Article Text

Abstract
Introduction Transradial artery access (TRA) for cerebrovascular angiography is increasing due to decreased access site complications and overwhelming patient preference. While interventional cardiologists have reported up to 10 successive TRA procedures via the same radial access site, this is the first study examining successive use of the same artery for repeat procedures in neurointerventional procedures.1
Methods We reviewed our prospective institutional database for all patients who underwent a transradial neurointerventional procedure between 2015 and 2019. Index procedures were defined as procedures performed via TRA after which there was a second TRA procedure attempted. Reasons for conversion to a transfemoral approach (TFA) for subsequent procedures were identified.
Results 104 patients underwent 237 procedures (230 TRA, 7 TFA). 97 patients underwent ≥2 TRA procedures, 20 patients >3, four patients >4, three patients >5, and two patients >6 TRA procedures. The success rate was 94.7% (126/133) with 52% (66/126) of successive procedures performed via the same radial access site (snuffbox vs antebrachial) while the alternate radial artery segment was used for access in 48% (60/126) of subsequent procedures. There were seven (5.3%) cases requiring crossover to TFA, six cases for radial artery occlusion (RAO) and one for radial artery narrowing.
Conclusion Successive TRA is both technically feasible and safe for neuroendovascular procedures in up to six procedures. The low failure rate (5.3%) was primarily due to RAO. Thus, even without clinical consequences, strategies to minimize RAO should be optimized for patients to continue to benefit from TRA in future procedures.
- transradial approach
- radial access
- angiography
- endovascular
- repeat
- radial artery occlusion
- neurovascular
- neurointervention
Statistics from Altmetric.com
- transradial approach
- radial access
- angiography
- endovascular
- repeat
- radial artery occlusion
- neurovascular
- neurointervention
Introduction
The transradial approach (TRA) for cerebral angiography and interventions is increasingly used due to overwhelming evidence demonstrating a decrease in access site complications, improved patient preference, and cost reduction when compared with traditional transfemoral access (TFA).2–4 Led by the interventional cardiology community, multiple large randomized multicenter trials as well as meta-analyses have reported a greater than 60% reduction in vascular complications as well as significant decreases in all-cause mortality and net adverse clinical events with TRA.3 5–11 Despite the many advantages of TRA, there are also limitations including radial artery occlusion (RAO) and radial artery spasm.12 RAO is the most frequent complication of radial procedures with a reported incidence of 1–6%.13 14 While RAO is almost always asymptomatic due to the ulnar–palmar collateral vascular blood supply of the hand, persistent RAO precludes the use of radial artery access in any future interventions. Judicious practice of RAO prevention strategies has allowed interventional cardiologists to perform up to 10 successive TRA procedures via the same radial access site.1 However, neuroendovascular procedures often require larger catheter systems than interventional cardiology procedures to navigate tortuous cervical and cerebral anatomy. In this study we report the feasibility of performing repeat TRA in patients undergoing neuroendovascular procedures.
Methods
Following IRB approval, we reviewed our prospective institutional database for all consecutive patients who underwent a complete transradial neurointerventional procedure between October 2015 and July 2019 with at least one subsequent attempted or completed TRA procedure. Patient demographics, procedural details, clinical data, and subsequent neurointerventional procedures were recorded.
During the study period, operators included three neurointerventionalists (DRY, RMS, ECP) and six neurointerventional fellows (BS, SS, JC, PK, MCB, SC). We have previously described the set-up and technical details of our transradial procedures.4 12 15–19 Diagnostic cerebral angiography was performed with a 100 cm hydrophilic coated 5 French Simmons 1, Simmons 2, or Simmons 3 catheter through a 5 French radial sheath. Neurointerventions included a wide variety of procedures including balloon angioplasty, stenting, coiling, flow-diverting stent placement, embolization with liquid embolic agents, intra-arterial chemotherapy administration, and mechanical thrombectomy. All interventions required a 6 French or larger system. The radial sheath is removed immediately following completion of the procedure and patent hemostasis is achieved with a TR band. Per protocol the band is deflated after 30 min.
