Article Text

Abstract
Background Rapid development in endovascular aneurysm therapy continuously drives demand for suitable neurointerventional training opportunities.
Objective To investigate the value of an integrated modular neurovascular training environment for aneurysm embolization using additively manufactured vascular models.
Methods A large portfolio of 30 patient-specific aneurysm models derived from different treatment settings (eg, coiling, flow diversion, flow disruption) was fabricated using additive manufacturing. Models were integrated into a customizable neurointerventional simulator with interchangeable intracranial and cervical vessel segments and physiological circuit conditions (‘HANNES’; Hamburg ANatomic Neurointerventional Endovascular Simulator). Multiple training courses were performed and participant feedback was obtained using a questionnaire.
Results Training for aneurysm embolization could be reliably performed using HANNES. Case-specific clinical difficulties, such as difficult aneurysm access or coil dislocation, could be reproduced. During a training session, models could be easily exchanged owing to standardized connectors in order to switch to a different treatment situation or to change from ‘treated’ back to ‘untreated’ condition. Among 23 participants evaluating hands-on courses using a five-point scale from 1 (strongly agree) to 5 (strongly disagree), HANNES was mostly rated as ‘highly suitable for practicing aneurysm coil embolization’ (1.78±0.79).
Conclusion HANNES offers a wide variability and flexibility for case-specific hands-on training of intracranial aneurysm treatment, providing equal training conditions for each situation. The high degree of standardization offered may be valuable for analysis of device behavior or assessment of physician skills. Moreover, it has the ability to reduce the need for animal experiments.
- aneurysm
- angiography
- catheter
- intervention
- technique
Statistics from Altmetric.com
Introduction
With an approximate prevalence of 2–4% in the general population, intracranial aneurysms (IAs) are a common finding. Lethal aneurysmal subarachnoid hemorrhage, in the majority of cases caused by small IAs,1 is a major concern as most affected patients require emergency treatment.2 3 In recent years, neuroendovascular treatment has become the favored approach for many ruptured and unruptured IAs.4 As endovascular aneurysm treatment is a rapidly developing field, it offers a wide range of distinct neurointerventional devices for long-term aneurysm occlusion.5–7 For neurointerventionalists just starting, apart from the required anatomic and clinical knowledge, understanding of the angiography system as well as the applied materials is necessary and technical skills in handling the equipment need to be acquired.8 Interdependence between technical skills and clinical expertise has been proved in various settings, and artificial training environments have been shown to enhance handling and safe use of distinct microcatheters and microwires.9 10 Moreover, familiarization with new techniques or practice with less frequently encountered pathology can be realized using artificial training environments.5 6 Available training modalities consist of animal models, computer-based angiography simulators, and synthetic vascular models.8 The recent advance in 3D printing technology and its implementation in the medical field offer enriching opportunities.11–13 The benefit of 3D-printed hollow aneurysm models based on real patients’ anatomy in perioperative training settings has been observed previously,11 14 15 and exact replicas of difficult human anatomies can help in planning of the surgical approach and may improve operator familiarity with new endovascular devices.16 Additionally, such models provide an opportunity to imitate specific intraoperative challenges, subsequently aiming to assess alternate treatment options.16 17
With the increasing availability of additive manufacturing techniques as a highly versatile tool for obtaining detailed vascular models,11 16 we aimed to develop a demonstrator of an integrated neurovascular training environment with the key features of patient-specific, rapidly exchangeable intracranial and cervical vessel modules, near-physiologic flow conditions, and a complete femorocranial vascular access route (‘HANNES’; Hamburg ANatomic Neurointerventional Endovascular Simulator). Physicians participating in neurointerventional hands-on training courses in our department were asked about their neurointerventional experience with HANNES and a simplified interventional training setup (‘SITS’; Simplified Interventional Training Setup). Our aim was to assess the value of an integrated modular neurovascular training environment for aneurysm embolization using 3D-printed aneurysm models. We hypothesized that working on HANNES provides numerous advantages and is thus better than an ordinary neurointerventional training setup.
