Article Text

Abstract
Background and purpose Robotic-assisted endovascular interventions have been increasingly performed in the coronary and peripheral vascular beds. We aim to describe the feasibility and initial safety of a robotic-assisted platform for treating carotid artery disease.
Methods Single-center technical report of the first four consecutive cases of carotid artery stenting for the treatment of severe symptomatic carotid stenosis utilizing the CorPath GRX Robotic System (Corindus Inc, Waltham, MA).
Results Four patients (one in early 60s and three in early 70s; NASCET degree of stenosis: 88%, 77%, 83% and 82%) with ipsilateral strokes on presentation were treated. All steps of the procedure (including delivery/removal of micro-guidewire, emboli-protection system and angioplasty balloon) could be successfully performed robotically with the exception of navigation/deployment of the stents due to incompatibility with the current robotic platform. Technical success was achieved in all patients resulting in resolution of the stenosis without any complications.
Conclusions Robotic-assisted carotid artery stenting is technically feasible. Future studies are warranted to properly establish safety and benefits.
- stenosis
- stent
- stroke
- technique
Statistics from Altmetric.com
Introduction
Robotics has been increasingly incorporated across many areas of medicine. The robotic architecture can be thoroughly tailored for specific procedures in order to provide greater consistency and mechanical precision while also minimizing occupational hazards and optimizing the operator’s ergonomics and comfort during the surgical act. Robotic assistance for endovascular procedures in the coronary and peripheral vascular arterial beds is a rapidly growing reality. However, there is a paucity of experience and data about its utilization on the cerebrovascular bed including the carotid artery. Herein, we describe the first case series of robotically assisted carotid angioplasty and stenting for the treatment of severe symptomatic carotid stenosis.
Robotic system
The CorPath GRX Robotic System (Corindus Inc, Waltham, MA) consists of a table-side robotic unit connected to an operator cockpit by a communication cable (figure 1). The interventional cockpit is a radiation-shielded mobile workstation comprising a console with an X-ray foot pedal, three joysticks and touchscreen controls that allow the surgeon to remotely operate 1) a guide catheter 2) a 0.014 inch guidewire and 3) a rapid-exchange system including angioplasty balloons, stents and distal embolic protection devices, all with increments as small as 1 mm. In addition, the system enables the operator to rotate the guidewire in minimal increments, allowing for precise vascular navigation. An autonomous navigation “Rotate on Retract (RoR)” feature that enables quick navigation to a targeted lesion by automatically rotating the guidewire on joystick retraction in a more consistent and predictable manner is also integrated within the system. The rapid-exchange system joystick provides control of linear (advancement and retrieval) motion while the guide catheter and the guidewire joysticks allow for both linear and rotational (clockwise and counterclockwise) movements. The devices can be controlled independently (by using one joystick at a time) or simultaneously (by activating multiple joysticks at once). For precise, discrete manipulation, the rapid-exchange device, guidewire and catheter can also be manipulated in discreet 1 mm increments via the touch-screen buttons on the console. The procedure is followed in real-time from an ergonomically favorable seating position using an ultra-high-definition display monitor with audible feedback. The system also allows the operator to accurately measure lesion lengths using the guidewire or rapid exchange system movements as a reference. The table-side unit consists of (1) a single-use cassette that provides a platform for loading and unloading the interventional equipment and serves as a sterile barrier between the long-lasting robotic gear and the disposable interventional devices, (2) a table-side touchscreen that provides a user interface for the bedside operator via step-by-step instructions during system set-up, loading, and device exchanges, (3) an articulating arm mounted on the rail of the procedure table that allows for the support and flexible positioning of the robotic drive, and (4) the robotic drive encompassing seven motors that cover the linear, rotational and pinch functions. The system was cleared by the Food and Drug Administration for percutaneous coronary intervention in 2012 (K120834) and peripheral vascular intervention including carotid intervention in 2018 (K173288), but has not yet received clearance for intracranial neurovascular intervention in the USA.
