Article Text

Abstract
Background Direct thromboaspiration has been reported as an effective mechanical treatment for acute ischemic stroke. We aimed to determine whether the angle of interaction between the aspiration catheter and the clot affects the success of clot removal in ischemic stroke patients with large vessel occlusion in the anterior and posterior circulation.
Methods All patients treated at our institution by direct thromboaspiration as a firstline technique between January 2016 and December 2017 were enrolled in the study. We retrospectively reviewed baseline and procedural characteristics, the angle of interaction formed between the aspiration catheter and the clot, the modified Thrombolysis in Cerebral Infarction score, and the 3 month modified Rankin Scale score.
Results 85 patients underwent direct thromboaspiration as the firstline treatment during the study period. 100 direct thromboaspiration passes were performed. An angle of interaction of ≥125.5° significantly influenced the success of clot removal (P<0.001) with good sensitivity and specificity, in particular for occlusion of the middle cerebral and basilar artery. The combination of aspiration with a stent retriever based thrombectomy was a valid rescue treatment in cases of standalone direct thromboaspiration failure.
Conclusions In our series, an angle of interaction between the aspiration catheter and the clot of ≥125.5° was significantly associated with successful clot removal. The prediction of the angle of interaction on pretreatment imaging may help operators to select the most adequate mechanical thrombectomy technique on a case by case basis.
- Stroke
- Thrombectomy
- Catheter
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Since 2015, stent retriever thrombectomy (SRT) associated with intravenous fibrinolysis is the treatment of reference for acute ischemic stroke (AIS) secondary to large vessel occlusion in the anterior circulation.1–5 Direct aspiration of the clot or direct thromboaspiration (DTA) performed with dedicated large bore catheters6 7 represents an alternative technique that is currently mainly performed by neurointerventionalists. When effective, DTA has advantages over SRT, such as reduction of the cost and duration of the procedure. Nevertheless, in cases of DTA failure, an SRT is performed as a rescue treatment,6 8 thus increasing the cost and duration of the overall procedure compared with a standalone SRT.
Irrespective of the thrombectomy technique, different factors are involved in the success of clot removal, including clot consistency, size, location, and the anatomy of the occluded artery.9–12 As previously reported by Zhu et al,13 a curved shape of the middle cerebral artery (MCA) was related to failure of clot removal when the Merci retriever device (Concentric Medical Inc, Mountain View, California, USA) was used for mechanical thrombectomy (MTB). Similarly, Schwaiger et al 14 showed that the efficacy of SRT in the anterior circulation was negatively influenced by the tortuosity of the MCA. Based on these findings, we hypothesized that vessel anatomy may also influence DTA efficacy by modifying the angle of interaction (AOI) between the aspiration catheter and the clot.
In this study, we retrospectively measured the AOI between the aspiration catheter and the clot in a consecutive series of patients treated at our institution by DTA for an AIS to assess whether it was related to the efficacy or failure of the technique. We also aimed to determine an AOI cut-off value to enable operators to predict the success of the DTA.
Methods
We performed a single center retrospective review of the clinical and radiological records of all consecutive patients treated for an AIS of the anterior or posterior circulation by MTB between January 2016 and December 2017. All patients treated by DTA as a firstline technique were included in the study. The AOI of each DTA pass and the final result of the procedure were assessed according to the Thrombolysis in Cerebral Infarction score (TICI).15 Ethics approval was obtained from the local institutional review board.
Patient selection by imaging
According to our institutional protocol, AIS patients were evaluated by a native CT scan, CT angiography, CT perfusion, and an automated CT perfusion system (RAPID software; iSchemaView, Menlo Park, California, USA). Patients presenting with an AIS in the anterior circulation with a cerebral blood flow reduction of ≤70 mL and a cerebral blood flow/mean transit time mismatch ratio of ≥1.8 were considered eligible for MTB within 8 hours after stroke onset.16Patients presenting with an AIS in the posterior circulation within 24 hours from symptom onset were considered eligible for MTB if a basilar artery occlusion was present.
