Article Text

Abstract
Background and purpose Microcatheterization is an important, but also difficult, technique used for the embolization of intracranial aneurysms. The purpose of this study was to investigate the application of three-dimensional (3D) printing technology in microcatheter shaping.
Methods Nine cases of internal carotid artery posterior communicating artery aneurysm diagnosed by CT angiography were selected, and 3D printing technology was used to build a 3D model including the aneurysm and the parent artery. The hollow and translucent model had certain flexibility; it was immersed in water and the microcatheter was introduced into the water to the target position in the aneurysm, followed by heating the water temperature to 50°C. After soaking for 5 min, the microcatheter was taken out and the shaping was completed. After sterilization, the shaped microcatheter was used for arterial aneurysm embolization and evaluation was conducted.
Results Nine cases of microcatheter shaping were satisfactory and shaping the needle was not necessary; no rebound was observed. The microcatheter was placed in an ideal position, and the stent-assisted method was used in three cases of wide-neck aneurysm. There were no complications related to surgery.
Conclusion A new microcatheter shaping method using 3D printing technology makes intracranial artery aneurysm embolization more stable and efficient.
- aneurysm
- brain
- catheter
- coil
Statistics from Altmetric.com
Introduction
The stable and precise shaping of the microcatheter is the key to successful intervention embolization of the intracranial artery aneurysm.1–4 Appropriate microcatheter shaping provides intra-aneurysm stability of the microcatheter during aneurysm embolization. If the shape of the microcatheter tip is inappropriate it can cause premature retreat of the microcatheter and affects the further packing of the coil. Lee et al found that microcatheter shaping during aneurysm intervention resulted in good immediate and long-term angiographic outcomes with a low rate of periprocedural complications.5 Xiaochuan et al used the ‘Z-shape’, ‘S-shape’ or ‘U-shape’ of microcatheter tip shaping to locate and stabilize the microcatheter according to the position and orientation of the aneurysm. All patients presented good clinical results.6 Although microcatheter shaping is a routine technique, it can be difficult to conduct. In some special sites or in aneurysms with complex morphology, even experienced doctors sometimes need to shape the microcatheter multiple times to achieve successful shaping. There are many reports on the new methods of microcatheter shaping,2 7–9 but there are certain limitations. We developed a new microcatheter shaping method by using three-dimensional (3D) printing technology and evaluated the usefulness of the technique during surgery.
Methods
Patient selection
Because the diameter of the artery which functions as the parent internal carotid artery is relatively wide, the error caused by the difference in accuracy of the CT angiography (CTA) file can be reduced. At the same time, in order to reduce the impact of serious illness on prognostic evaluation, patients with relatively mild illness were selected. This study established the following inclusion criteria: (1) arterial aneurysm with rupture and hemorrhage confirmed by CT examination, Hunt-Hess grade 0–III; (2) post-communicating artery aneurysm confirmed by CTA examination; (3) no surgical-related contraindications. Nine patients with rupture communicating artery aneurysm diagnosed by CTA from March to September 2018 were selected.
Preoperative model preparation
Model establishment
The files in DICOM format of CTA were input into the Mimics Innovation Suite software (Materialise 18, Leuven, Belgium), to establish the STL (stereolithography) file. The 3D image data including the aneurysm and the parent artery were captured segmentally and input into a 3D printer (DWS-XFAB, Italy). Transparent elastic liquid photosensitive resin was used as the printing material, and DLP (digital light procession) 3D printing technology was used to print out the model, which is hollow and made of photosensitive resin; the printer model resolution was 0.02 mm. The inner cavity was printed at the ratio of 1:1 of the true vascular cavity with a wall thickness of 0.5 mm and certain visibility and flexibility. The lumen could be clearly observed and the wall could be pushed and pressed. After the preparation of the model, it was measured to check whether the inner diameter of the model matched the inner diameter of the STL image, and whether the appearance was consistent.
Model sterilized
The 3D model in this experiment was sterilized by low-temperature plasma sterilization and a low-temperature plasma sterilizer with a short sterilization time in the mode of enhanced circulation (specification PS-100-B, SHINVA, China), which is suitable for the sterilization of long-cavity items. The sterilization lasted about 1 hour. The sterilized model was reserved for use.
Intraoperative model use and evaluation
Microcatheter shaping
Because the silicone lumen was less compliant than a real blood vessel, the microcatheter produced great friction and was not easy to position in the model. We immersed the model in water and the whole process was operated under water to increase the compliance of the microcatheter. Generally, the microcatheter was directly placed into the model. In case of resistance, the wall of the tube could be pressed or the microguide wire could be introduced until a desired position of the aneurysm was reached. The water temperature was heated to 50°C. After 5 min, the microcatheters were pulled out to complete the shaping. The 0° SL-10 microcatheters were used for all microtubes (Stryker, USA) Figure 1.
