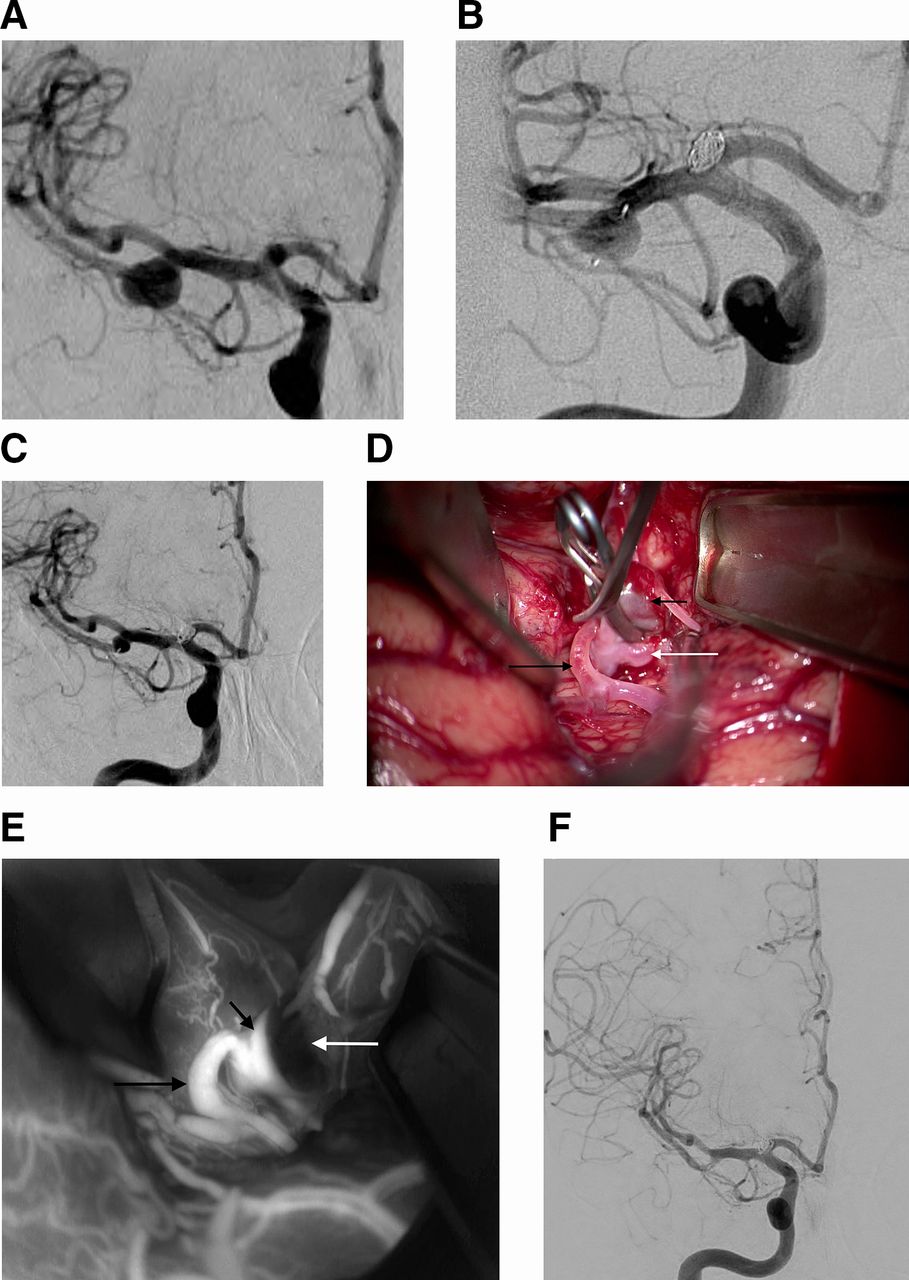
Unruptured right middle cerebral artery bifurcation aneurysm. (A) DSA, working view, shows the aneurysm (transverse diameter 7.4 mm; neck 5.5 mm). (B) DSA at the end of the Woven EndoBridge (WEB) procedure shows residual flow in the aneurysm (and the device). (C) DSA after 7 months shows an aneurysm remnant. (D) Intraoperative photograph (short black arrow: aneurysm sac, long black arrow: temporal branch of MCA, white arrow: MCA bifurcation) and (E) Peroperative ICG angiogram control (white arrow: thrombosis of aneurysm fundus) confirming aneurysm occlusion. (F) Six months after clipping, DSA shows complete aneurysm occlusion.