Direct thromboaspiration procedures
All procedures were performed with the patient under general anesthesia using a biplane C arm Allura Clarity FD20 (Philips Healthcare, Best, The Netherlands). Eligible patients received intravenous recombinant tissue plasminogen activator prior to MTB. Three types of aspiration catheters were used during the study period: ACE 64 (Penumbra Inc, Alameda, California, USA), SOFIA 6F, and SOFIA 5F (MicroVention, Aliso Viejo, California, USA). The type used for each case was selected according to operator preference. Procedures were performed via a common femoral artery access. A guide catheter was placed proximally in the concerned internal carotid or vertebral artery and the aspiration catheter was advanced as close as possible to the proximal edge of the clot. The catheter was then connected to a vacuum system (Penumbra Inc) and negative pressure was applied. Negative pressure was interrupted when significant blood flow was visible inside the tube connecting the catheter to the vacuum system. If any blood flow was visible inside the tube, the clot was assumed to be stuck at the distal tip of the catheter. In this case, the catheter was gently withdrawn inside the guide catheter. Up to three DTA passes were performed for each patient. In cases of clot removal failure, a combined DTA/SRT technique was performed as a rescue treatment as follows: the aspiration catheter (previously used for DTA) was maintained proximal to the clot and a microcatheter was advanced over a microguidewire beyond the occlusion point. A stent retriever was then advanced and delivered via the microcatheter through the clot. Subsequently, the stent retriever was entirely retrieved out of the patient’s body through the aspiration catheter, while a concomitant negative pressure was applied by the vacuum system.
Measurement of the angle of interaction
Intraoperative DSA images were retrospectively reviewed by two operators (PM and GB) with experience in MTB in a consensus reading to identify the AOI formed between the major axes of the aspiration catheter and the clot (figure 1). AOIs were measured using OsiriX software (Pixmeo Sarl, Bernex, Switzerland) with a specific tool for angle measurement, reviewers analyzed working projections performed before and after vessel recanalization (figure 1). In cases of missed occluded artery reopening, the axis of the clot was evaluated by analyzing angiograms performed when the microguidewire and/or the microcatheter were placed beyond the occlusion point. In cases where multiple DTA passes were performed during the same procedure, the AOI was measured for each pass.
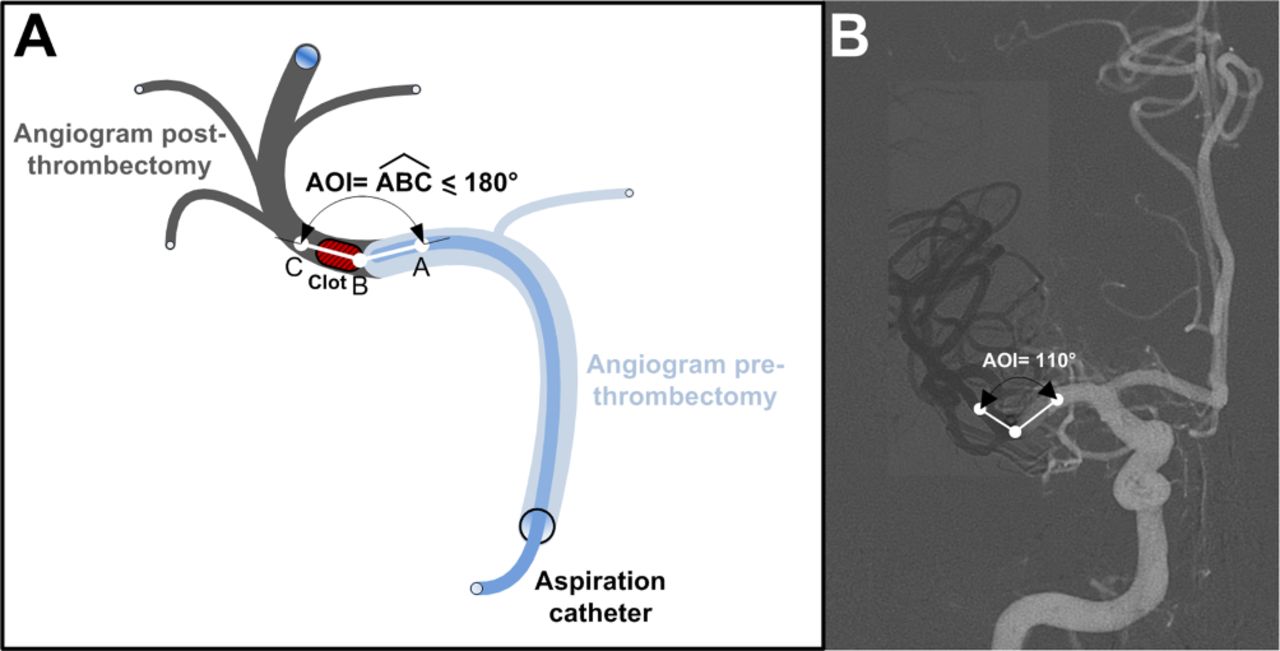
Schematics of vessel anatomy and example of angle of interaction (AOI). Light gray and dark gray depict the vessels before and after thromboaspiration, respectively. (A) The AOI is defined as the smallest angle (≤180°) between the clot (red) and the aspiration catheter (blue). (B) Example AOI on real DSA.