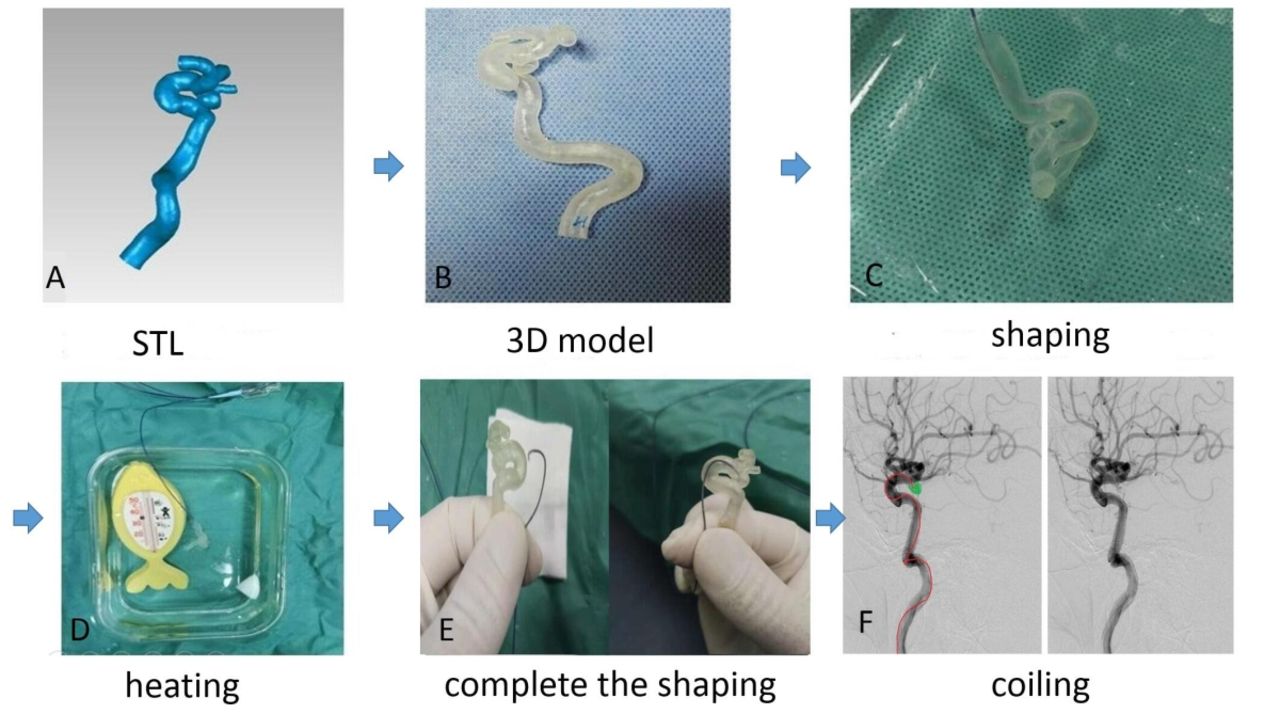
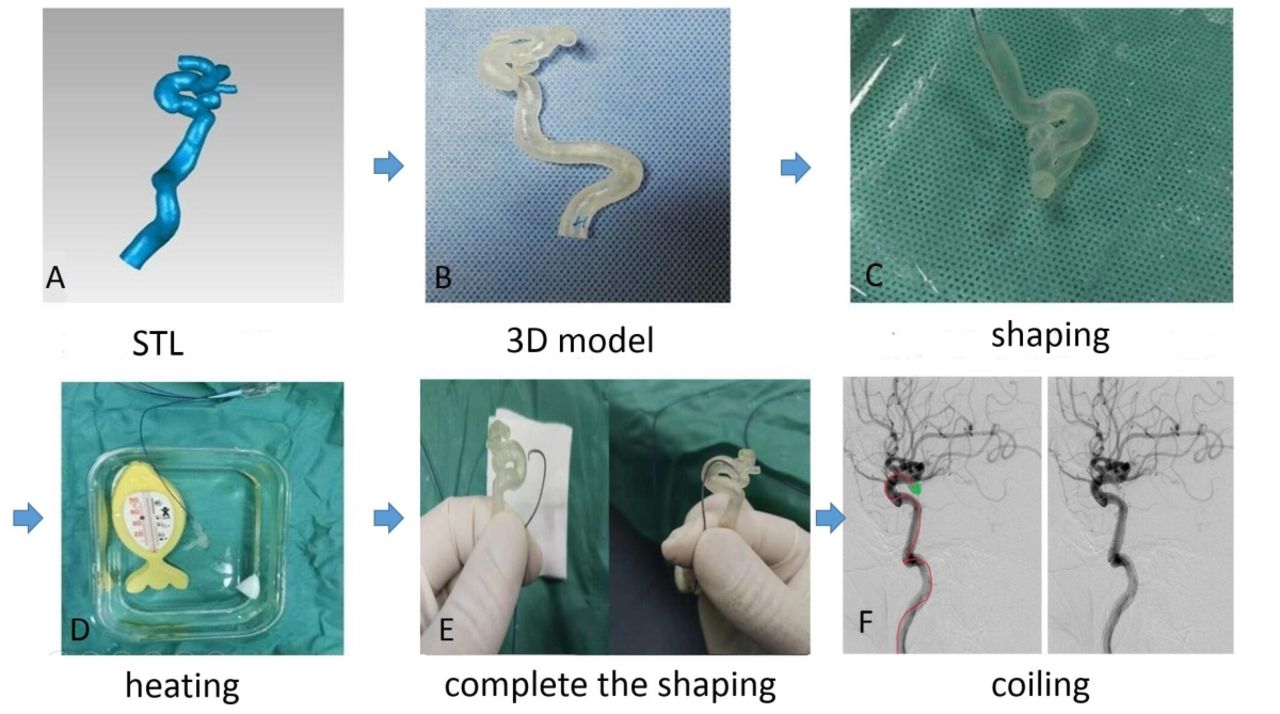{kind=link}
Intracranial aneurysm embolization using 3D printing technology for microcatheter shapping. Firstly, the STL format file was made by CTA source file(A), and the model of aneurysm was printed by 3D printer(B). The microcatheter was placed in the target position of the model in water(C). The water temperature was raised to 50°C. After 5 minutes(D), the microtubule was pulled out(E) and embolized with the new-shaped microtubule(F).
Practical application and evaluation
Routine 3D digital subtraction angiography (DSA) was performed before the operation and the size of the aneurysm was recorded. The shaped model was used for the treatment of the artery aneurysm embolization. The shaped microcatheters were evaluated using the methods of Toshihiro Ishibashi et al, and the usefulness of the technique was evaluated according to four standards (positioning, stability, and shape modification). The same standards were used for everyone. Two senior professors in neurointervention used ’good' and ’poor' to evaluate the accessibility, the in-position condition and stability, recorded whether re-shaping was needed,10 whether stent-assistance or other techniques were necessary, and evaluated other indicators such as aneurysm embolization rate and intraoperative complications. Prognostic assessment MRSModified Rankin Scale) was performed 3 months after surgery.
Results
In nine patients, the head end of the microcatheter was not well attached in the intra-aneurysm, but the packing of the coil was not affected. All the remaining shaped microcatheters reached the target position smoothly and were stable in the packing process. The microcatheters were not shaped for a second time in this study (supplementary table 1). Three patients with wide-neck aneurysms received stent-assisted treatment. For these three cases, the stents were first released, then the microcatheters were inserted into the aneurysm through the stent mesh by a guide wire. If the in-stent release technique was used, re-shaping might be needed. The packing process was stable with smooth arrival of the microcatheters in position and no surgical complications. Most achieved complete embolization. The prognosis was good at 3 months postoperatively (supplementary table 2).
Supplementary file 1
Supplementary file 2
Discussion