Approach selection and catheter choices were at the discretion of the operator and not standardized. Transradial access was defined as access that permitted completion of the neuroendovascular procedure. An index procedure was defined as any completed TRA procedure with a subsequent attempt at performing a second neuroendovascular procedure via TRA. TRA failure describes conversion to TFA after attempted radial access.
Results
During the study period a total of 104 patients underwent 237 neurointerventional procedures (230 TRA procedures and 7 TFA procedures). The mean age of the cohort was 57.5 years at the time of the index procedure and 67.3% (70/104) of patients were female. All TRA procedures were performed via the right radial artery. The distal radial artery in the anatomical snuffbox was accessed in 75 procedures and the conventional antebrachial radial artery was used in the remaining 155 procedures.
There were a total of 133 index TRA procedures including 83 (62.4%) diagnostic cerebral angiograms and 50 (37.6%) neurointerventions (table 1) . There were no clinically significant access site complications. The success rate of repeat TRA procedures was 94.7% (126/133). Ninety-seven (93.2%) patients underwent ≥2 TRA procedures; 20 (19.2%) patients >3, four (3.8%) patients >4, three (2.9%) patients >5, and two (1.9%) patients >6 TRA procedures. The median time between TRA procedures was 161 days (range 0–674). Sixty-six of the 126 successive procedures (53%) were performed via the same access site (distal vs antebrachial radial artery) while the alternate radial artery segment was used for access in the remaining 47% (60/126) of subsequent procedures (table 2).
Procedural characteristics of index procedures
Procedural characteristics of successful repeat transradial procedures
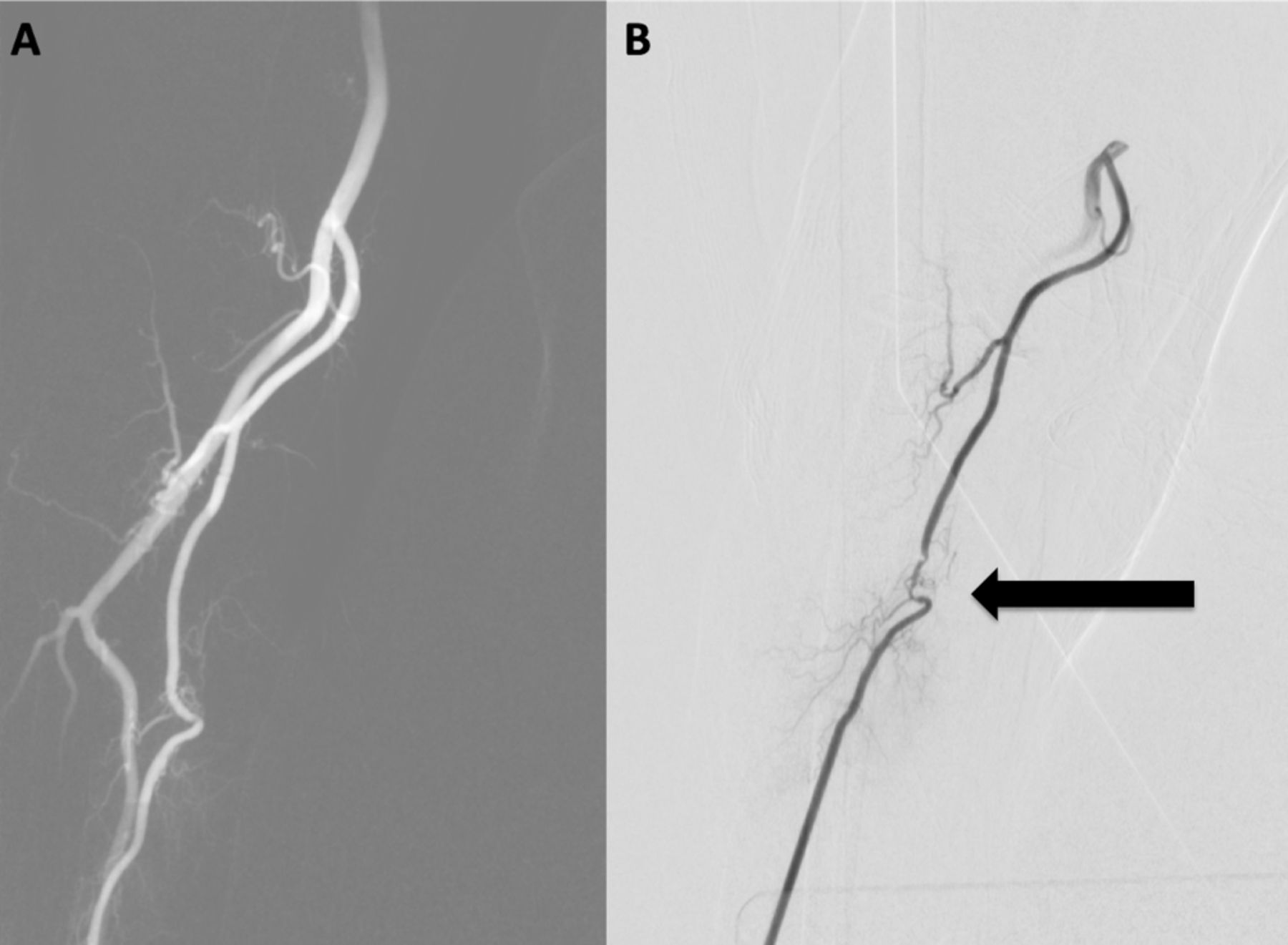
In 5.3% (7/133) of index cases, a repeat TRA procedure was attempted but converted to TFA. Of these, access could not be obtained in six patients due to RAO and one patient had significant narrowing of the radial artery on the radial angiogram necessitating conversion to femoral access (figure 1). Among the seven patients, two had an 0.088 inch guide catheter placed as a shuttle through the conventional radial artery site to perform the index intervention, one patient had a 6 French radial sheath, while the remainder were associated with a 5 French radial sheath. The median time between procedures was 181 days (range 15–207 days).