Statistical analysis
The influence of the AOI between the aspiration catheter and the clot on the probability of success of the DTA was evaluated by logistic regression. An analysis of the area under the receiver operating characteristic (AUC of the ROC) curve was used to test the accuracy of predicting the procedure success rate based on the AOI. The Kolmogorov–Smirnov test was used to test the normal distribution of continuous data in all groups before performing parametric tests (analysis of variance). In the case of a non-normal distribution of data in at least one of the groups to be tested and in non-continuous variables, a non-parametric test was used (Kruskal–Wallis test) to compare medians between groups. Associations between categorical variables were assessed by Fisher’s exact test. A two tailed significance level of 0.05 was used for all tests. All statistical analyses were performed on SPSS V.22.
Results
From January 2016 to December 2017, 225 patients presenting with an AIS in the anterior and posterior circulation due to large vessel occlusion were treated at our institution by MTB. Eighty-five patients received DTA as the firstline treatment (table 1) and 140 patients were directly treated with SRT.
Clinical and procedural variables subdivided in success or failure of direct thromboaspiration
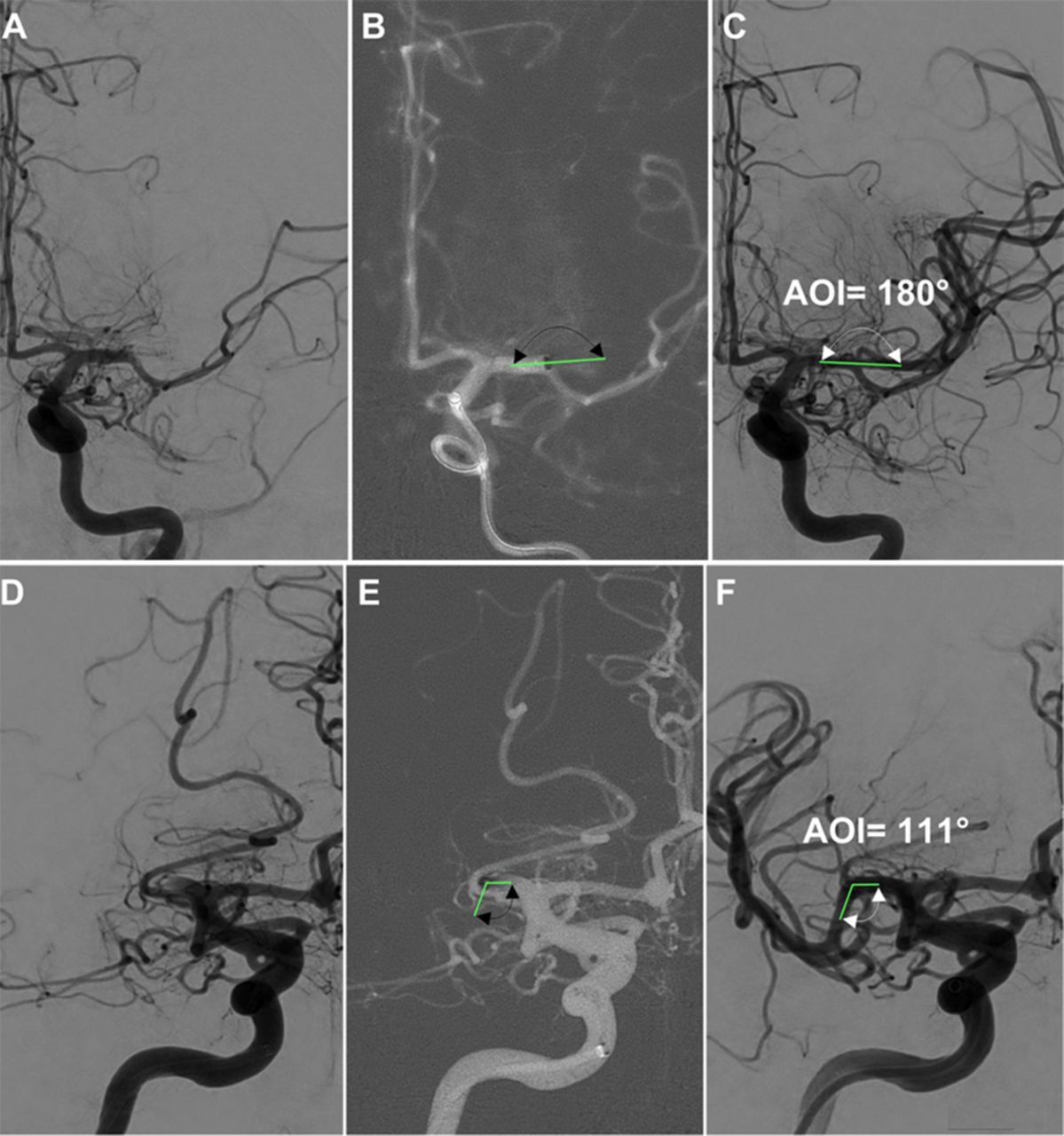