The application of 3D printing technology in medical care has developed rapidly in recent years. Kaneko et al have even successfully established a geometrically realistic intracranial aneurysm model with a living endothelium lining using 3D printing technology. This in vitro model will provide a new method for studying aneurysm growth or rupture.11 A recent multicenter study showed that past simulation training of neurological interventions was often performed using animal models, and lacked standardized training for neurointerventional physicians. Therefore, it is necessary to further develop a standardized artificial environment that meets the requirement to replace animal model training.12 3D printing technology provides a promising method to establish an in vitro model for simulation training of interventional surgery or to directly apply 3D printing techniques to surgery. Thus an in vitro model of an aneurysm can be established by 3D printing, and the microcatheter can be directly shaped by the model and applied to aneurysm embolization surgery.
Microcatheter shaping is one of the important factors for the successful embolization of an aneurysm. At present, most surgeons perform manual microcatheter shaping according to the 3D-DSA image on the screen. Although this technique is the basis for cerebrovascular intervention, sometimes the microcatheter shaping can be unsatisfactory. There are two main reasons. First, the 2D computer screen lacks in-depth information, so the surgeon cannot make accurate spatial assessments of the 3D structure and position. Second, it is difficult for the surgeon to accurately determine the true path of the microcatheter into the parent artery and has to depend on experience.10
It has also been reported that new methods have been proposed for microcatheter shaping; for example, some investigators used 3D printing technology to print a solid model and imitated the shape of the model to shape the microcatheter so that the surgeon can more intuitively understand its 3D shape. However, it still fails to get rid of the inaccuracy caused by the manual measurement, and the problem of rebound due to the use of the shaping needle cannot be overcome.9 10 Others have directly shaped the microcatheter in the body and introduced the microcatheter in between the parent artery and the aneurysm opening for stasis for a period of time. After it was pulled out, the head end was shaped for a second time.13 14 Shaping in vivo has certain risks compared with shaping in vitro and there are some uncontrollable factors in the degree of position-reaching of the microcatheter and the secondary shape of the head end.