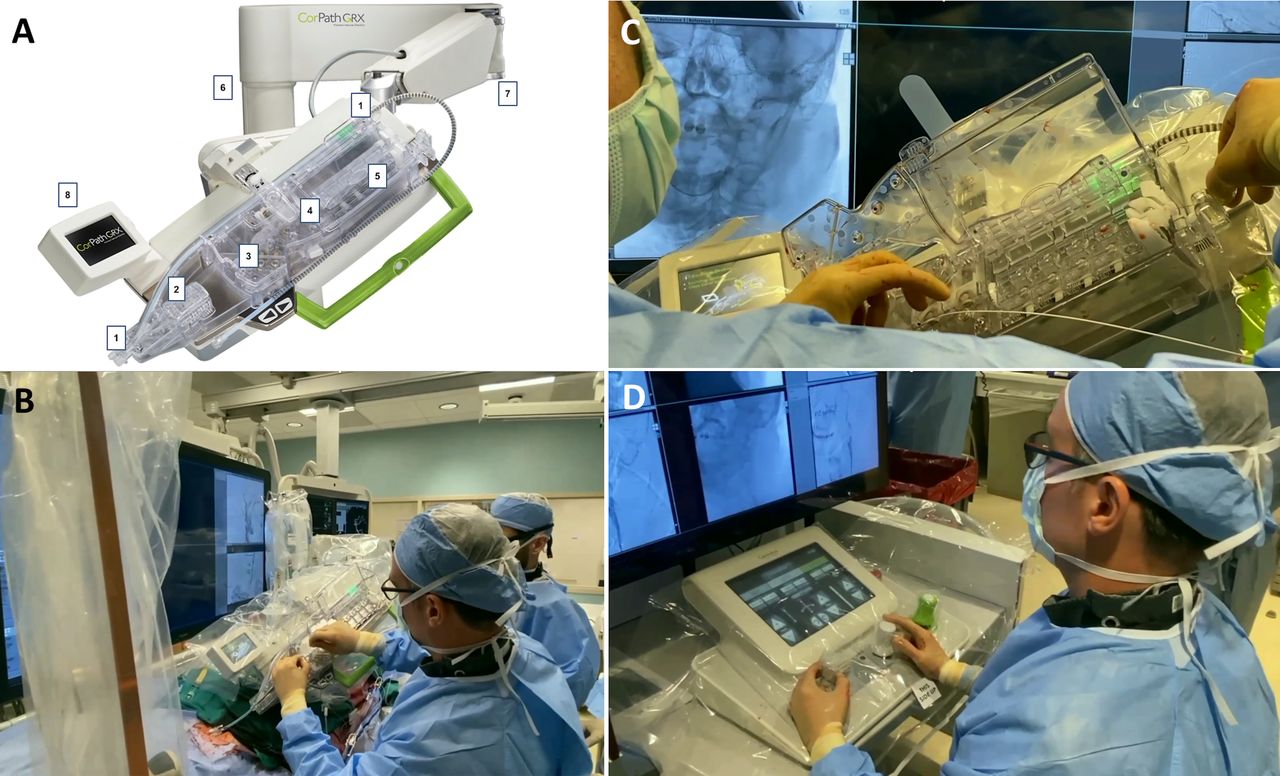
(A) Robotic drive unit:1–5, single-use cassette: 1, guide catheter support track; 2, guide catheter rotation module; 3, rapid exchange catheter module; 4, guidewire linear module; 5, guidewire rotation module; 6, procedure table mount; 7, robotic articulating arm; 8, table-side touchscreen. Copyright Corindus Inc, used with permission. (B) Robotic unit in relation to patient and operator. (C) Close-up view of the manual removal of the rapid exchange system after its robotic retraction. (D) Operator cockpit.
Study patients and procedures
Four consecutive patients underwent revascularization treatment for symptomatic carotid stenosis between November 19 and December 17, 2019.