Most occlusions involved the MCA (63/85); other locations were the carotid artery terminus (n=13) and the basilar artery (n=9). In 65 of 85 patients (76.4%), DTA was successful in clot removal with a TICI score of ≥2b. In 57 of 65 patients, DTA was effective at first pass, while in 8 of 65 patients (7 cases of carotid artery terminus occlusions), a second or third pass was performed to obtain adequate recanalization (figure 2). All patients with basilar artery occlusion were successfully treated with a single DTA pass. In the remaining 20 of 85 cases (23.5%), a rescue combined DTA/STR technique was performed after DTA failure. Rescue DTA/STR was successful (TICI score ≥2b) in 15 cases (75%) cases. In 21 of 85 cases (24.7%), a distal embolus was noted after the first proximal thromboaspiration.
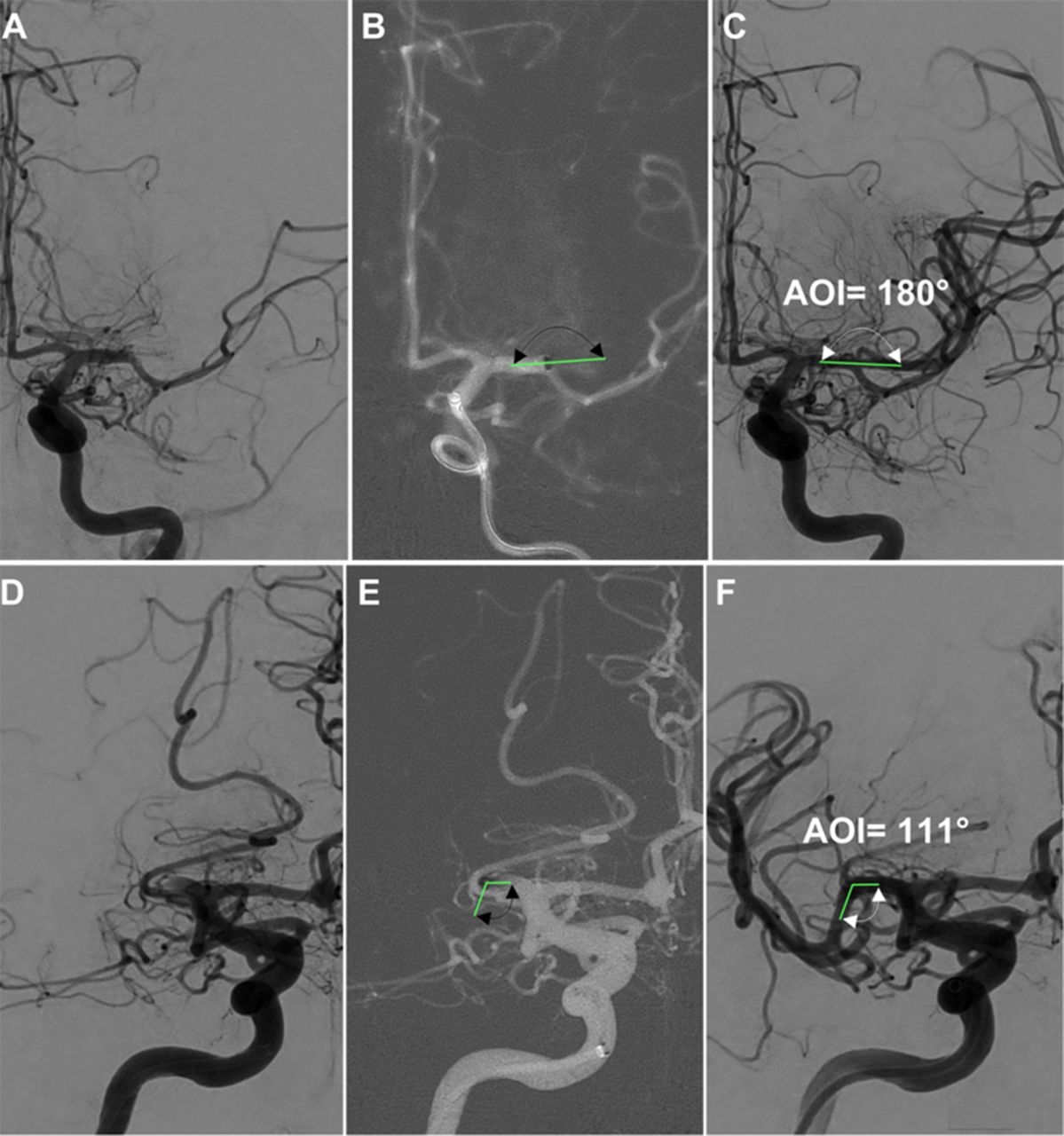
Two examples of favorable (A–C) and unfavorable (D–F) angles of interaction (green lines). Recanalization after one direct thromboaspiration pass: (A) occlusion; (B) catheter in contact with the clot; (C) recanalization (angle of interaction (AOI)=180°). Recanalization after rescue treatment with stent retriever thrombectomy: (D) occlusion; (E) catheter in contact with the clot; (F) recanalization (AOI=111°).
In such cases it was not possible to discern whether the distal embolus was already present prior to the proximal thromboaspiration.
In 1 of 21 cases (4.8%) the embolus was in a new territory (A3 segment of the anterior cerebral artery). In the other 20 cases (95.2%), the distal embolus was in the same territory of the target vessel (19 cases of MCA, 1 case of basilar artery).
In 13 of 20 cases (65%), the distal embolus was judged not accessible for retrieval for both DTA and SRT. In seven cases the distal clot was judged not reachable by the aspiration catheter but the clot was successfully removed combining DTA with SRT.