Due to the expiration of the 3D printing patent, the cost has dropped drastically, and printing a single selected blood vessel model is relatively inexpensive. The use of new machines and materials has made 3D printing more applicable to medical clinics. In this group of patients, 3D printing technology was used to shape the microcatheter and the characteristics are as follows. In the past, most of the 3D printing of brain blood vessels used 3D-DSA. If a ruptured aneurysm requires emergency surgery, the printing time of the model is very quick and it is difficult to perform same day surgery. 3D-CTA is used in the source file. Although the accuracy of 3D-DSA is higher, there is little difference for large blood vessels such as the parent artery. Also, the CTA file is easy and fast to obtain, which can save a lot of time for model printing.15–20 After mastering the software synthesis technology, if intervention is planned, the STL format file required for 3D printing can be immediately synthesized by the software, which is then input to the printer to print out the 3D model of the aneurysm. Theoretically, it takes 30 min to synthesize, 2 hours and 30 min to print the model, and 1 hour for sterilization. If 1 hour is allowed for in the middle link, it takes at least 5 hours to create the sterilized model needed for the surgery. It takes more time when the factors in each link of the actual operation are taken into account. This surgery is basically carried out the next day. It is believed that if the process is further optimized, the surgery can be performed on the day of emergency. In the traditional shaping method, it is necessary to measure the distance from the aneurysm outlet to the target point in the tumor. Sometimes the second bending needs to be shaped in order to make the microcatheter more stable—that is, the distance from the proximal end of the parent artery to the aneurysm outlet and the angle between the head-end shaping, which is highly technically demanding for the surgeon, and even experienced surgeons sometimes need to shape multiple times. In this group of patients, the model is directly used for microcatheter shaping without the need to consider the length, angle, depth and other indicators of the microcatheter shaping. After predetermining the position of the head end of the microcatheter in the aneurysm cavity in advance, the microcatheter can be sent to the predetermined position in vitro without measurement, which can remove the limitation of manual shaping and is more precise. Also, rebound of the microcatheter after shaping can be avoided without the use of the shaping needle.
In the actual embolization treatment, the shaped microcatheters in this group can be placed quickly and smoothly in position and the microcatheters are stable during embolization, especially for the narrow neck aneurysms. For wide-neck aneurysms, this study used a stent-assisted technique and the embolization results are satisfactory. In future experiments, in order to make the microcatheters better able to reach the position, this study envisages that the STL files can be modified appropriately when designed by computer. By means of manual intervention, microcatheter shaping can be more smooth and closer to the ideal goal after the establishment of the model.
However, there are also limitations in this study. First, the number of samples is small and dominated by the communicating arteries, and most of them are small aneurysms. In order to facilitate the prognostic assessment, patients with a preoperative Hunt-Hess grade 0–III were selected, thus in-depth evaluation of large data is lacking. Second, in this group of models, liquid silicone rubber with soft texture was selected as the material and DLP printing technology was adopted. Because the model should be hollow, in order to avoid tube wall collapse during the printing, the model was designed in the lumen and some small internal supports were added in some positions, which may have had a minor effect on the microcatheter shaping. Third, the clinical results were evaluated manually and thus lack standardization.
Conclusion
In the treatment of intracranial aneurysm embolization, microcatheter shaping using 3D printed models is a new method which can make the microcatheter shaping standardized and programmed, and thus will be more convenient, stable and precise. It is expected to be promoted in the clinic setting.
References
Footnotes
YX and WT contributed equally.
WL and BD contributed equally.
Contributors YX, WT, ZW, YL, XG, BD and WL : designed and performed the experiments, analyzed and processed the data, drafted the manuscript. WT, ZW and YL: contributed to document collection, software processing, preparation of the 3D aneurysm model, disinfection and other preoperative preparations. BD and WL: participated in the surgery, revised the manuscript. YX and XG: participated in the surgery and the intraoperative evaluation.
Funding This work was supported by Dalian Municipal Science and Technology Plan [Grant number: 2015E12SF165], and supported by 81672968 National Natural Science Foundation of China.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement For access to the raw images obtained in this study, please contact the corresponding author.
Correction notice This article has been corrected since it appeared Online First. Funding has been added to the paper as follows "supported by 81672968 National Natural Science Foundation of China".
Patient consent for publication Not required.