WEB procedure
One aneurysm was originally treated with a WEB DL and the three others with a WEB SL, without any additional device. The WEB procedures were uneventful. One patient (patient No 1) had a thromboembolic complication during the simultaneous treatment of another aneurysm. At the end of the WEB procedures, DSA showed complete occlusion in patient No 1, slight residual flow in the device and the aneurysm in patient No 2, and residual flow in patient Nos 3 and 4.
Follow-up after WEB treatment
For patient No 1, the 13 month DSA and 32 month MR angiography showed stable complete aneurysm occlusion. An aneurysm remnant was detected on DSA at 46 month. For patient No 2, an aneurysm remnant was depicted on DSA after 8 months and was increasing in size on DSA after 14 months. For patient No 3, a neck remnant was depicted on the 3 month MR angiogram and became an aneurysm remnant on DSA at 7 months. For patient No 4, the aneurysm remnant was depicted on the 6 month DSA and persisted on the 14 month DSA.
Indication for treatment
In the four cases, indications for retreatment were decided by the multidisciplinary group (neurosurgeons and interventional neuroradiologists). The decision for retreatment was made because there was an aneurysm remnant in all patients, two of which were growing between two imaging controls (patient Nos 2 and 3). Endovascular techniques (including stent assisted coiling and flow diversion) were considered inappropriate given the shape and location of the remnant, and clipping was decided.
Surgical procedure
Surgical procedures were performed 54 months (patient No 1), 16 months (patient No 2), 11 months (patient No 3), and 28 months (patient No 4) after the WEB procedure. The procedure was performed via a fronto-pterional approach for MCA aneurysms and a fronto-orbital approach for Acom aneurysms with use of the microscope. The aneurysm was dissected, thus avoiding the use of permanent retraction. The WEB device mesh was detected through the thin transparent aneurysm wall for all patients and aneurysm neck was noted to be flowing with a red/pink color and a vascular pulsation. There was no protrusion of the flow disrupter device into the subarachnoid space in the four cases, a phenomenon detected in previously coiled aneurysms. The device did not modify aneurysm wall thickness.
The WEB device was easily compressible inside the aneurysm sac due to low radial force. There was no need to remove the WEB device from the aneurysm sac during the surgical procedure. In the first, second, and fourth patients, only one clip was placed at neck level and the WEB device was not included in the clip (one straight and one curved clip).
With the third patient, one clip was initially placed at the level of the neck, but did not completely suppress the flow inside the remnant aneurysm. The aneurysm sac volume with the WEB device inside pushed the clip closed in efferent arteries. A second curved clip was placed in the proximal part of the WEB device, using the first clip as a guide. This facilitated correct placement of the second clip with the WEB device. The first clip was removed after placing the second clip.
In the fourth patient, placement of the clip was slightly difficult due to the position of the proximal marker of the device in the parent artery. Placing the clip was associated with a slight displacement of the proximal marker of the WEB, associated with shape modification of the parent artery (angulation). Clipping the aneurysm without mobilizing the proximal marker was obtained by the use of three different clips: two temporary clips in the anatomical neck to maintain the marker on the right position and one definitive clip at the junction between the surgical neck and the proximal part of the WEB.
No patient complications were reported during the clipping procedures.
Follow-up after clipping procedure
Control DSA was obtained 12 months (patient No 1), 2 days (patient No 2), 6 months (patient No 3), and 4 months (patient No 4) after clipping. In patient Nos 3 and 4, the aneurysm was completely occluded. In patient Nos 1 and 2, a neck remnant was visible.
Discussion
This small single center series provides two important pieces of information regarding WEB aneurysm treatment. First, in both ruptured and unruptured aneurysms reported in the present series, open surgical visualization showed that the device was within the aneurysm sac and not in the subarachnoid space. Second, this series showed that aneurysm clipping is feasible in the event of aneurysm recanalization after WEB treatment.
WEB aneurysm treatment has been proven to be a safe endovascular modality in treating complex aneurysms, particularly wide neck bifurcation aneurysms, in the four prospective, independently adjudicated GCP studies conducted in Europe and the USA.20–23 Morbidity and mortality at 1 month in the cumulative population of the three European GCP studies were 3.0% and 0.0%, respectively, and very similar results were reported in the US trial (0.7% and 0.0%, respectively). As shown in the three European GCP studies, WEB treatment also demonstrated good efficacy with adequate occlusion (complete occlusion and neck remnant) in 79.1% of patients at 1 year following treatment.