Patient 1 was a septuagenarian individual with a history of hypertension, hyperlipidemia, diabetes mellitus, chronic kidney disease, and prior right middle cerebral artery (MCA) stroke who presented with transient right hemiparesis. Brain MRI showed small scattered acute-subacute embolic infarcts in the left MCA territory (figure 2A). Head and neck CT angiography (CTA) demonstrated severe stenosis of the proximal left internal carotid artery just above the carotid bulb due to calcified and soft plaque with minimal residual lumen.

Patient 1 (A–D; upper panels) and patient 2 (E–H; lower panels). Pre-revascularization diffusion-weighted MRI (A, E), pre-revascularization (B, F) and post-revascularization (C, G) digital subtraction angiography and native images (D, H).
Patient 2 was a sexagenarian individual with a history of asthma and smoking who presented with left hemianopsia, hemineglect, mild hemiparesis and dysarthria (National Institutes of Health Stroke Scale (NIHSS) 8). Head and neck CTA demonstrated severe stenosis of the proximal right internal carotid artery with complete occlusion of the MCA-M1 segment with thrombus extending and occluding a 6 mm distal M1 trunk aneurysm. The patient was treated with mechanical thrombectomy with successful reperfusion. A 24 hour follow-up MRI showed a moderate size infarct (figure 2E) with re-occlusion of the MCA which was confirmed on CTA. Ticagrelor and aspirin were started. Repeat CTA 12 days later showed spontaneous recanalization of the MCA. Stent-assisted coil embolization of the MCA trunk aneurysm was performed in anticipation of carotid artery stenting (CAS).
Patient 3 was a septuagenarian individual with a history of hypertension, hyperlipidemia, diabetes mellitus and prior left MCA stroke who presented with acute onset of right hemiparesis and dysarthria (NIHSS 6). Brain MRI revealed small acute left anterior cerebral artery-MCA watershed infarcts (figure 3A). A head and neck CTA showed severe stenosis of the proximal left internal carotid artery with a free-floating filling defect consistent with intraluminal thrombus. The patient was managed with intravenous heparinization for 6 days then converted to ticagrelor and aspirin in anticipation of CAS.
{kind=link}
{kind=link}
{kind=link}
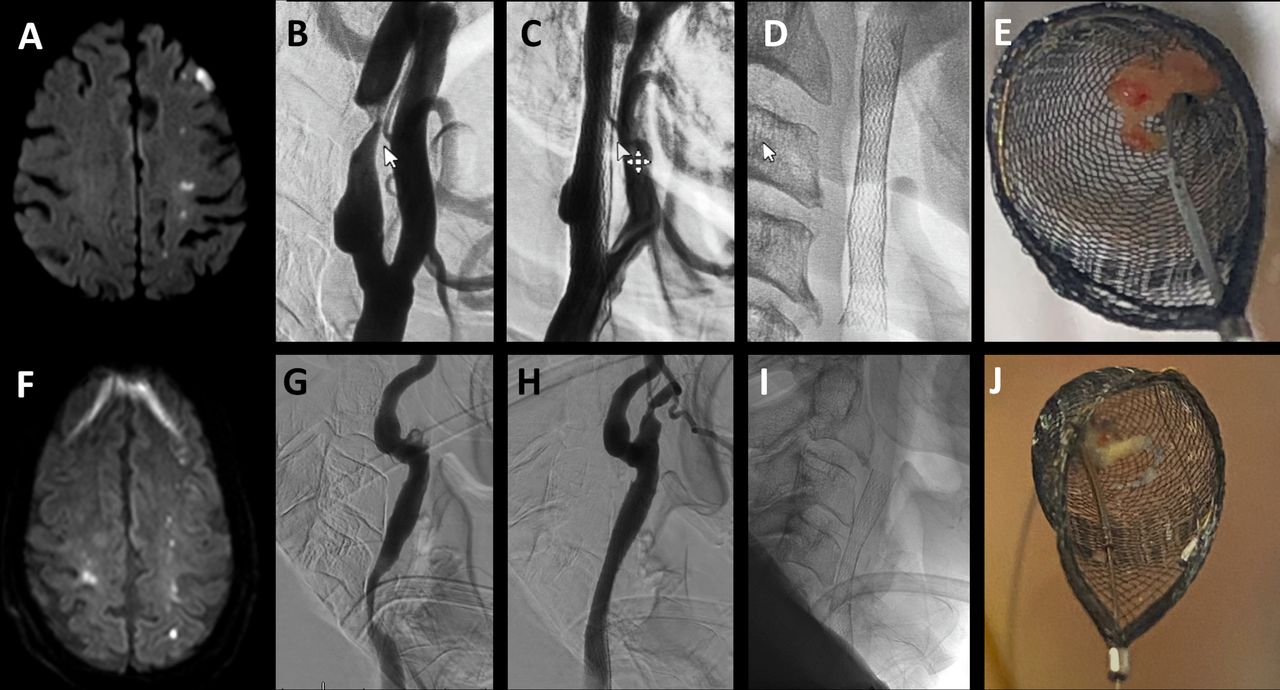
Patient 3 (A–E; upper panels) and patient 4 (F–J; lower panels). Pre-revascularization diffusion-weighted MRI (A, F), pre-revascularization (B, G) and post-revascularization (C, H) digital subtraction angiography, native images (D, I) and emboli protection devices demonstrating captured debris (E, J).