(A) Index procedure radial artery angiogram demonstrating appropriate size radial artery. (B) Subsequent radial artery angiogram 41 days later during planned coil embolization demonstrating focal narrowing of radial artery (arrow). Due to the need for a minimum 6 French system in this case, we did not attempt to cross stenosis and converted to transfemoral access.
Discussion
Our study demonstrates the feasibility and safety of repeat TRA procedures in up to six successive procedures without any clinical complications. Importantly, only 5.3% of repeat TR access attempts resulted in conversion to a transfemoral technique due to RAO or significant narrowing. While this conversion rate is low, it highlights the importance of preventive RAO strategies for repeat catheterization.
The superficial and distal location of the radial artery confers the benefit of easy positioning, peripheral access, and reliable compressive hemostasis. However, the significantly smaller size of the radial artery increases the risk of spasm and arterial occlusion. While rates of RAO are low (1–6%) and typically clinically silent, persistent RAO might preclude subsequent transradial procedures, thus subjecting the patient to the increased risks of a transfemoral procedure in the future.13
Our experience is consistent with previous studies within the interventional cardiology literature which have reported the feasibility of successive TRA in up to 10 repeated ipsilateral TRA procedures.1 20–24 Sakai et al reported a series of 812 patients undergoing 1539 transradial coronary procedures in which technical failure of radial access increased from 3.5% and 7.9% of men and women, respectively, at the time of the second radial procedure to 15.9% and 28.6% in men and women, respectively, at the time of the fifth procedure.22 Similarly, Abdelaal et al studied the outcome of repeat transradial procedures in 519 patients undergoing 1420 procedures (separated by ≥2 months) and found a 93% success rate for a single repeat radial access procedure.1 Their linear regression analysis estimated a 5% estimated failure rate associated with each successive attempt. The most common reasons for technical failure were vessel narrowing or occlusion, although all patients were asymptomatic.
