Article Text

Abstract
Background The COVID-19 pandemic has disrupted established care paths worldwide. Patient awareness of the pandemic and executive limitations imposed on public life have changed the perception of when to seek care for acute conditions in some cases. We sought to study whether there is a delay in presentation for acute ischemic stroke patients in the first month of the pandemic in the US.
Methods The interval between last-known-well (LKW) time and presentation of 710 consecutive patients presenting with acute ischemic strokes to 12 stroke centers across the US were extracted from a prospectively maintained quality database. We analyzed the timing and severity of the presentation in the baseline period from February to March 2019 and compared results with the timeframe of February and March 2020.
Results There were 320 patients in the 2-month baseline period in 2019, there was a marked decrease in patients from February to March of 2020 (227 patients in February, and 163 patients in March). There was no difference in the severity of the presentation between groups and no difference in age between the baseline and the COVID period. The mean interval from LKW to the presentation was significantly longer in the COVID period (603±1035 min) compared with the baseline period (442±435 min, P<0.02).
Conclusion We present data supporting an association between public awareness and limitations imposed on public life during the COVID-19 pandemic in the US and a delay in presentation for acute ischemic stroke patients to a stroke center.
- stroke
- statistics
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Introduction
The SARS-CoV-2 virus pandemic and its clinical syndrome, COVID-19, is causing significant disruption to established care paths, including for acute conditions such as acute ischemic stroke. Since the initially slow recognition of the issue, a breakpoint was reached with the first reported death attributable to the novel coronavirus in the US on February 29, 2020. Public awareness has increased dramatically.1 During March 2020, several states in the US have declared a state of emergency and have implemented restrictions on business, travel, and social life.
There have been anecdotal reports of a reduction in cases of acute neurological injury, including acute ischemic stroke, and also reports in delays in presentation for both neurological and cardiac disease,2 suggesting that patients are not seeking timely and appropriate medical care for these conditions.3 On the other hand, some of the most seriously ill COVID-19 patients are presenting with cardiac symptoms.4 There is growing recognition that COVID-19 may not be confined to the respiratory system, and may even have neuro-invasive features that can lead to devastating hemorrhagic events.5–7 In some population-dense areas in the US, concerns about the incidence of strokes in younger patients with COVID-19 have been raised.8
Here we aim to quantify the influence of the COVID-19 pandemic on the timing of presentation of all acute ischemic stroke patients. We hypothesize that patients may be delaying care for stroke symptoms due to fears related to the pandemic.
Methods
We gathered an anonymized limited data set from comprehensive stroke centers at 12 participating institutions across six states, based on the prospective ongoing data collection that is entered into the American Heart Association ‘Get With The Guidelines’ (GWTG) database.9 We compared the period of February and March 2019 (the baseline period) to February 2020 (the ‘pre-COVID’ period) and March 2020 (the ‘COVID’ period). The grouping arose naturally from an analysis of Google searches (figure 1), denoting the relative interest of the search terms ‘COVID’ or ‘Coronavirus’ on the Google search engine. Consistent with the timeline of events surrounding COVID-19 in the US, there appears to be very little public awareness before March 1, 2020. Centers were selected based on their ability to respond to a rapid data request and range in characteristic from urban (eight) to suburban (three) to rural (one) location. No center was located in an area of resource exhaustion.

Google trends analysis of the relative interest in the search terms around COVID-19. The graph is scaled relative to the peak interest.
Each center contributed a consecutive list of patients who presented with an acute ischemic stroke as adjudicated by the GTWG database entry of the final diagnosis. The reported variables were limited to the calendar week of presentation, the interval between the ‘last-known-well’ timepoint (LKW) and the time of arrival to the reporting comprehensive stroke center in minutes, and the first documented National Institutes of Health Stroke Scale (NIHSS), which was considered a proxy for the severity of stroke presentation.
This research as done under the guidance of the Institutional Review Board and exempted (Geisinger IRB 2016–0483).