With the increasing number of patients with intracranial aneurysms treated with the WEB device, it is not surprising to observe some aneurysm remnant or recanalization during follow-up. In the three European GCP studies, aneurysm remnants were reported in 20.9% of aneurysms treated with the WEB.20 In the same population, the rate of aneurysm retreatment at 1 year was 6.9%. Indications for retreatment of previously treated aneurysms are still a matter of debate and have to be decided based on the potential risk of rebleeding of the remnant. The CARAT study has shown that the rebleeding risk for previously ruptured aneurysms was directly related to the degree of occlusion: 1.1% for complete occlusion, 2.9% for 91–99% occlusion, 5.9% for 70–90%, and 17.6% for <70%.30 Based on these results, the most current strategy (at least in Europe) is to leave neck remnants untreated and to follow them with MR angiography or CT angiography. If the neck remnant is changing in shape or increasing in size, or in the case of an aneurysm remnant, a retreatment strategy is considered and discussed.
Retreatment modalities depend on several factors, including the way the aneurysm was initially treated, its location, its size, the feasibility of surgery, and the different endovascular approaches available. For aneurysms initially treated with the WEB, the way aneurysms are retreated varies. In the three GCP European series, retreatment was performed with stent and coils in four aneurysms, flow diverters in four, stent in one patient, the WEB and stent in one patient, and the WEB in one patient. Similar modalities were reported in a recent series dealing with retreatment of aneurysms initially treated with the WEB.24 This great heterogeneity of treatment modalities shows that these recanalized aneurysms are not easy cases for retreatment due to their location and shape, and no single modality of retreatment can appropriately address all of the cases.
Recanalized aneurysms after initial coiling are sometimes retreated by clipping.27 28 As outlined by Nisson et al, previously coiled aneurysms are more resistant to manipulation than untreated aneurysms and can be challenging to treat in narrowly accessed anatomic corridors.27 In addition, clip blades can slide down to the tip of these coils jeopardizing encroachment of the lumen of the parent vessel, particularly when the coils extend out of the aneurysm and into the parent vessel, necessitating coil extraction from the aneurysmal sac. In the series by Nisson and colleagues, manipulation of coils before clipping was necessary in 19% of aneurysms. In a systematic review of the literature, coil extraction was reported in a similar percentage of cases (13%).28 In this review, clipping of previously coiled aneurysms was associated with a high rate of angiographic cure (93%) at the price of a relatively high morbidity and mortality (9.8% and 3.6%, respectively).
In contrast to that reported by Nisson et al for coiled aneurysms, it seems from our preliminary experience in this series that clipping of aneurysms treated with the WEB is not as challenging and is associated with good safety (no mortality or morbidity) outcomes. It is probably explained by several factors: (1) as shown in the present series, surgical visualization of the aneurysm did not show that the device was in the subarachnoid space, even in the case of ruptured aneurysms; (2) according to the shape of the device and owing to the fact that its proximal surface is flat, there seems to be less risk of having part of the device in the neck or even in the parent vessel; however having the proximal marker present in the aneurysm bifurcation can create some technical difficulties for clipping (as was the case with patient No 4); and (3) the WEB device, which has very limited radial force and can be easily compressed by the clip blades, is less likely to have surgical clips slip as they would over compacted coils, as described in the series by Nisson et al 25 Similar observations were reported in the only case report of a recanalized Acom aneurysm after WEB treatment.27 In our series, adequate occlusion (complete occlusion or neck remnant) was obtained in all cases, but with neck remnant in two cases. This result confirms the specific complexity of treatment of this subgroup of aneurysms in which WEB treatment is indicated.
Conclusion
In a context where the WEB device is increasingly used for the treatment of both ruptured and unruptured intracranial aneurysms, this preliminary series shows that, after its placement in the aneurysm sac, the WEB device is not migrating in the subarachnoid space in unruptured or ruptured aneurysms. In the case of recanalization of aneurysms initially treated with the WEB, clipping is a feasible option, among others, to treat the remnant.
References
Footnotes
Contributors All authors have: provided a substantial contribution to the conception and design of the studies and/or the acquisition and/or the analysis of the data, and/or the interpretation of the data; drafted the work or revised it for significant intellectual content; approved the final version of the manuscript; and agree to be accountable for all aspects of the work, including its accuracy and integrity.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests LP is a consultant for Balt, MedTronic, Microvention, Penumbra, and Vesalio.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.