Article Text

Abstract
Background The novel coronavirus disease 2019 (COVID-19) pandemic is still spreading across the world. Although the pandemic has an all-round impact on medical work, the degree of its impact on endovascular thrombectomy (EVT) for patients with acute ischemic stroke (AIS) is unclear.
Methods We continuously included AIS patients with large artery occlusion who underwent EVT in a comprehensive stroke center before and during the Wuhan shutdown. The protected code stroke (PCS) for screening and treating AIS patients was established during the pandemic. The efficacy and safety outcomes including the rate of successful reperfusion (defined as modified Thrombolysis In Cerebral Infarction (mTICI) graded 2b or 3) and time intervals for reperfusion were compared between two groups: pre-pandemic and pandemic.
Results A total of 55 AIS patients who received EVT were included. The baseline characteristics were comparable between the two groups. The time from hospital arrival to puncture (174 vs 125.5 min; p=0.002) and time from hospital arrival to reperfusion (213 vs 172 min; p=0.047) were significantly prolonged in the pandemic group compared with the pre-pandemic group. The rate of successful reperfusion was not significantly different between the two groups (85.7% (n=18) vs 88.2% (n=30); OR 0.971, 95% CI 0.785 to 1.203; p=1.000).
Conclusion The results of this study suggest a proper PCS algorithm which combines the COVID-19 screening and protection measures could decrease the impact of the disease on the clinical outcomes of EVT for AIS patients to the lowest extent possible during the pandemic.
- thrombectomy
- stroke
- intervention
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Introduction
Although the pandemic of the novel coronavirus disease 2019 (COVID-19) in China has been brought under control to some extent, as indicated by the end of the Wuhan shutdown on April 8, 2020, the virus is still spreading rapidly around the rest of the world and it is too early for us to ease off. Official data from the website of the World Health Organization (WHO) showed that up to April 14, more than 1 840 000 patients were diagnosed as confirmed cases all over the world, including 117 021 deaths.1
During the pandemic, almost all elective operations have been deferred or even stopped because of the need for SARS-CoV-2 infection prevention and relocation of limited medical resources.2 Emergency surgeries such as endovascular thrombectomy (EVT) for acute ischemic stroke (AIS) must be performed without any delay even during the pandemic, in order to rescue important functions and save lives.3 4 However, the impact of the pandemic may be inevitable, because the hospitals have to take the necessary measures to prevent further spread of SARS-CoV-2 among medical personnel and patients.2 It can be expected that, given the current situation of the pandemic, strict prevention and control measures will remain and be implemented across the world for at least the next few months. It is still unclear whether the evaluation and treatment process and clinical outcomes of AIS patients who need EVT have been affected, and what we can do to ensure the quality of treatment of AIS patients as well as avoid the spread of SARS-CoV-2 during the pandemic.
Therefore, based on the data from a comprehensive stroke center, we compared the evaluation and treatment process as well as clinical outcomes of AIS patients who underwent EVT before and during the pandemic, with the aim of evaluating the impact of the pandemic on the process and outcome of EVT implementation for AIS patients.
Methods
Patient selection and data collection
We continuously included all AIS patients treated with EVT in a comprehensive stroke center between January 23 and March 7, 2020 (44 days in total from the date of the Wuhan shutdown to the date of no newly confirmed cases locally) as the pandemic group. Similar patients with the same time span (44 days) between December 1, 2019 and January 14, 2020 were included as the pre-pandemic group. The Stroke Code team in our center was composed of seven attending physicans, five residents, eight nurses, five technicians and three anesthetists. All confirmed and suspected COVID-19 patients were transferred to designated hospitals in accordance with the guidelines of the National Health Commission5 and thus excluded from this study. The following data were obtained from our prospective database: patient demographics, past medical history, presenting National Institutes of Health Stroke Scale (NIHSS), Alberta Stroke Program Early CT Score (ASPECTS), site of thrombus, side of thrombus, therapeutic interventions, preintervention and postintervention modified Thrombolysis In Cerebral Infarction (mTICI) scores, time from onset to hospital arrival, time from hospital arrival to groin puncture, time from groin puncture to first recanalization attempt, time from hospital arrival to first recanalization attempt, time from onset to first recanalization attempt, procedures (stenting, angioplasty, stent retriever, and/or aspiration thrombectomy), time from groin puncture to successful reperfusion, device used for thrombectomy, procedure-related complications, other complications, and post-procedure NIHSS scores. These data were obtained from our Electronic Medical Records System (EMRS) and workstation of Picture Archiving and Communication System (PACS) for digital subtraction angiogram. The study was approved by the ethics committee of our hospital.