Methods
Patient data and aneurysm models
We designed a single-center study with waived individual consent. Research was approved by the local ethical committee at Medical Chamber Hamburg, Germany. Twenty-nine patients with 30 IAs comprising different dimensions and anatomic locations were retrospectively identified. Existing clinical 3D rotational angiography data (AlluraClarity FD 20/20 angiography system, Philips Healthcare, Best, The Netherlands) were used for additive fabrication of hollow aneurysm models, as described previously.11 Images were obtained with the following parameters: 220° rotation (5 s), 150 single frames at a frame rate of 30/s, 27 cm detector field of view, and 512 acquisition matrix. Reconstruction was conducted using an intermediate kernel with an isotropic voxel size (0.8 mm). Images were anonymized before exportation and data were processed using Analyze 11.0 (AnalyzeDirect, Inc., Overland Park, Kansas, USA) and CATIA V5 (Dassault Systèmes SA, Vélizy-Villacoublay, France). 3D hollow aneurysm models were manufactured using either a semitransparent (TangoPlus FLX930 27 Shore A) or an opaque material (Formlabs flexible photopolymer resin FLFLGR02) with wall thicknesses ranging from 1 to 2 mm. TangoPlus is a rubber-like material, characterized by its elasticity, whereas Formlabs is a slightly stiffer material, providing higher tear resistance. TangoPlus models are produced applying multi-jet modeling technology. Formlabs models are manufactured using a laser-based stereolithography 3D printer. Following the individualization standardized process according to Spallek et al,18 patient-specific aneurysm models can be designed easily at any time.
SITS before the implementation of HANNES
From October 2016 to November 2017, before the use of HANNES, training courses were performed with SITS using TangoPlus aneurysm models (3–5 cm length, omitting the thoracoabdominal and cervical vessels as well as the petrous segment of the internal carotid artery) connected to a silicone tube flow circuit. An external pump provided water for the system, operating at room temperature.
Experimental setup of HANNES
The newly developed integrated neurovascular training environment (HANNES) operates with a standardized silicone aorta, including the proximal femoral arteries used as angiographic access route and the main aortic branches. HANNES was used for training courses starting in December 2017. Several different carotid arteries (straight and curved) and intracranial aneurysm models derived from patient anatomy were manufactured, applying the Formlabs material. Using standardized quick-change adapters, cervical and intracranial anatomies can be exchanged easily to switch to a different treatment scenario. A standard skull-base completes the whole relevant vessel tree for neurointerventions. Near-physiological circuit conditions are provided by an integrated pump enabling an adjustable flow rate into the system, a pulsatile valve for creating a pulse adjustable between 0 and 150 bpm, a fluid reservoir, and a heating system for raising the fluid temperature up to 45°C. The standardized system configuration provides a water temperature of 37°C, a flow rate of around 0.4 L/min through the intracranial vessels, and a pulse rate of 70 bpm. As implementation of a silicone based aorta causes relatively high friction forces, the system pressure diverges slightly from physiologic conditions. A pulsating pressure gradient between 100 and 120 mmHg is achieved, resulting in a pulse shift of 20 mm Hg. HANNES presently makes it possible to perform aneurysm coil embolization, WEB and flow diverter placement under fluoroscopic control.