Forty-seven (55%) of 85 patients presented with a modified Rankin Scale score of ≤2 at the 90 day follow-up.
Statistical results
Overall, 100 DTA passes were performed in our series and each pass was retrospectively evaluated to assess the AOI between the clot and the aspiration catheter. Effective DTA passes were associated with a median value of 160° (IQR 139–167°). The median value recorded for unsuccessful DTA passes was 114° (IQR 105–134.5°). The AOI value significantly influenced the clot removal success rate (P<0.001). For a 1° increase in the angle, the odds of success increased by a factor of 1.087 or 8.7%. ROC analysis resulted in good sensitivity and specificity of AOI in predicting the procedure success rate, with an AUC of 0.882 (95% CI 0.803 to 0.961; P<0.001). According to the ROC analysis, a reasonable cut-off of AOI to predict procedure success was 125.5°, with a sensitivity of 95.5% and a specificity of 66.7% (figure 3A-B). However, a slightly smaller angle of 122.0° resulted in a sensitivity of 100% with only a slightly lower specificity (63.6%).
The site of occlusion significantly affected the AOI and thus the success rates of the procedure (P=0.006). As a consequence, clot locations associated with an unfavorable AOI were related to a higher number of DTA attempts and DTA/STR technique rescue procedures (P=0.045). No association was found between catheter type or diameter and success rate of first thromboaspiration attempt (P=0.473).