Protected code stroke
The regular code stroke algorithm was used to prioritize the hyperacute assessment and care of a patient presenting with clinical manifestations for stroke.6 However, during the pandemic, the algorithm needed to be modified to the protected designation to provide an additional layer of protection for patients and medical personnel who were engaged in triage, rapid assessment, and treatment of patients.6 Herein, we established a protected code stroke (PCS) for AIS patients who need EVT during the pandemic based on expert consensus from the Chinese Federation of Interventional and Therapeutic Neuroradiology and the Chinese Society of Cardiology (figure 1).7 8
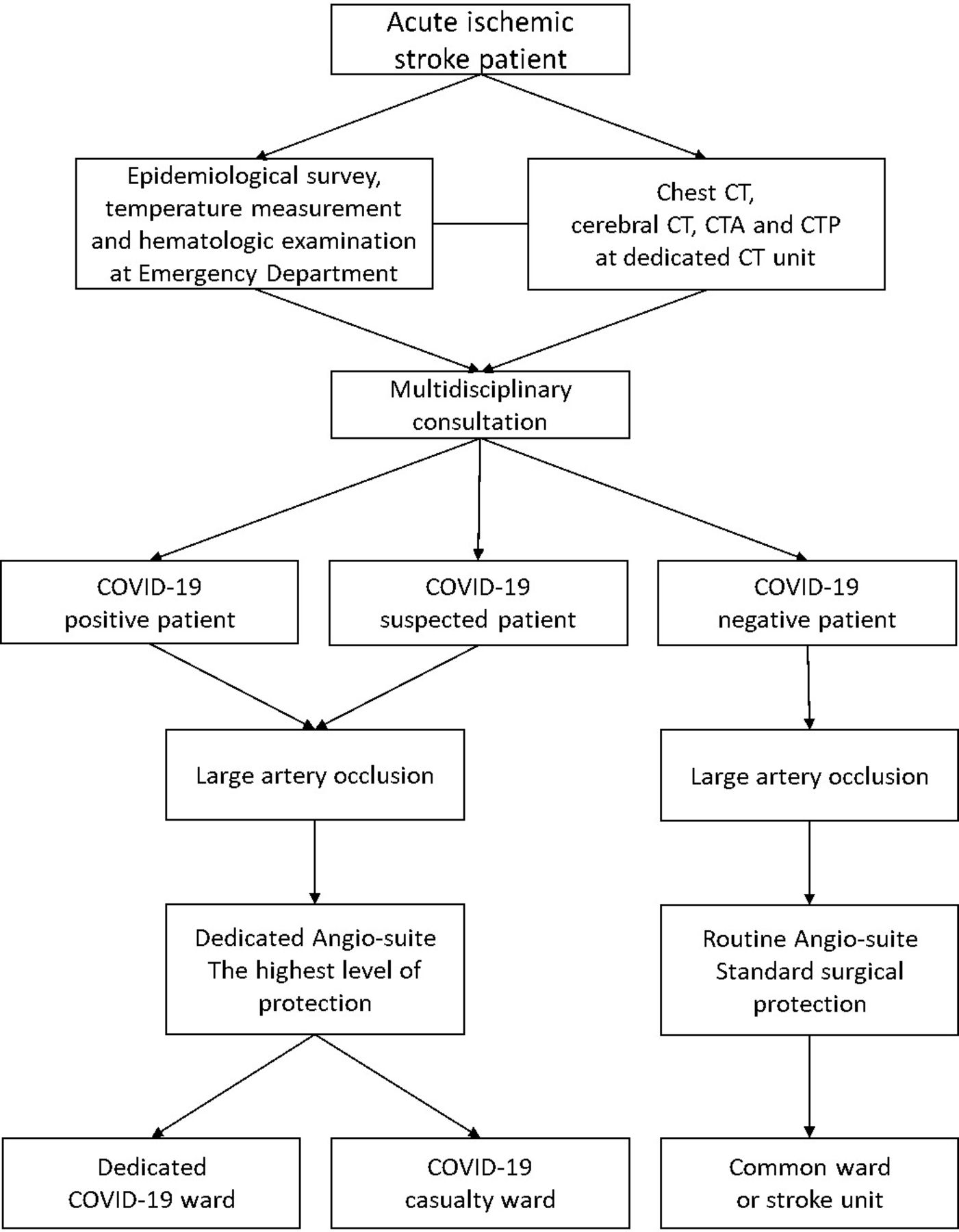
The screening and interventional process for acute ischemic stroke patients during the COVID-19 pandemic. CTA, CT angiography; CTP, CT perfusion.