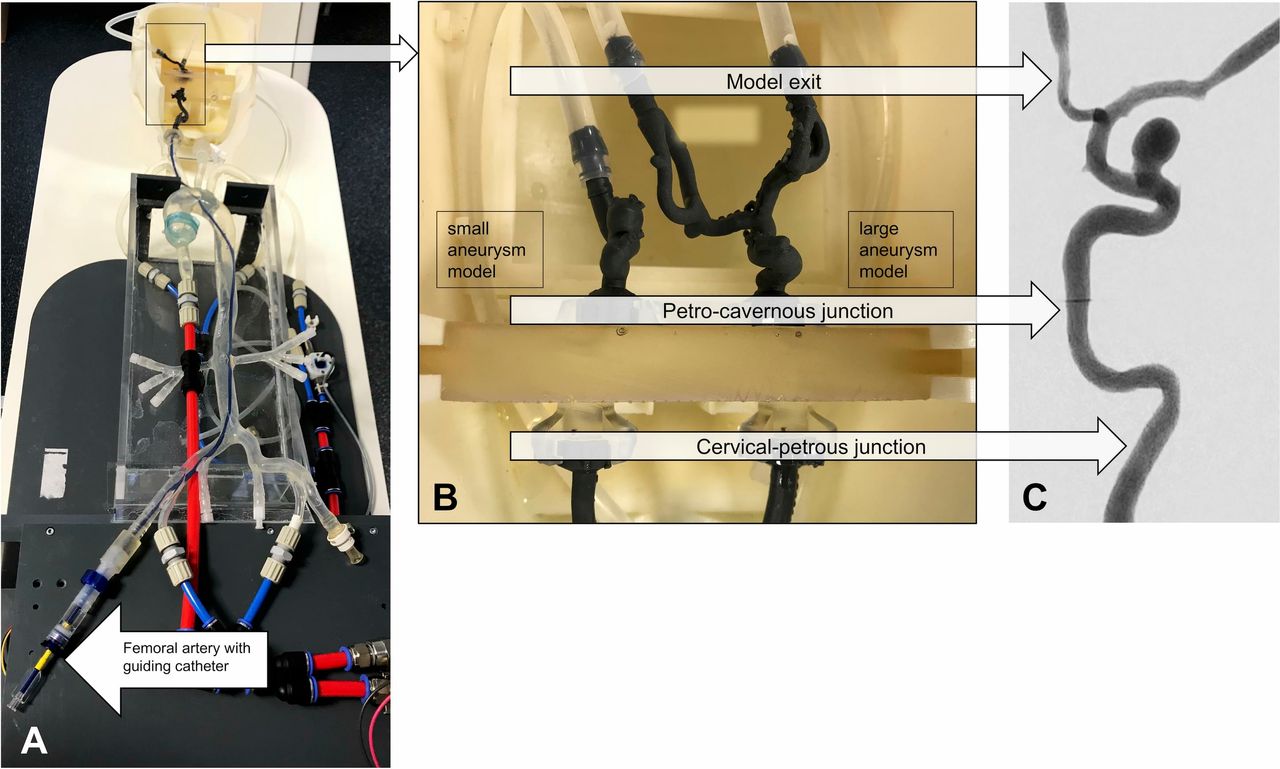
All training sessions were carried out in a research laboratory equipped with a fully featured angiography system (AlluraClarity FD 20, Philips Healthcare, Best, The Netherlands). Figure 1 illustrates the principal setup of HANNES as used during the training sessions.

HANNES setup. (A) Training setup of HANNES in the angiographic research laboratory; note the guiding catheter introduced into the femoral artery. (B) HANNES’ skull base offers the possibility of connecting two different cervical vessel anatomies and two aneurysm models simultaneously. Specially designed adapters facilitate model exchange; HANNES is designed with no inner edges at change positions. (C) DSA of a large aneurysm model as depicted in our experimental angiosuite.
In addition to rarely occurring aneurysm model perforations, we are aiming to develop an external aneurysm rupture simulation. Establishing a radiation-free training environment is another objective in progress.
Validation of microcatheter positioning
Outside training courses, microcatheter introduction and final positioning in aneurysm models were compared with clinical procedures in six models (‘L’, ‘I’, ‘B’, ‘M’, ‘P’, and ‘NLI’), using probability maps of 10 microcatheter insertions carried out by two operators (0 and 4 years of clinical expertise in interventional neuroangiography, respectively). Images from the corresponding clinical cases were compared with probability maps obtained with the model and independently rated by two neurointerventionalists for microcatheter positions using a three-point scale (1, near identical; 2, comparable; 3, not comparable).
Evaluation of SITS and HANNES
After each training course involving trainings on SITS and on HANNES, respectively, participants were asked to fill in questionnaires about their neurointerventional experience and perceived benefit of hands-on training with aneurysm models (see online supplemental questionnaire).
Supplemental material
Results
Aneurysm characteristics
A portfolio of 30 intradural aneurysm models derived from patient data was prepared. Patients presented either with incidental intracerebral aneurysms (n=21; 70%) or in the setting of subarachnoid hemorrhage (n=9; 30%) in our university neurovascular center between November 2011 and February 2016 (online supplemental table 1). Aneurysms were categorized with at least three instances according to each of the following categories: anatomical location according to the Unruptured Cerebral Aneurysm Study classification,19 endovascular treatment type and rupture state, resulting in a wide distribution of aneurysm characteristics across the entire portfolio. As the primary target was to provide a training environment for coil embolization, the vast majority of aneurysms had saccular morphology (n=29); we also manufactured a single fusiform internal carotid artery aneurysm.