{kind=link}
{kind=link}
{kind=link}
(A) Boxplot of the angle of interaction (AOI) between the major axis of the aspiration catheter and the major axis of clots located in the middle cerebral artery in unsuccessful and successful mechanical thrombectomy. Larger AOIs are associated with higher success rates (P<0.001). (B) Receiver operating characteristic (ROC) curve of the AOI between the major axes of the aspiration catheter and the clot in the middle cerebral artery as a predictor of success rate of mechanical thrombectomy with direct thromboaspiration. AUC=0.915 (95% CI 0.830 to 0.999) (P<0.001).
Given the differences in the success rate observed in the three different anatomical locations (MCA, basilar artery, and carotid artery terminus), a separate logistic regression and ROC analysis were performed for each occlusion site. These showed that the influence of the AOI on procedure success rate was greatest when the clot was located in the MCA (figure 3A). In this location, a 1° increase in the AOI increased the odds of success by 1.098 or 9.8% (P<0.001), and the ROC analysis showed excellent sensitivity and specificity with an AUC of 0.915 (95% CI 0.830 to 0.999; P<0.001) (figure 3B). An angle of 125.5° also proved a reasonable cut-off for clots in the MCA, resulting in a sensitivity of 96.2% and a specificity of 80.0%. Of note, an angle of 122° resulted in a sensitivity of 100% and a specificity of 76.0%. The same analysis was not possible for clots in the basilar artery as all procedures were successful in this location. In the carotid artery terminus, the AOI did not significantly affect the procedure success rate, with an increase of 1.046 in the OR for a 1° increase in the angle (P=0.235). The AUC in the ROC analysis was also low (0.635 (95% CI 0.371 to 0.979); P=0.306).
Discussion
In this retrospective study of patients presenting with an AIS in the anterior and posterior circulation due to large vessel occlusion, we showed that vessel anatomy influences MTB performed by DTA which, in turn, is influenced by the AOI between the aspiration catheter and the clot. To be successful, the DTA technique requires an optimal AOI between the clot and the distal hole of the aspiration catheter to maximize the contact surface area. We found that an AOI ≥125.5° was significantly related to successful clot removal (P<0.001) irrespective of the type or inner diameter of the catheter used to perform DTA. The overall lowest number of DTA passes was associated with an AOI of approximately 180°. In these cases, the main axis of the catheter is coaxial to the main axis of the clot and the suction force is transmitted to the entire length of clot. The highest successful clot removal rate was recorded for the MCA M1 segment and basilar artery occlusions where an AOI of ≥125.5° was recorded in most cases. For M1 occlusions, an increase of 1° in the AOI increased the odds of success by 9.8% (P<0.001) and a TICI ≥2b at the first DTA pass was obtained in 68.2% of these patients.
Several clinical and experimental studies have evaluated factors related to the failure of MTB17–22 and vessel anatomy has been reported as one of the main factors related to clot removal failure. Zhu et al 13 evaluated the results of patients treated with the Merci retriever device for MCA occlusions. The shape, curvature, and branches of the MCA were identified on pretreatment MRI analyzing T2 weighted gradient echo susceptibility vessel sign (SVS) and the angle of the SVS curvature was evaluated with dedicated software. Two patient groups were identified: one presenting a straight SVS and one presenting branching and/or a curved SVS. Endovascular treatment was more effective in the straight SVS group, with a higher recanalization rate compared with the curved SVS group. Schweiger et al 14 evaluated how vessel anatomy influenced MTB performed with stent retrievers in the carotid artery terminus, and MCA (M1 and M2) occlusions. Vessel anatomy was assessed on intraoperative anterior–posterior by DSA measuring the angle formed by the occluded segment of the MCA and the more proximal patent arterial segment. The authors found that a curved vessel anatomy negatively influenced SRT efficacy.
The Contact Aspiration vs Stent Retriever for Successful Revascularization (ASTER) trial23 compared the results of 381 patients presenting with AIS due to a large vessel occlusion in the anterior circulation and treated by SRT or DTA. The study failed to demonstrate any significant difference in terms of effective recanalization (85.4% and 83.1% for DTA and SRT, respectively). Moreover, no significant differences in terms of clinical outcome or per procedural adverse events were recorded between the groups. In this study, patients were randomized to receive SRT or DTA irrespective of clot location or vascular anatomy. Based on our results, we have reasons to argue that DTA and SRT should not to be considered as competing procedures or alternatives but rather as different techniques to be performed alone or in combination in different scenarios and selected on a case by case basis.
