Article Text

Abstract
Background Benefit of thrombectomy in patients with a low initial Alberta Stroke Program Early CT Score (ASPECTS) is still uncertain. We hypothesized that, despite low ASPECTS, patients may benefit from endovascular recanalization if good collaterals are present.
Methods Ischemic stroke patients with large vessel occlusion in the anterior circulation and an ASPECTS of ≤5 were analyzed. Collateral status (CS) was assessed using a 5-point-scoring system in CT angiography with poor CS defined as CS=0–1. Clinical outcome was determined using the modified Rankin Scale (mRS) score after 90 days. Edema formation was measured in admission and follow-up CT by net water uptake.
Results 27/100 (27%) patients exhibited a CS of 2–4. 50 patients underwent successful vessel recanalization and 50 patients had a persistent vessel occlusion. In multivariable logistic regression analysis, collateral status (OR 3.0; p=0.003) and vessel recanalization (OR 12.2; p=0.009) significantly increased the likelihood of a good outcome (mRS 0–3). A 1-point increase in CS was associated with 1.9% (95% CI 0.2% to 3.7%) lowered lesion water uptake in follow-up CT .
Conclusion Endovascular recanalization in patients with ASPECTS of ≤5 but good collaterals was linked to improved clinical outcome and attenuated edema formation. Collateral status may serve as selection criterion for thrombectomy in low ASPECTS patients.
- stroke
- brain ischemia
- thrombectomy
- edema
- outcome
- computed tomography
Statistics from Altmetric.com
Introduction
Ischemic stroke patients with acute large vessel occlusions of the anterior circulation benefit from endovascular recanalization.1 This benefit applies to inclusion criteria of clinical trials including patients with Alberta Stroke Program Early CT Score (ASPECTS) of >5. Only limited data exist that indicate the effect of mechanical thrombectomy (MT) in patients with lower ASPECTS.1–6 Potential clinical benefit or harm from MT in patients with low initial ASPECTS remains under debate.4 7–9 The recent sub-analysis of the HERMES (Highly Effective Reperfusion Using Multiple Endovascular Devices) meta-analysis offered promising results, concluding that patients with an ASPECTS of 3–5 may benefit from MT.4
Prior research indicated that good collaterals may trump poor ASPECTS when considering patients with low ASPECTS for intravenous lysis.10 Moreover, poor collaterals have been demonstrated to be strong predictors of an unfavorable response to MT and functional outcome.11–13 Therefore, in the prospective multicenter ESCAPE (Endovascular Treatment for Small Core and Proximal Occlusion Ischemic Stroke) trial, patients with poor collaterals were excluded from MT.14 The impact of collateral status on clinical outcome in low ASPECTS patients after endovascular recanalization, however, is as yet uncertain and a matter of current debate.15 Good collaterals are known to be less frequent in low ASPECTS patients, but still occur in up to 30% in this patient group, and there may be a potential favorable effect so that collateral status could serve as selection criterion for treatment of this subgroup.10
Ischemic cerebral edema—that is, the degree of lesion water uptake—has been described as a possible mechanism for early collateral failure after onset of a large vessel occlusion. Progression of early edema eventually leads to adjacent mass effect and elevated interstitial pressure which increases the resistance of collateral arterioles and downstream perforating arterioles.16 Therefore, patients affected by low levels of water uptake despite large early ischemic lesion extent may sustain good collateral circulation, and these patients may also benefit from MT.16 We hypothesized that in patients with a large early infarct (ie, low initial ASPECTS), proficient collateral circulation and low ischemic tissue water uptake are closely interrelated and indicate a benefit of vessel recanalization.
Methods
Patients
All ischemic stroke patients admitted between October 2015 and December 2018 at the local university hospital, a high-volume tertiary stroke center, were retrospectively analyzed. The study protocol was approved by the local ethics committee (Ethikkommission der Ärztekammer Hamburg, WF04-13) and was in accordance with the Declaration of Helsinki. The institutional review board waived informed consent after review. Ischemic stroke patients with large vessel occlusion in the anterior circulation and an ASPECTS of ≤5 were screened based a priori defined inclusion criteria: (1) ischemic stroke with acute occlusion of the M1 segment of the middle cerebral artery (MCA) or distal occlusion of the internal carotid artery (ICA); (2) multimodal CT protocol at admission including CT angiography (CTA) and CT perfusion (CTP) performed within 12 hours from known symptom onset; (3) an initial ASPECTS ≤5 in admission CT; (4) follow-up CT (FCT) after 24 hours; (5) admission National Institutes of Health Stroke Scale (NIHSS) score >3; (6) absence of intracranial hemorrhage and pre-existing thromboembolic or hemodynamic infarctions in admission non-enhanced CT (NECT) or pre-existing significant carotid stenosis. Baseline clinical characteristics were retrieved from the medical records, including the modified Rankin Scale (mRS), after 90 days.