Statistical analysis
The study design is a retrospective, unspecified analysis of routinely and prospectively entered data of a standard quality database used to ensure quality standards for acute stroke patients. The structure of this database has been described before.8 Data were analyzed using JMP, Version 14.0 (SAS Institute Inc., Cary, NC). Groups were compared using Student’s t-test.
Results
Patient characteristics
From February to March 2019, designated the baseline period, 320 patients presented with a final diagnosis of acute ischemic stroke. In February 2020, designated the pre-COVID period, 227 distinct patients were analyzed. In March 2020, designated the COVID period, 163 patients were available for analysis, for a total of 710 patients analyzed.
The number of cases recorded by the week number of the year showed a general increasing trend in 2019, in line with the expectation of developing more optimal patient care pathways and systems of care.10 In the COVID period in 2020, we observed a drop in the absolute number of cases per calendar week (figure 2).
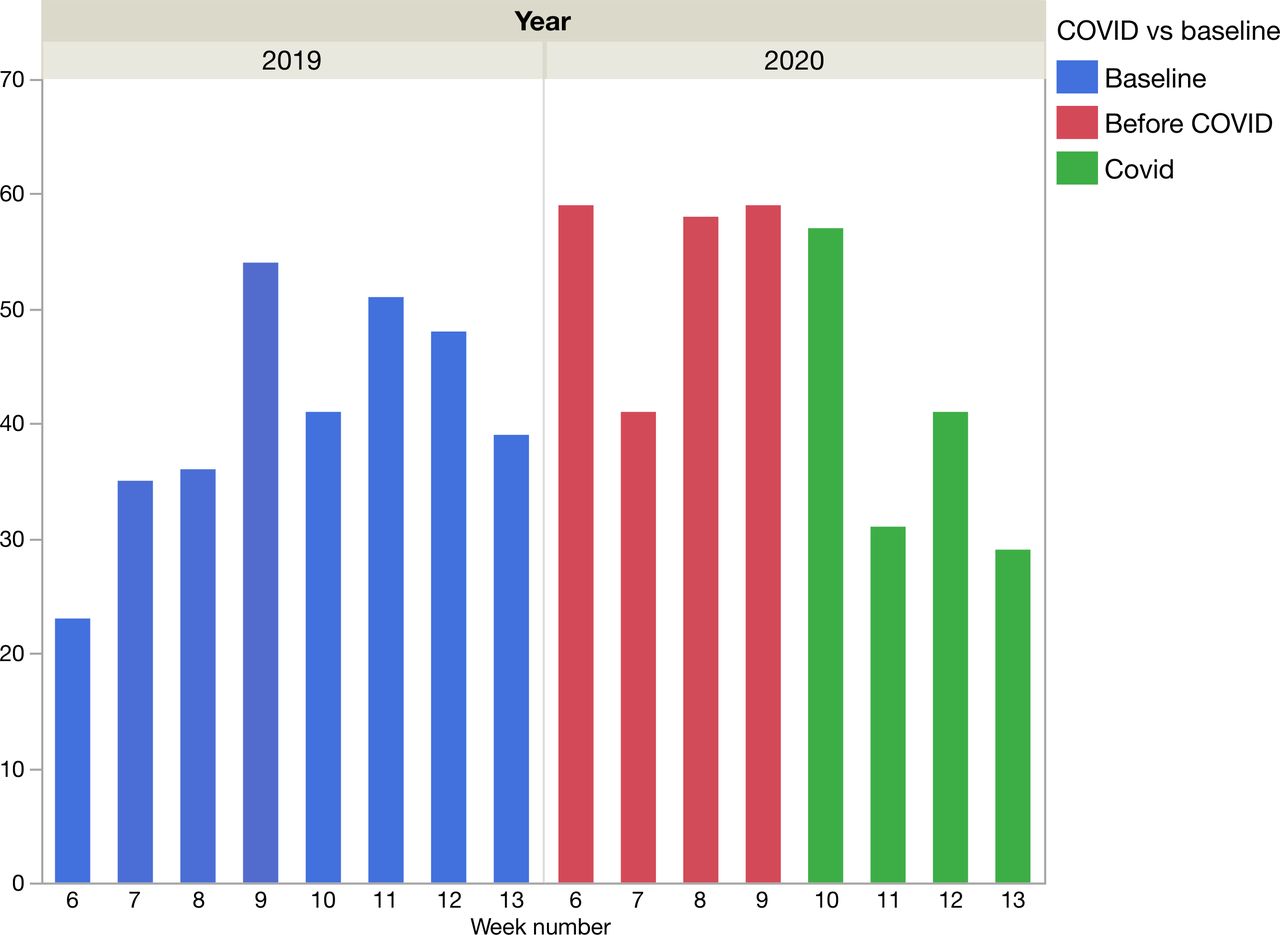
Development of the number of patients presenting with acute ischemic stroke per calendar week.