Blanc et al 24 identified clot location as the main factor related to DTA efficacy with a high rate of successful recanalization for M1 occlusions and a low rate for carotid artery terminus occlusions. The authors suggested that there was a more effective interaction in the M1 location between the aspiration catheter and the clot due to the better correspondence between the vessel and the catheter diameters. In accordance with these findings, we observed that DTA was more effective for M1 occlusions, while carotid artery terminus occlusions were associated with a higher number of DTA passes and DTA/SRT rescue treatments, with an adequate clot removal (TICI ≥2b) obtained at first pass in only 38.4% of cases. This latter result was probably due to the significant clot burden related to such a location and the lack of correspondence between the diameter of the catheter and the vessel. In addition, clots at this location appeared to be more prone to fragmentation and embolization in more distal branches (ie, the M1 segment). Gory et al 25 compared SRT and DTA as firstline approaches for the treatment of AIS in the posterior circulation secondary to a basilar artery occlusion and observed that DTA had a higher recanalization rate and shorter procedure duration compared with SRT, similar to our study.
Our results demonstrated that the efficacy of the DTA was related to the AOI between the aspiration catheter and the clot. Prediction of such an AOI could help the operator in selecting the most appropriate MTB technique on a case by case basis. Ideally, DTA should be performed as a first approach for an AOI ≥125° and SRT or a combined DTA/SRT for an AOI ≤125°. Interestingly, we found that SRT was a valid rescue technique with a high rate of target vessel recanalization in cases of DTA failure (15 of 20 cases), even for an unfavorable AOI.
At present, diagnostic tools do not allow the prospective measurement of the AOI and only indirect findings help the operator to define such an angle. In some cases, we observed that the AOI could be predicted as being formed by the major axis of the clot visible as a hyperdense or hypointense sign26 27 on the preprocedural CT or MRI scan and the hypothetical position of the distal tip of the aspiration catheter speculated analyzing CT or MR angiography. In other instances, the AOI could be intraoperatively predicted by DSA analyzing the orientation of the proximal portion of the occluded vessel and, in the presence of collateral circulation, the distal edge of the clot outlined by retrograde contrast filling.28
In the majority of the cases in our series we were not able the predict the AOI on preprocedural imaging because the clot was not visible. Nevertheless, in a few cases (mostly basilar artery occlusions) we were able to identify such angles, which were confirmed by DSA after recanalization. We considered a statistical analysis to evaluate the concordance between the AOI value prospectively evaluated on the preprocedural imaging and the value evaluated by DSA after recanalization but we concluded that such an analysis was not appropriate given the limited number of cases in which AOI prediction was possible on preprocedural imaging.
Our study had some limitations. The study was retrospective and conducted in one center where a relatively small number of patients were evaluated. Furthermore, our study was not designed to demonstrate a possible correlation between the AOI value before and after recanalization. Nevertheless, the study adds additional information to the current knowledge of MTB and could serve as a basis for the development of diagnostic tools in the future, thus enabling the operators to evaluate the AOI using preprocedural imaging in order to select the most adequate MTB technique. Furthermore, prediction of the location of the clot could allow the selection of the most effective thrombectomy device and the optimal interaction between the clot and the device used for MTB, improving the rate of first pass recanalization irrespective of the thrombectomy technique used.29–31
Conclusion
This retrospective study showed that the efficacy of DTA was related to the AOI between the aspiration catheter and the clot. An AOI of ≥125.5° was associated with successful clot removal by DTA. In our series, DTA was highly effective for basilar artery occlusions where the straight anatomy of the artery allowed an overall AOI of ≥125.5° among cases. We also observed that a combined technique of DTA/SRT was a valid rescue treatment in standalone DTA failure, even in cases of unfavorable AOI. The prediction of AOI on pretreatment imaging might help operators in selecting the most adequate MTB technique on a case by case basis.
References
Footnotes
Contributors Substantial contributions to the conception or design of the work; acquisition, analysis, or interpretation of data for the work; drafting the work; revising it critically for important intellectual content; final approval of the version to be published; and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Ethics approval Ethics approval was obtained from the local institutional review board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All the data are available upon request to the corresponding author.
Patient consent for publication Not required.