Article Text

Abstract
Introduction Transradial access is increasingly used among neurointerventionalists as an alternative to the transfemoral route. Currently available data, building on the interventional cardiology experience, primarily focus on right radial access. However, there are clinical scenarios when left-sided access may be indicated. The purpose of this study was to evaluate the technical feasibility of left transradial access to cerebral angiography across three institutions.
Methods A retrospective chart review was performed for patients who underwent cerebral angiography accessed via the left radial artery at three institutions between January 2018 and July 2019. The outcome variables studied were successful catheterization, vascular complications, and fluoroscopic time.
Results Nineteen patients underwent a total of 25 cerebral angiograms via left transradial access for cerebral aneurysms (n=15), basilar occlusion (n=1), carotid stenosis (n=1), arteriovenous malformation (n=1), and cervical neurofibroma (n=1). There were 12 diagnostic angiograms and 13 interventional angiograms. The left transradial approach was chosen due to left vertebrobasilar pathology (n=22), right subclavian stenosis (n=2), and previous right arm amputation (n=1). There was one instance of radial artery spasm, which resolved after catheter removal, and one conversion to transfemoral access in an interventional case due to lack of distal catheter support. There were no procedural complications.
Conclusions Left transradial access in diagnostic and interventional cerebral angiography is a technically feasible, safe, and an effective alternative when indicated, and may be preferable for situations in which pathology locations or anatomic limitations preclude right-sided radial access.
- angiography
- artery
- technique
Statistics from Altmetric.com
Introduction
Cerebral angiography has seen a recent shift toward transradial access instead of traditional transfemoral access out of concerns for patient preference and safety.1–5 In neurovascular centers across the USA in 2016, up to 4.5% of mechanical thrombectomies for acute ischemic stroke were performed via transradial access.6 This trend follows the lead of interventional cardiologists who reportedly pursue transradial access in 36% of their total angiographies and 28% of acute interventions in the USA, with up to 80% of cardiac cases performed via transradial access worldwide.7 8
The radial artery is typically accessed in the right arm, but there are a number of clinical scenarios in which access from the left arm may be advantageous—for example, left vertebral artery pathology or anatomic limitations of the right radial artery. The purpose of this multi-institutional study was to evaluate the technical feasibility and safety of left transradial access for cerebral angiography.
Methods
After Institutional Review Board approval, a retrospective review of the electronic medical records was conducted to examine outcomes in consecutive patients undergoing cerebral angiography via left transradial access across three institutions between January 2018 and July 2019. In addition to identifying indications for left transradial access, data collection included relevant clinical and demographic information (age at time of procedure, sex, body mass index, comorbidities, underlying pathology, operative details, and any complications associated with the procedure). Outcome variables included successful catheterization, access site complications, and fluoroscopic time. Descriptive statistics were used to characterize the population and are presented as mean±SD unless otherwise indicated.
For each procedure, despite left transradial access, the operator stands on the patient’s right side and the equipment orientation remains identical to that of transfemoral or right transradial access. Left transradial access is facilitated by separate sterile prepping of the patient’s left forearm, which is positioned across the patient’s abdomen to lie close to the right femoral artery access site (figure 1). This permits the operator to access the left wrist from the right side of the patient without standing on the left side of the table or reconfiguring any equipment. Positioning the patient in this way also brings the left radial access site close to the right wrist and right groin, in case additional or alternative arterial access is needed. Catheterization of the great vessels is also analogous to right-sided transradial angiography,1 with the exception that, when using the Simmons catheter, the curve is formed in the descending rather than the ascending aortic arch (figure 2 and online supplementary video 1).
Supplementary video

Patient positioning for left transradial access. The left wrist (arrow) with sheath in place is positioned over the abdomen, permitting easy and ergonomic access from the patient’s right side. The right wrist and right groin (asterisks) are also accessible.