Stroke presentation
The median age was 70±14 (SD) years overall, The mean age of patients who presented in the baseline period was 67±15 years, slightly younger than in the pre-COVID period (70±14 years) and the COVID period (69±14 years)(see online supplementary figure 1). The difference between the baseline and the pre-COVID period was statistically significant (P<0.02), but there was no significant difference between the baseline and COVID or pre-COVID and COVID groups, P=0.07 and P=0.55, respectively.
Supplemental material
There was no significant difference between the severity of presentation, as the mean initial NIHSS was 9.2, 9.7, and 9.6 for the baseline, pre-COVID, and COVID period, respectively (P=0.79)(see online supplementary figure 2).
The mean time interval between LKW and presentation to the stroke center was 442±435 min for the baseline, 552±630 min for the pre-COVID, and 603±1035 min for the COVID period. The difference of 160 min average increase in time between LKW to presentation between the baseline period and COVID period was significant (P<0.03) (figure 3).

{kind=link}
{kind=link}
{kind=link}
Time interval between last-known-well time (LKW) and arrival at the stroke center (minutes).
We performed a sensitivity analysis to exclude an effect driven by strokes with less disabling presentations and excluded patients with NIHSS<=3 from the analysis. The mean LKW-presentation interval for patients with NIHSS >4 was 405±50 min for the baseline and 613±70 min for the COVID period, remaining significant (P<0.02).
Discussion
Stroke and resultant outcomes have considerable socioeconomic impact,11 and much time and effort have been spent over the past few years to standardize care recommendations12 and create systems of care.10 COVID-19 has been putatively linked to an increased incidence of cerebrovascular and cardiovascular events.8 13–15 A pooled analysis of several studies that have been published to date suggested that there is a 2.5-fold increase in the incidence of strokes and poor outcomes or mortality.16
Concomitantly there have been anecdotal reports from physicians in the US regarding a decrease in the number of acute cardiovascular and cerebrovascular emergencies, contrasted by some reports in the higher affected areas reporting an increase or concerns about the severity of strokes or the age of presentation,3 8 leading to conflicting perceptions of the overall stroke burden during the pandemic.
Our results suggest that there is another variable to consider, namely the delay of presentation. Similar results were reported in a limited study of cardiac interventions in Hong Kong in January 2020, in which substantial increases in time from symptom onset to medical contact were observed.2 This may be due to patients’ perceived concerns or outright fear of interacting with the healthcare system, leading to reluctance in seeking medical help shortly after symptom onset. Delays in care have been described in other settings, including heart failure and (during COVID-19) tuberculosis.17 18 The common thread is that the factors leading to delays when seeking care are poorly understood and generally not well studied but include factors such as fear, embarrassment, and well-being.