Progressive luminal narrowing of the radial artery has been reported following transradial procedures. Studies using intravascular ultrasound, optical coherence tomography, or histology have demonstrated alterations of the radial artery such as intimal damage, inflammation, and medial dissection after TRA coronary interventions.25–28 These endothelial changes may trigger a cascade of events promoting thrombus formation acutely as well as intimal hyperplasia with progressive narrowing over time. An acute radial artery thrombus may limit early repeat access, but recanalization occurs >50% of the time.29 Yoo et al evaluated mean radial artery diameters and found a mean reduction of 0.14±0.11 mm in radial artery diameter over 4.5±4.1 months after initial use of radial artery; however, there was no significant decrease in the success of repeated procedures.24
While similar results can be expected in the cerebrovascular patient population, neurointerventions often require larger systems for more tortuous anatomy and lengthier procedures. In this study we demonstrate the feasibility of repeated radial access for neuroendovascular procedures with 97 patients successfully undergoing between two and six TRA procedures. However, RAO or narrowing necessitated conversion to TFA in 5.3% of cases. Previously reported risk factors for RAO after TRA catheterization include female gender, diabetes mellitus, low body mass index, high sheath to radial artery diameter ratio, procedural duration, heparin dose, and occlusive hemostasis.30 31 Similarly, in our cohort all crossover patients were women, average radial artery size was smaller although this difference was not significant (2.96 vs 2.24 mm, p=0.76), and 43% of cases were associated with use of 6 French or larger systems in the index procedure.
Thus, while neurointerventional procedures can be safely and successfully performed via 6 French and 7 French systems, their size may also increase the risk of RAO, precluding future TRA access. Accordingly, it is imperative to employ strategies to minimize the risk of RAO such as using the minimal size sheath or catheter that is necessary to accomplish the procedure, administering heparin and antispasmodics, and careful use of compression devices to close the arteriotomy with patent hemostasis.12 13 29
Additionally, this is the first series to use alternating distal radial artery access for diagnostic angiography and antebrachial radial artery access for interventions in order to minimize repeated trauma to the same arterial site within a short duration of time. While our results are promising, a prospective trial will be necessary to evaluate how timing of repeat procedures as well as alternating sites affects feasibility of repeat TRA procedures. Similarly, accessing the ulnar artery if it is larger than the radial artery or in cases of expected need for repeat access may decrease rates of post-access occlusion and maintain the longevity of accessibility in the antebrachial arteries. Finally, in cases of posterior circulation pathology where only left vertebral artery catheterization is needed, the left radial artery may be used as an alternative site.
The principal limitation of this study is the retrospective design and lack of standardized protocol for selecting the access site at our institution during the study period. The true RAO rate may not be accurately reflected, as TRA was not attempted in patients in whom a subsequent TFA procedure was planned after the initial TRA procedure for anatomical purposes such as subclavian tortuosity. Furthermore, we do not routinely perform delayed Doppler ultrasounds to evaluate radial artery patency. Finally, access and repeat procedures were performed by a number of operators with varying experience and comfort with TRA, which may have influenced the failure rate.
Conclusion
We present the first series demonstrating the technical feasibility and safety of repeat TRA for neuroendovascular procedures. Only 5.3% of cases resulted in conversion to a transfemoral technique due to narrowing or occlusion of the radial artery (figure 2). Differential use of antebrachial and distal snuffbox radial artery access sites may minimize the effect of local trauma to the artery. This is one of the many strategies that should be employed to improve RAO rates allowing patients to continue to benefit from the advantages of TRA in future procedures.

{kind=link}
{kind=link}
Flowchart describing access type and procedure performed in successful repeat TRA neuroendvascular procedures and reasons for failure. DTRA, distal transradial approach; DSA, digital subtraction angiography; RA, radial artery; RAO, radial artery occlusion; TRA, transradial approach.
References
Footnotes
Twitter @Starke_neurosurgery
Contributors All authors contributed to the conception, data gathering, and drafting of the manuscript. DRY, RMS, and ECP provided manuscript oversight and administrative support. All authors critically reviewed the manuscript and approved its final submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests DRY: Medtronic Neurovascular: Consultant, Cerenovus: Consultant, Rapid Medical and Neuralanalytics: Consultant. RMS: Medtronic Neurovascular: Consultant, Penumbra: Consultant, Cerenovus: Consultant, Abbott: Consultant. ECP: Stryker Neurovascular: Consultant, Penumbra: Consultant, RIST Neurovascular: Stockholder, Medtronic Neurovascular: Consultant, Cerenovus: Consultant.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.