{kind=link}
{kind=link}
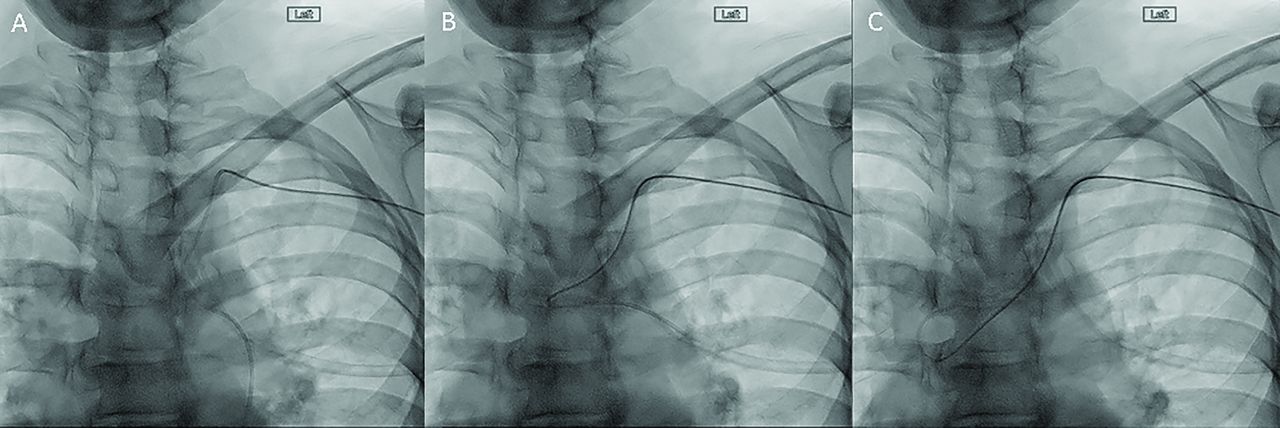
Forming the Simmons catheter from the left subclavian. (A) After the wire and catheter are placed in the descending aortic arch, the wire is pulled back into the straight portion of the Simmons catheter. (B) The catheter is pushed, forming the Simmons curve in the ascending aortic arch. (C) Once formed, the catheter can be used to select the great vessels from the ascending aorta.
Results
During the study time period, 25 left transradial cerebral angiograms were performed in 19 patients across three institutions. Radial access was performed as previously described1 2 via either the traditional access point (three fingerbreadths above the palmar crease; n=14) or via the distal radial artery in the anatomic snuffbox (n=11).9 The snuffbox approach was used to preserve the traditional access point for future interventions, if needed. A total of 11 patients (58%) were female. The average patient age was 56.1±16.6 years and the average body mass index was 28.4±5.9 kg/m2 (table 1). The indications for left transradial access are shown in table 1 and fell into two broad categories: pathology best reached via the left vertebral artery (n=14; left vertebral artery dominance or left vertebral artery pathology) or inability or inconvenience in gaining arterial access from the right radial artery (n=5; amputation of right upper extremity, subclavian stenosis, iliac artery stents). Pathology consisted of posterior circulation aneurysms (n=13), anterior circulation aneurysms (n=2), a basilar thrombus (n=1), bilateral carotid stenosis (n=1), arteriovenous malformation (n=1), and a cervical neurofibroma encircling the vertebral artery (n=1). Two patients (patients 1 and 4) had acutely ruptured aneurysms.
Patient demographics
Table 2 shows the operative details from the 25 angiograms. A 5 Fr sheath was used for diagnostic procedures and a 6 Fr or 7 Fr sheath for interventional procedures. In one procedure (patient 16), a 90 cm 6 Fr sheath was used to support Pipeline-assisted coiling. The left vertebral artery was successfully catheterized during 23 (92%) procedures; in two procedures it was not attempted because the pathology was located elsewhere. Twelve angiograms were performed for diagnostic purposes only and had an average fluoroscopy time of 6.6±7.6 min. The average fluoroscopy time per vessel during diagnostic angiography was 4.0±2.8 min.
Procedural details
The procedure for one of these cases (patient 2) was aborted due to vasospasm in the radial artery, but only after the angiogram of the vessel of interest had been completed.
Thirteen interventional procedures were performed, including endovascular repair of 11 aneurysms, one sacrifice of a left vertebral artery, and one aspiration thrombectomy for basilar occlusion. The average fluoroscopy time for interventions was 45.9±26.2 min. Only one intervention procedure, an attempted stent coiling of an unruptured anterior communicating artery aneurysm, had to be aborted due to inability to track the guide catheter into the internal carotid artery (patient 3). This patient had right-sided subclavian stenosis precluding right radial catheterization, and the procedure was successfully completed via transfemoral access. No patient in the cohort suffered any procedure-related complications.
Discussion
These results show that left radial access can be safe and technically feasible for both diagnostic cerebral angiography and interventional procedures when treating complex left-sided pathology or when it is not possible to achieve access from the right radial artery.