In the case of this current pandemic, we show an increase in the mean interval between the LKW time and the time of presentation to the hospital. We have shown no change in stroke severity in the cohort described in comparison to the baseline, though the full effect of the pandemic is still not known. The result remains significant when excluding less severe strokes with NIHSS<=3. Seeking care as early as possible remains paramount since a delay in stroke treatment has long-lasting consequences.12 Public measures imposing social distancing, stay-at-home, or shelter-in-place orders are necessary measures to limit the spread of COVID-19. However, they may have the unintended effect of increasing the perceived downsides of seeking care for non-COVID related diseases, leading to delayed care and worse outcomes.
Our work does not incorporate emergency medical services (EMS) activation rates or the interval between LWK and the activation of EMS which may be a potentially more granular time interval to study the delay between onset of symptoms and seeking care. Unfortunately, no systematic data collection was available for analysis and depending on the geography a variable number of patients are brought to the hospital directly.
Our analysis points to the need for a public education campaign. A future additional resurgence of COVID-19 or other pandemic outbreaks could occur. Helping the public to understand the more imminent risks may avoid additional burden on the healthcare system and improve the recovery potential of the patients.19 20 We have limited information about the impact of patient screening protocols on the transfer of patients. Widespread testing of asymptomatic patients had not been implemented in the US during the study period, and we do not believe that non-testing screening protocols can account for the difference seen in our results.
Limitations of this study include the limited dataset gathered, which is reflected in the relatively small number of stroke centers included, necessitated by the need to respond to a rapid data request and the related limited geographic sampling across the US. Similarly, the rapidly changing landscape of the COVID-19 pandemic, including more definitive effects of social distancing may not yet be captured in this dataset. We do not attempt to analyze the difference in referral pattern and patient flows between different centers in this study, nor does this analysis take the intermediate stop or bypass of a first hospital or stroke center into account. We assume that all factors that would contribute to the aggregate efficiency of the stroke referral system of the centers included here remains at least stable if not improved between the baseline and the COVID period. This is based on the systematic process improvement efforts that all stroke centers are engaged in. These efforts are typically directed toward reducing intervals from door to needle or revascularization. We correlate the presence of COVID-19 as a single changed variable but do not believe that other confounders would be able to explain the significant effect size demonstrated in our results.
Conclusion
In this work, we present new data supporting that the outbreak of the COVID-19 pandemic in the US is associated with a delay in presentation of patients with acute ischemic stroke. We urge policymakers and patient advocates to consider these results in future decision making and raise awareness of the need for patients to seek appropriate and timely medical attention for stroke symptoms, even in the face of the current or future pandemic crisis.
References
Footnotes
Twitter @ClemensSchirmer, @MayfieldChair, @AdamArthurMD, @wchrisfox, @DrMichaelLevitt
Contributors Planning CMS, AMS, AJR, reporting all authors, conception and design CMS, AMS, acquisition of data or analysis all authors, interpretation of data CMS, editing, and approval of manuscript all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests CMS: Research Support: Penumbra, Shareholder Neurotechnology Investors. ASA: Consultant for Johnson and Johnson, Medtronic, Microvention, Penumbra, Scientia, Siemens, Stryker, Research support from Balt, Cerenovus, Medtronic, Microvention, Penumbra, Siemens, and Stryker, Shareholder in Bendit, Cerebrotech, Endostream, Magneto, Marblehead, Neurogami, Serenity, Synchron, Triad Medical, Vascular Simulations. WCF: Consultant for NuVasiveJames: Shareholder, Remedy Pharmaceuticals. MRL: Research support from Stryker, Medtronic, Philips Volcano, Shareholder in Cerebrotech, Synchron, eLoupes. RT: Shareholder in Medtronic. EV: Patentholder with Penumbra, Mizuho, Consultant for Toshiba. AMS: Consultant Penumbra, Cerenovus, Stryker, Terumo, Research support Penumbra.
Patient consent for publication Not required.
Ethics approval Geisinger IRB 2016-0483.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available. Data in GWTG database.