Supplemental material
Experimental setup of SITS and HANNES and neurointerventional training courses
All aneurysm models were successfully manufactured. Two different cervical vessel anatomies were used during training.
Before hands-on training with both the SITS and HANNES, trainees participated in a 4-hour theoretical session. This consisted of approximately 2.5 hours of structured presentations and discussions, including aneurysm and subarachnoid hemorrhage epidemiology, basic endovascular techniques, and peri-interventional medical management. This was followed by 1.5 hours of clinical case discussions based on fluoroscopy recordings from cases constituting the aneurysm portfolio.
Fourteen neurointerventional training sessions applying SITS (without implementation of HANNES) were conducted between October 2016 and November 2017. Subsequently, a total of 16 courses with HANNES took place between December 2017 and August 2018. All training courses were led by experienced neurointerventional physicians. One additional training course was offered to familiarize radiographers with stent-protected angioplasty of the cervical carotid artery. In all instances, the target aneurysm could be successfully treated using the chosen technique. Adjunctive devices used included remodeling balloons and remodeling stents, depending on the individual course itinerary.
Simulation of complications
Technical difficulties and minor complications, including transient inability to access the aneurysm, microcatheter displacement from the aneurysm during coil advancement, and coil protrusion from the aneurysm, were comparable to clinical practice and occurred relatively frequently during training courses. Clinical treatment difficulties for aneurysm model ‘B’ could be reproduced in various training sessions. Using distinct preshaped microcatheters, aneurysm selection appeared to be rather tough and almost impossible. Selecting the internal carotid artery with a straight microcatheter during training sessions and in the corresponding clinical case, aneurysm access emerged as finally feasible by slowly retracting the microcatheter inside the vessel. Furthermore, in aneurysm model ‘M’, several operators were unable to access the aneurysm using a straight microcatheter owing to a ledge effect at the ostium. In the corresponding clinical case, the identical problem had occurred. Interestingly, both in clinic and in the model, this difficulty could be overcome by steam shaping the microcatheter tip. We observed spontaneous rupture of a Tangoflex-based model during one of the training courses. Model rupture occurred near the aneurysm ostium and was deemed to be related to forceful advancement of a 0.027" microcatheter before stent placement. The rupture site gradually enlarged and the model had to be discarded owing to severe fluid leakage.
Comparison of microcatheter positioning
All microcatheter positions in the aneurysm models were assessed as ‘near’ identical or ‘comparable’ compared with clinical cases, and none of the microcatheter positions was rated as ‘not comparable’. Furthermore, no significant difference between the operator ratings was observed (1.50±0.55 and 1.67±0.52, p=0.599).
Figure 2 shows a comparison of three microcatheter positions in clinical cases and three probability clouds of microcatheter positions in our aneurysm models, respectively.

Comparison of microcatheter (mc) positions in three different aneurysm models with real positions in DSA during endovascular treatment (red crosses indicate the distal microcatheter tip position inside the aneurysm dome). ICA, internal carotid artery; Pcom, posterior communicating artery.
Evaluation of SITS and HANNES
Thirty-eight physicians with an average experience of 3.38±2.53 years participated in endovascular aneurysm training courses using the SITS between October 2016 and November 2017, whereas 23 physicians with an average experience of 4.60±4.02 years participated in such training courses using HANNES at our department between December 2017 and August 2018.
Twenty-one participants working on SITS (55%) compared with 15 participants working on HANNES (65%) occasionally (more than twice in the past 2 years) practiced neurointerventional procedures, whereas only two participants working on SITS (5%) compared with one participant working on HANNES (4%) regularly (more than twice in the past year) practiced neurointerventional procedures using a vascular model—that is, a silicone or rubber-based vascular replica in which the movement of introduced catheters and devices is controlled with a camera or with fluoroscopy (see online supplemental questionnaire).