On arrival at the emergency department (ED), each patient was screened and evaluated for AIS by a stroke team. The personnel at the ED were equipped with adequate personal protective equipment (PPE). Additional screening for COVID-19, including travel history, body temperature measurement, complete blood count and chest CT, were performed simultaneously. The patient triage was done by multidisciplinary consultation based on the above screening results, as shown in figure 1. In short, COVID-19 clinically negative patients who needed EVT were treated in a routine angio-suite with standard surgical protection. COVID-19 clinically positive or suspected patients were treated in a dedicated angio-suite with the highest level of protection and transferred to a dedicated COVID-19 ward (for positive cases) or COVID-19 casualty ward (for suspected cases) after the procedure. The involved personnel were pre-alerted for adopting adequate PPE. A real-time reverse transcriptase-polymerase chain reaction (RT-PCR) assay for COVID-19 nucleic acid was not a routine test for AIS patients because of the limited access at the early stage of the pandemic and the urgent nature of evaluation and treatment for AIS. Only clinically confirmed and suspected cases diagnosed by multidisciplinary consultation according to the guidelines of the National Health Commission5 received further nucleic acid testing. The regular angio-suites in our center do not contain a negative-pressure system, so were unsuitable for the treatment for patients with an infectious disease like COVID-19. We therefore converted one of the regular angio-suites into a dedicated angio-suite with a negative-pressure system immediately after the outbreak of the pandemic, in order to meet the necessary requirements.
Procedure
Local anesthesia was recommended during the procedure, but general anesthesia was chosen if the patient was irritable and uncooperative. Intravenous heparin would be administered if thrombolysis was not performed. Any mechanical stent retriever (Solitaire, Medtronic and Trevo, Stryker; Irvine, CA, and Freemont, CA, respectively) or aspiration catheter (Penumbra System, Penumbra, Alameda, CA) and distal access catheter (Navien, Medtronic, Sofia Plus, MicroVention and Catalyst, Stryker; Irvine, CA, Tustin, CA and Freemont, CA, respectively) were approved for use. Any procedure such as a direct aspiration first-pass technique (ADAPT), stent retrieval, or stent retriever combined with aspiration (Solumbra technique) was permitted to be performed.9–11 The decisions as to whether to use a rescue therapy and which technique to use were left at the discretion of the surgeon. Permitted rescue techniques were intra-arterial tirofiban and angioplasty with or without stenting. Angiographic success was defined as achieving thrombolysis in mTICI grade 2b or 3.
Outcomes
The primary outcome was the rate of successful reperfusion defined as an mTICI grade 2b or 3 assessed on angiography.
Secondary outcomes included the change in the NIHSS score from baseline to 3 days after the procedure, and the safety outcome which was defined as a composite of all-cause mortality at 3 days after the procedure, intracerebral hemorrhage (ICH) on brain imaging at 24±12 hours after the procedure, and procedure-related serious adverse events (arterial perforation, arterial dissection, and subarachnoid hemorrhage (SAH)).