Patient 4 was a septuagenarian individual with a history of hypertension and hyperlipidemia who presented with right sided weakness (NIHSS 3). Head and neck CTA revealed chronic right carotid bulb occlusion and severely stenosed left mid-to-distal common carotid artery. Brain MRI revealed watershed infarcts involving both hemispheres, more significantly on the left (figure 3F). Ticagrelor and aspirin were started.
All treatment decisions were made in conjunction with the patients and their families after multidisciplinary input from the vascular neurology, neurosurgery and neuroendovascular teams. The authors applied for and were granted an exempted status from their institutional review board for this research. Patients underwent CAS 5, 13, 10 and 3 days after their presentation, respectively. On the day of the procedure, antiplatelet response was uniformly confirmed with the VerifyNow P2Y12 assay. All procedures were performed in a biplane angiography suite (Philips Allura) under monitored anesthesia care. On angiographic evaluation, the degree of stenosis according to the NASCET (North American Symptomatic Carotid Endarterectomy Trial) criteria was 88%, 77%, 83%, and 82%, respectively.
Technical description and procedural results
The robot operators underwent a formal protocolized training including the use a computer-based simulator at the manufacturer’s headquarters. Before the first human procedure, a simulated robotic-assisted CAS intervention was performed using the exact same devices in a model based on a 3D printer silicone reconstruction of the arterial system from the common femoral arteries to the cerebrovascular arterial tree. The operators trained in the model until they felt completely comfortable with the operating platform and had an understanding of the device response. The use of the system was felt to be very intuitive and the whole training took approximately 2 hours. An interventional cardiologist with greater than 30 robotic-assisted coronary interventions was present to proctor the cases. Right or left common femoral arterial access was obtained and a 6 French Shuttle sheath (Cook Medical Inc, Bloomington, IN) was inserted and connected to a continuous infusion system of heparinized saline solution (4000 units/L). Intraprocedural heparin bolus (70 units/kg) was administered to achieve an activated clotting time of 2–2.5-times the baseline. Selection catheterization of the distal common carotid artery was performed with the aid of a 125 cm Vitek catheter and a 0.038 inch guidewire. The Glidewire was removed and the sheath was connected to the table-side robotic drive using a Tuohy Borst system (Copilot Bleedback Control Valve; Abbott Vascular) to provide hemostasis and to enable the insertion of the micro-guidewire and rapid-exchange interventional devices into the guide catheter during the procedure.