Currently, the femoral artery remains the preferred access point among many proceduralists due to its large diameter, easy compression to the femoral head, anatomic familiarity, and catheter design. However, femoral access has several notable disadvantages. Vascular complications such as bleeding, pseudoaneurysms, arteriovenous fistulas, retroperitoneal hematomas, and limb ischemia are seen in approximately 1% of transfemoral angiograms, with increased risk for obese patients and those on antiplatelet or anticoagulation therapy.10
In contrast, transradial access has a rate of 0.1–0.2% for similar vascular complications.11 Other common complications include a 5% rate of asymptomatic temporary or permanent radial arterial occlusion and a 10% rate of arterial spasm despite standardized preventative spasmolytic measures.2 Importantly, the vascular complications associated with transradial access tend to be relatively benign compared with those experienced with transfemoral access: in coronary angiography, transradial procedures are associated with a 29% decrease in 30-day mortality and a 17% decrease in 1-year mortality, with a 78% risk reduction in hemorrhagic complications and 80% decrease in blood transfusions compared with transfemoral procedures.12–17 Conversion from transradial to transfemoral access has been reported in 1–7% of cases,18 and our study reports similar results with one in 25 procedures (4%) converting from transradial to transfemoral access.
Patient preference for transfemoral or transradial access has also been studied. One study found 71% of patients favored transradial access, citing concern for increased bleeding risk with transfemoral access, worse discomfort with femoral artery puncture, and more easily tolerated postoperative mobility precautions.19 Another study of 98 patients who underwent both transfemoral and transradial cerebral angiography found that 94% of patients preferred the transradial approach.5 Reduced hospitalization times and lower rates of complications associated with transradial access may also translate into lower healthcare costs.20
Although left transradial access is rarely reported for cerebral angiography, interventional cardiologists have reported extensive experience. The most commonly perceived pitfalls for left transradial access include increased procedural time and operator discomfort. However, Larsen et al found no difference in mean procedural time, procedural success rate, or postoperative complications among right and left radial arterial access for acute coronary interventions.21 Studies have reported that left transradial access does not increase contrast load for the patient and may even decrease radiation exposure for the operator.22 23 Others have shown that operator discomfort during left transradial access is only a factor during arterial puncture and can be mitigated by moving the patient’s arm closer to midline or across the abdomen.24 Interestingly, one study of cerebral emboli during cardiac catheterization found a reduced incidence when procedures were performed via left transradial access compared with the right.25
In this study we found two broad categories of indications for performing left transradial access: location of pathology and anatomic limitations. In most patients in this cohort the location of pathology could be more easily accessed via the left vertebral artery. Selective catheterization of the left internal carotid artery or left vertebral artery may be better facilitated by left transradial access, particularly if the patient has acute angles between the right brachiocephalic trunk and the ascending aorta. Furthermore, a tortuous right subclavian artery may persuade the operator to consider left transradial access, as would isolated left vertebral or left internal carotid pathology. While left vertebral artery catheterization is possible via the right radial artery,26 catheter design and anatomic angles make such catheterization less likely to be successful compared with the direct anatomic access from the left subclavian artery afforded by left transradial access.
In the second group of patients, both transfemoral and right transradial access were considered less suitable procedures due to anatomic limitations. For example, patient 2 had multiple traumatic amputations of other limbs, while patients 3 and 18 both had right subclavian stenosis and prior bilateral iliac artery surgical repair. Faced with these limitations, left transradial access was performed to attempt to harness the benefits of the transradial approach.
This retrospective study has some limitations, including potential bias in patient selection. Furthermore, the variety of pathologies and the relatively low number of patients precludes substantial statistical analysis. This study does not compare results with right transradial or transfemoral procedures. However, the purpose of this study was to identify patients across three institutions in which left transradial access was used and to characterize the feasibility and safety of this approach in this patient cohort.
Conclusions
Left transradial access is a safe, effective, and technically feasible alternative for vascular access in diagnostic and interventional cerebral angiography, and may be preferable for certain situations in which pathology location or anatomic limitations preclude right-sided transradial access.
Acknowledgments
The authors appreciate the assistance of Sharon Durfy with manuscript preparation.
References
Footnotes
Contributors All authors contributed to the study design, data acquisition, data interpretation and/or manuscript drafting and revision, and each provided final approval of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests JWO reports grants and personal fees from MicroVention and personal fees from Terumo Medical and Microbot. MRL reports equity interest in eLoupes Inc, Cerebrotech, and Corindus, and has unrestricted educational grants from Stryker, Medtronic, and Philips Volcano. ECP is a consultant to Stryker Neurovascular, Penumbra, Medtronic Neurovascular, and Cerenovus, and a shareholder in RIST Neurovascular. MW is a consultant to Medtronic.
Patient consent for publication Not required.
Ethics approval This research was reviewed and approved by the University of Washington Institutional Review Board, Study Number 00006662.
Provenance and peer review Not commissioned; externally peer reviewed.