Statistical analysis
Categorical variables are reported as frequencies and percentages. Quantitative variables are reported as mean±SD or median (IQR) for non-normal distribution. Differences in continuous variables were assessed with the Mann-Whitney U test with non-normal distribution. Differences between proportions were assessed with the χ2 test or Fisher’s exact test. Differences were considered statistically significant at p<0.05. Data were analyzed using SPSS version 22.0 software package (IBM Corp, Armonk, NY).
Results
Baseline characteristics
A total of 167 AIS patients were screened in the ED; 112 of them were declined for EVT due to low NIHSS scores, high modified Rankin Scale (mRS) scores, no obvious mismatch on multimodal CT scan, no evidence of large artery occlusion or refusal to undergo EVT. Fifty-five patients (mean±SD age, 65.1±13.1 years; 37 men (67.3%)) with AIS caused by intracranial large artery occlusion were finally included (table 1): 34 (61.8%) in the pre-pandemic group and 21 (38.2%) in the pandemic group, treated before and during the Wuhan shutdown, respectively. No statistically significant differences in all baseline characteristics were found between the two groups. All 21 patients in the pandemic group went through additional screening for COVID-19, including chest CT scans and multidisciplinary consultations during the evaluation process. One patient was screened as a clinically suspected case of COVID-19 and PCS was launched throughout the procedure until the diagnosis of COVID-19 was ruled out by further examinations. The median (IQR) preoperative NIHSS score was 13 (11–17) in the pre-pandemic group and 12 (11–18) in the pandemic group (p=0.537). The median baseline ASPECTS and time from symptom onset to hospital arrival in both groups were similar. None of our team members has been infected by SARS CoV-2.
Baseline characteristics of AIS patients treated with EVT in the pre-pandemic and pandemic groups
Outcomes
The primary outcome, the rate of successful reperfusion, was not significantly different in the pre-pandemic group versus the pandemic group (88.2% (n=30) vs 85.7% (n=18); OR 0.971, 95% CI 0.785 to 1.203; p=1.000) (table 2, figure 2).

{kind=link}
{kind=link}
(A) The mTICI grade distribution. No significant difference was revealed between the pre-pandemic and pandemic groups. (B) The time intervals from onset to successful reperfusion. Compared with the pre-pandemic group, the time from hospital arrival to puncture time (174 vs 125.5 min, p=0.002) and hospital arrival to reperfusion time (213 vs 172 min, p=0.047) in the pandemic group was prolonged significantly. HTP, hospital arrival to puncture; mTICI, modified Thrombolysis In Cerebral Infarction; OTH, onset to hospital arrival; PTR, puncture to reperfusion.
Procedural details and clinical outcomes of EVT for AIS patients in pre-pandemic and pandemic groups
Compared with the pre-pandemic group, hospital arrival to puncture time (174 vs 125.5 min, p=0.002) and hospital arrival to reperfusion time (213 vs 172 min, p=0.047) in the pandemic group was prolonged significantly. No difference in anesthesia approaches (67.6% vs 85.7%; OR 1.267, 95% CI 0.947 to 1.695; p=0.240), puncture to reperfusion time (32 vs 40.5 min, p=0.231), and the first-line choice of thrombectomy technique and rescue treatment after first-line strategy (29.4% vs 23.8%; OR 0.810, 95% CI 0.321 to 2.043; p=0.650) was revealed between the two groups. Early improvement in neurological outcomes was not significantly different between the two groups, with no obvious change in NIHSS score at 24 hours or 72 hours in both groups (table 2). The safety outcome was also not significantly different in the pre-pandemic group versus the pandemic group (35.3% (n=12) vs 28.6% (n=6); OR 0.810, 95% CI 0.68 to 2.10; p=0.606). One patient (2.9%) of the pre-pandemic group died due to ICH within 24 hours post-procedure (table 2).
Discussion
In this retrospective study during the COVID-19 pandemic, we evaluated the impact of the PCS algorithm (figure 1) on EVT for AIS patients by comparing its process and clinical outcomes between the pre-pandemic period and the pandemic period. The results showed: (1) hospital arrival to puncture time and hospital arrival to reperfusion time were significantly prolonged during the pandemic compared with the pre-pandemic period (table 2); (2) puncture to reperfusion time decreased by an average of 10 min but without statistical significance (table 2); (3) rate of successful reperfusion and other clinical outcomes were all comparable between the two groups (table 2 and figure 2).