Eighteen physicians working on SITS (47%) and 15 physicians (65%) training on HANNES had performed a diagnostic neuroangiography in patients as first operator over 200 times before participating in our hands-on training course (see online supplemental questionnaire).
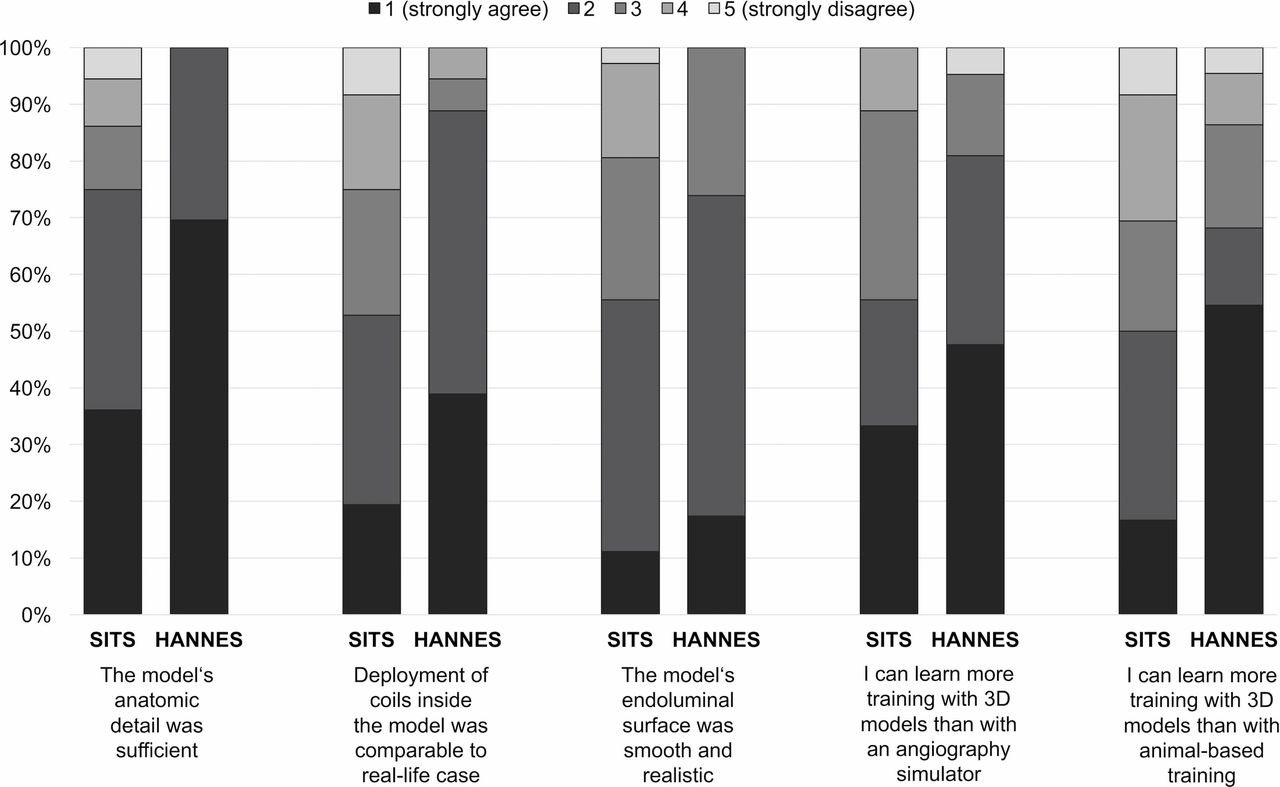
Pooling responses across all statements on SITS respectively on HANNES, we observed significantly more favorable rating for trainings with HANNES than those with SITS (with HANNES 0.85±1.04, with SITS 2.18±1.14, p<0.001).
Figure 3 illustrates selected answers to all statements assessed by the participants after training courses using SITS as described above and working on HANNES, respectively.

{kind=link}
{kind=link}
{kind=link}
Comparison of participant’s evaluation of SITS and HANNES. Left column indicates statements on training with SITS, right column indicates statements on training with HANNES, respectively.