At that point, the robotic-assisted portion of the procedure was initiated. A Synchro-2 0.014 inch guidewire (Stryker Neurovascular, Fremont, CA) was inserted in a 5 or 6 mm Spider-Fx (ev3, Plymouth, MN) distal embolic protection device rapid-exchange port and both devices were loaded into the appropriate modules and guide tracks of the robot cassette. The guidewire was then robotically advanced across the stenotic segment using a combination of linear and rotational maneuvers. Once the guidewire reached a stable position within the petrous internal carotid artery (ICA) the Spider-Fx catheter was robotically advanced into the distal cervical ICA. The guidewire was then robotically retracted and manually removed. The Spider-Fx guidewire was loaded into the wire track of the cassette and the filter was robotically advanced into the distal cervical ICA. At that point, the Spider-Fx catheter was robotically retracted deploying the filter.
The filter catheter was removed from the cassette. A 4.0 mm × 20 mm, 4.5 mm × 20 mm, or 6.0 mm × 30 mm Viatrac angioplasty balloon was advanced over the filter wire, loaded in the rapid-exchange track of the cassette and robotically navigated across the stenotic segment. Balloon inflation to nominal pressure was manually achieved followed by a control angiography. The balloon was then robotically retracted and manually removed. An XACT 8–10 mm × 40 mm stent was manually advanced over the filter wire, deployed across the stenotic segment, and removed. An angiogram confirmed optimal positioning of the stent with complete resolution of the stenosis in cases 1 and 2. Cases 3 and 4 showed residual stenosis and therefore received a second stent (XACT 8–10 mm × 40 mm and 10 mm × 30 mm, respectively) in order to provide better coverage across the soft plaque in anticipation to repeat angioplasty. Successful post-stent angioplasty with a Viatrac 6.0 mm × 30 mm balloon was robotically performed in cases 3 and 4. There was no residual stenosis in patients 1, 2 and 3 while there was 36% residual stenosis in patient 4 (figures 2 and 3).
The filter recovery catheter was then advanced over the filter wire, loaded in the rapid-exchange track of the cassette and robotically navigated across the stent to collapse and recover the filter. The filter wire and catheter were then simultaneously retracted by the robot system. Debris was observed within the filter in cases 3 and 4 (figure 3E,J). The shuttle sheath was then removed and hemostasis achieved after deployment of a 6 French AngioSeal closure device (Terumo Medical, Somerset, NJ). There were no periprocedural complications with stable to improved neurological status on discharge in all four patients.
Discussion
We report the first series of robotic-assisted carotid stenting. All steps of the procedure could be successfully performed with robotic assistance with the exception of the stent navigation and deployment due to its incompatibility with the current version of the robotic system. All cases were symptomatic, with evidence of embolic infarcts on pre-treatment imaging, and had a relatively high degree of complexity. Despite these clinical and anatomical challenges, technical success was achieved in all four cases resulting in resolution of the stenosis without any complications.
Robotics is not new to the percutaneous endovascular intervention space. In fact, the first pilot studies of robotically assisted percutaneous coronary intervention (R-PCI) date back to 2006.1 The system has since undergone multiple refinements and R-PCI has been shown to have comparable safety and clinical and procedural efficacy to the manual approach in prospective studies.2 3 The robotic approach has also been increasingly utilized for peripheral vascular interventions.4 Its expansion to neurovascular intervention was therefore the next obvious frontier.
The introduction of robotics in neuroendovascular medicine represents the inception of a new era with significant implications for individual patients, operators and systems of care. The robot’s sensitive mechanism and steady arms can deliver exceedingly accurate movements beyond even the most experienced and skilled of human hands without being affected by fatigue or suboptimal ergonomics. Furthermore, artificial intelligence algorithms can lead to a continuous technical evolution and provide better consistence across the different operators. Robotic assistance also brings significant benefits for the treating team as it can dramatically reduce the occupational hazards attributable to the cumulative radiation exposure as well as the musculoskeletal strain related to the prolonged wearing of radiation protective garments which may lead to permanent orthopedic injuries. One of the most significant innovations associated with endovascular robotics is the potential to perform interventional procedures remotely. Indeed, telerobotic-assisted PCI was recently successfully accomplished in five patients at a 20 mile distance from the operator.5 If this model can be successfully reproduced for mechanical thrombectomy in the future, it could potentially revolutionize acute stroke treatment by shortening the gaps in expertise and speed to reperfusion in more remote areas.