The prolonged hospital arrival to puncture time (by 48.5 min, p=0.002) and hospital arrival to reperfusion time (by 41 min, p=0.047) mainly reflected the delay caused by the COVID-19 screening process. In accordance with guidelines of the National Health Commission, all hospitals need to conduct strict COVID-19 screening for all newly admitted patients, including emergency cases. The screening included taking a travel history, chest CT scanning, complete blood count test, body temperature measurement and the ensuing multidisciplinary consultation.5 Although this screening was started simultaneously with the screening for AIS, and patient transfer among different departments within the hospital was facilitated, it still delayed the subsequent treatment. Another reason was perhaps the launch of PCS. A middle-aged patient was diagnosed as a clinically suspected case of COVID-19 by the multidisciplinary consultation based on fever, abnormal lymphocyte count and signs of inflammation in the chest CT; thus PCS was triggered and EVT was performed under the highest level of protection. Postoperative mTICI 2b recanalization was achieved. Hospital arrival to puncture time was 287 min, 46 min longer than the average hospital arrival to reperfusion time (241 min). On the other hand, our results showed the lengthy increases of hospital arrival to puncture time and hospital arrival to reperfusion time did not impact the short-term outcomes. The currently available data in this study were not enough to explain the above situation. Although there was no significant difference in relation to short-term outcomes, we did not have the long-term follow-ups (eg, 90 day mRS scores) to evaluate the long-term efficacy. Whether the delayed time window for treatment had an impact on the long-term outcomes is thus still unclear. Both situations need further studies.
Puncture to reperfusion time was shown to have a tendency to decrease (from 40.5 min to 32 min) without evidence of any influence on patient safety and successful recanalization rates during the pandemic. A series of attempts were adopted to minimize the time of the EVT procedure, including performing the entire procedure by an experienced neurointerventional specialist and reducing angiography processes based on good CT angiography images. Other reasons may be more frequent use of local anesthesia and first-line ADAPT strategy (42.9% vs 29.4%; OR 1.457, 95% CI 0.711 to 2.987; p=0.308).
Although hospital arrival to puncture time and hospital arrival to reperfusion time have been prolonged during the pandemic, all clinical outcomes including rate of successful reperfusion and procedure-related serious adverse events have remained unchanged during the pandemic. Expert consensus from the Chinese Federation of Interventional and Therapeutic Neuroradiology recommended that all patients, including those receiving emergency cerebrovascular interventional therapy, should undergo preoperative chest CT scanning and multidisciplinary consultations to exclude COVID-19, and the PCS algorithm was established to deal with confirmed or suspected COVID-19 patients.7 The results of the present study show that this recommendation could potentially reduce the spread of SARS-CoV-2 without threatening patient safety and clinical outcomes.
One of the major limitations of this study is the retrospective, observational design which is prone to inherited selection bias. In addition, the sample size of this single center study was relatively small. Third, the limited follow-up due to the influence of the pandemic does not allow the evaluation of long-term efficacy (eg, 90 day mRS scores). Future prospective multicenter studies with large sample sizes are needed to confirm the above results.
In conclusion, the PCS algorithm which combines COVID-19 screening and protection measures could decrease the impact of the disease on the clinical outcome of EVT for AIS patients to the lowest extent possible during the pandemic. This needs to be confirmed by future well-designed studies.
Acknowledgments
The authors thank Mr Kun Yang (Department of Evidence-Based Medicine, Xuanwu Hospital, Capital Medical University, Beijing, China) for helping us with statistical analysis.
Footnotes
BY and TW contributed equally.
Contributors All authors of this work met the International Committee of Medical Journal Editors criteria for authorship and made substantial contributions to the conception and design, acquisition of data, analysis and interpretation of data, drafting, critical revising, and final approval of this manuscript.
Funding This work was supported by the National Key Research and Development Project (2016YFC1301703) and the Beijing Scientific and Technologic Project (D161100003816002).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Approved by the Ethics Committee of Xuanwu Hospital ([2020]005).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The data used to support the findings of this study are available from the corresponding author upon request.