In addition to this structured feedback, it was the course leaders’ impression that major strengths of HANNES from an educational perspective are the level of anatomic realism and detail as well as the ability to integrate identical clinical cases during the theoretical session as well as the hands-on training, allowing trainees to develop and test a treatment strategy in a unique way.
Discussion
With the rapid development of new endovascular treatment options for IAs, there is a growing need for physician training.20 Particularly for new neurointerventionalists, there is a high demand for learning and practicing technical skills required in the angiosuite.8 Neuroendovascular training courses can be beneficial for beginners and also for advanced neurointerventionalists.21 22 As 3D-printing techniques have been developing favorably in recent years,11 12 we aimed to assess the value of an integrated modular neurovascular training environment for aneurysm embolization using such aneurysm models.
Implementation of HANNES
Additive manufacturing in medicine originated in the 1980s and one of the first skull models was successfully printed by Mankovich et al using stereolithography in 1990.12 23 Diverse studies have been performed to assess the value and technical feasibility of synthetic vascular models in research and training.8 11 24 Wang et al demonstrated the feasibility of 3D aneurysm models for practicing aneurysm clipping before surgery,24 and Chueh et al showed the benefit of a silicone replica for preclinical evaluation of mechanical thrombectomy.25
On this background, HANNES was designed as a platform to allow hands-on training, testing of new devices, and research projects. Key design goals of HANNES were the complete replication of the femorocranial access route, near-physiologic flow conditions, a modular setup allowing easy switching of vessel segments, and the ability to integrate new, patient-specific models in the future following a standardized individualization process.18 The currently evaluated demonstrator of HANNES discloses the feasibility of this design as a training environment. Case-specific clinical difficulties, such as curved anatomies and difficult aneurysm access, can be reproduced easily by exchanging the intracranial aneurysm model and/or the cervical vessels. The training physicians can switch to a different treatment scenario or change from ‘treated’ back to ‘untreated’ condition as needed.
This aneurysm portfolio provides a wide selection of different aneurysm locations and configurations based on real patient data, allowing successful coil embolization in all instances. The degree of anatomic detail was overwhelmingly rated as sufficient. With this portfolio, the level of difficulty can be adapted to the participants’ demands. As confirmed in our survey, not only beginners, but also advanced neurointerventionalists benefit from our integrated neuroendovascular training environment as HANNES was rated as anatomically detailed and realistic. Compared with the former simple experimental setup (SITS), participants' feedback improved considerably after introduction of HANNES, particularly for the degree of anatomic realism and deployment characteristics of coils. Applying Formlabs models in HANNES compared with the use of TangoPlus models in SITS was assumed to be an important reason for this favorable evaluation. Training with giant aneurysm models required robust aneurysm walls (1.5–2 mm) and therefore, these aneurysm morphologies were preferably manufactured using the Formlabs material. Furthermore, microcatheter positioning in HANNES compared with clinical microcatheter positioning was at least comparable in all instances tested, which also supports the degree of anatomic realism of HANNES.
Apart from isolated training sessions, many other potential applications of HANNES can be imagined. Based on the aneurysm portfolio, a structured educational training programme could be designed. Spiotta et al emphasized structured training curricula previously, focusing on angiography simulators which might be incorporated into the angiosuite, creating a more realistic but simultaneously radiation-free environment.20 22 The precise elaboration of a structured curriculum is indispensable to improve the education of residents and fellows.20 22 According to the work of Crossley et al, essential steps of the training procedure should be determined systematically before assessing learning progress.26 They characterized the essential steps in mechanical thrombectomy, incorporated these metrics into a virtual reality endovascular simulation, and validated them in a defined setting with distinct neurointerventionalists, aiming to use these metrics in future training programmes.26 Major learning parameters in trainings with HANNES may be evaluated by repeating procedures under constant conditions. Periprocedural characteristics, such as time, contrast and fluoroscopy dose, occurrence of complications, or dangerous maneuvers, could be recorded.
Another potential application of HANNES is the preclinical testing of new devices. Previous studies have shown the benefit of using selected anatomies for evaluating device behavior and hands-on demonstration in artificial training settings.27 A study performed by Arthur et al in 2018, incorporated in the WEB Intrasaccular Therapy Study28 demonstrated the significance of creating a physical environment comprising a vascular simulator with patient-specific anatomies for education and training when introducing new technologies in clinical practice.27 HANNES may be particularly well qualified for such endeavors given its modular design, which allows easy testing of devices across a range of relevant anatomies.