Despite the promising overall results, it is important to acknowledge that the current robotic platform has been designed for percutaneous cardiovascular and peripheral vascular interventions, and at this time lacks many of the attributes necessary for the more complex intracranial procedures including the ability to safely manage microcatheters and other over-the-wire coaxial systems. Neuroendovascular-specific engineering and software modifications have been recently incorporated into a prototype and tested in a live porcine model with simulated neuroendovascular pathology (rete mirabile and induced aneurysm) with excellent results.6 7 Despite these advances, loss of haptics still represents a very significant drawback to robotic procedures and it may be a critical limiting factor when dealing with the more delicate and tortuous intracranial anatomy.
Given the close similarities between carotid and coronary or peripheral interventions, which include a more favorable vascular anatomy (vs the more tortuous intracranial vasculature), and the availability of rapid-exchange device platforms (vs the over-the-wire intracranial platforms), CAS was the most logical neurovascular procedure to be initially performed with the currently available technology. This has important potential implications in terms of both procedural volumes and safety. Despite the conflicting clinical trial data, the relative performance of CAS in relation to carotid endarterectomy has increased over time and improvements in CAS outcomes have occurred despite increases in vascular risk factors and the proportion of symptomatic patients being treated.8 9 The recent design improvements in stent and embolic protection systems may further reduce treatment risks and increase CAS utilization even further.10 It is likely that robotics will add further advantages to these technological advances.
In conclusion, we have demonstrated that robotic-assisted CAS is technically feasible. Future studies are warranted to properly establish its safety, benefits to patients and operating team, and cost-effectiveness profile.
Footnotes
Contributors RGN: Study conception, design of the work, acquisition of data, interpretation of data, drafting of the manuscript. RS: Data acquisition, critical revision of manuscript. ARA: Data acquisition, critical revision of manuscript. MHM: Critical revision of manuscript. MRF: Critical revision of manuscript. DCH: Acquisition of data, interpretation of data, drafting of the manuscript. All authors gave final approval of the version to be published, and are in agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests RGN: Corindus Vascular Robotics (Physician Advisory Board, stock options). Unrelated to this research: RGN: Stryker Neurovascular (DAWN Trial Principal Investigator- no compensation, TREVO Registry Steering Committee – no compensation, Trevo-2 Trial Principal Investigator- modest; Consultant - significant); Medtronic (SWIFT Trial Steering Committee - modest; SWIFT-Prime Trial Steering Committee – no compensation; STAR Trial Angiographic Core Lab - significant); Penumbra (3D Separator Trial Executive Committee – no compensation); Cerenovus/ Neuravi (ENDOLOW Trial Principal Investigator, EXCELLENT Registry Principal Investigator, ARISE-2 trial Steering Committee – no compensation, Physician Advisory Board, modest); Phenox (PROST Trial Principal Investigator, Physician Advisory Board, modest); Anaconda (Physician Advisory Board, modest); Genentech (Physician Advisory Board – modest); Biogen (CHARM Trial Steering Committee; Physician Advisory Board – modest); Prolong Pharmaceuticals (Physician Advisory Board – modest); Allm Inc. (Physician Advisory Board – no compensation); IschemaView (Speaker, modest); Brainomix (Physician Advisory Board, stock options); Sensome (Research Device Use – no compensation); Viz-AI (Physician Advisory Board, stock options); Philips (Research Software Use – no compensation, Speaker - modest); Vesalio (Physician Advisory Board, stock options); Ceretrieve (Physician Advisory Board, stock options); Astrocyte (Physician Advisory Board, stock options). DCH: Consultant for Stryker and Vesalio, Viz-AI (stock options).
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.