Limitations and comparison of HANNES with other training environments
HANNES discloses some limitations in its developmental state. The absence of intracranial perforator branches may need to be overcome and the use of water as a blood simulating fluid might be considered a limitation, as its reduction on the surface friction inside the vessel models might be insufficient. Additionally, adaptation of the diastolic blood pressure in HANNES (100 mm Hg) to the physiologic pressure of 80 mm Hg and further improvements of real-life pressure properties are in progress. Furthermore, the application of HANNES is presently limited to coil embolization, flow diverter, and WEB placement. As aneurysm rupture is a highly dangerous complication of coil embolization,29 an integrated aneurysm rupture simulation is desirable and under development.
Comparison of HANNES with other training environments shows several key advantages based on our experience with training courses. All animal-based training is limited because the animal model’s anatomy is often not adequately representative of the human cerebrovascular system and therefore of limited suitability for learning and practicing neuroendovascular procedures.8 Based on our center’s previous experience with the rabbit elastase model as a training environment (more than 20 courses held before introduction of SITS and HANNES), we are convinced that many procedural aspects and difficulties associated with aneurysm embolization are intimately connected to the human neurovascular anatomy, which can be much more closely mimicked with HANNES than in the rabbit model. One limitation was that we did not collect structured participant feedback from animal training courses and therefore cannot directly compare participants’ impressions of these two environments. Furthermore, vasospasm and thrombus formation are not presently realized in HANNES but may occur in animal models, offering an opportunity to train for their management. However, appearance, frequency, severity, and treatment response of these complications in animal models may differ from those in humans, limiting potential learning. Overall, we feel that the need for animal-based training can be reduced by the implementation of HANNES. Aneurysm embolization courses at our center have now been completely moved from the rabbit elastase model to HANNES.
Apart from synthetic vascular models, the use of angiography simulators for medical training has been shown to be valuable in improving angiography skills, anatomical knowledge, and an understanding of microcatheter–microwire interaction.22 30 One of the big advantages of an angiography simulator is the radiation-free training environment operating with simulated fluoroscopy.30 The current stage of development of HANNES needs to be used under fluoroscopic control. We are aiming to develop transparent cervical and intracranial vessel modules that would allow training under optic camera control, greatly facilitating the setup of training courses without X-ray.
Compared with synthetic vascular models, in which the actual real treatment instruments are used, current angiography simulators incorporate pieces of standard catheters that are cut at the distal end, limiting the degree of realism of any haptic feedback obtained. Furthermore, on a simulator the ability to include patient-specific data may be limited. Working with proper microcatheters and microwires is an advantage of model-based training, in which participants can experience the behavior and technical characteristics of real treatment instruments. The application of very new devices can be tested and taught easily in the HANNES environment but would require substantial programing and preparation work in an angiographic simulator.
Conclusion
As a representative demonstrator for an integrated neurovascular training environment, HANNES provides realistic working conditions for various scenarios of intracranial aneurysm treatment and is therefore assessed as better than simpler training environments. Allowing implementation of case-specific hands-on training, HANNES aims to improve operator skills and may thus reduce the need for animal experiments for this purpose. Beyond training, the system may have value for assessment of standardized devices.
Acknowledgments
The authors thank Philips Healthcare for the support and realization of the “Hermann Zeumer Research Laboratory”, including a Philips AlluraClarity angiography system.
References
Footnotes
Contributors Conception/design of work: AF. Data collection: AMF, JK. Data analysis and interpretation: JHB, AF, JF, JS, JK, DK. Drafting the article: AF. Critical revision of the article: JS, JK, DK, JHB, AF, JF. Final approval of the version to be published: AF, JF. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: JS, JK, DK, JHB, AF, JF.
Funding This work was supported by the German Ministry for Education and Research (BMBF grant 031L0068B).
Competing interests The prepared patent is currently being reviewed by the corresponding authority; no other relationships or activities that could appear to have influenced the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.