Clinical outcome was dichotomized. Good clinical outcome was defined as mRS 0–3 instead of 0–2 to avoid data imbalance, since a comparably worse outcome in low ASPECTS patients is expected.1 ASPECTS were rated by an experienced neuroradiologist and verified by an attending neuroradiologist. Discrepancies were corrected in consensus reading, if necessary. Patients were dichotomized by status of vessel recanalization: (a) successful vessel recanalization after MT (Thrombolysis In Cerebral Infarction scale (TICI) 2b or 3); (b) persistent large vessel occlusion (LVO) in patients with failed recanalization after mechanical thrombectomy (TICI 0-2a) or patients who did not receive endovascular treatment. In patients who did not undergo MT, the persistence of LVO was confirmed via a dense artery sign in FCT and/or transcranial color-coded duplex ultrasonography.17 Individual reasons to perform MT in patients with low initial ASPECTS included an early time frame from symptom onset despite existence of already recognizable signs of large ischemia, significant mismatch in CTP with tissue-at-risk in eloquent regions beyond areas contributing to the low ASPECTS, or younger patient age. Image acquisition protocols can be found in the online supplemental material.
Supplemental material
Imaging protocol
Image analysis
(Online supplementary material)The de-identified CT images were processed at an external core lab and segmented manually using commercially available software (Analyze 11.0, Biomedical Imaging Resource, Mayo Clinic, Rochester, MN). Collaterals were categorized applying an established 5-point scoring system.18 Intracranial CTA maximum intensity projections (MIPs) were used for grading the abundance of visible arterial vasculature distal to the occluded vessel in comparison to the contralateral hemisphere: 0=absent collaterals in >50% of the MCA territory; 1=diminished collaterals in >50% of the MCA territory; 2=diminished collaterals in <50% of an MCA-M2 branch territory; 3=collaterals equal to the contralateral hemisphere; and 4=increased collaterals.18 Figure 1 shows an example of two low ASPECTS patients with good versus poor collaterals. We determined net water uptake (NWU) within early infarct as the imaging biomarker to quantify cerebral ischemic edema in the admission CT before treatment and in FCT after treatment with a standardized procedure, as reported elsewhere.19–22

Examples of low ASPECTS patients with good versus poor collaterals. Initial non-enhanced CT, CT angiography maximum intensity projections, and follow-up CT in patients with low ASPECTS and poor (upper example) versus good collaterals (lower example). ASPECTS, Alberta Stroke Program Early CT Score; CTA, CT angiography; MIP, maximum intensity projection; NECT, non-enhanced CT.
Statistical analysis
Kolmogorov-Smirnov tests were used to determine whether the datasets were well-modeled by a normal distribution. Continuous variables were presented as mean (95% CI) or mean (SD). Alternatively, median and IQR were used (non-normal distribution). Student t-tests (normal distribution) with 95% CI or SD, or Mann-Whitney U tests (non-normal distribution) with IQR, were used to describe differences in the acquired parameters (table 1). Univariate and multivariate logistic regression analyses were performed to predict good functional outcome using backwards selection (mRS 0–3 after 90 days). As independent parameters we analyzed age, sex, collateral score, NIHSS, NWU in admission CT and FCT, recanalization status, ASPECTS, blood glucose at admission, and application of intravenous lysis. Good collaterals were defined as collateral score 2–4, and poor collaterals as 0–1. An interaction term ‘successful vessel recanalization * good collateral status’ was added to the model to differentiate the effect of recanalization in low ASPECTS patients dependent on collateral status.
Patient characteristics
Furthermore, patients with successful vessel recanalization were analyzed separately using Student t-tests (normal distribution) or Mann-Whitney U tests (non-normal distribution), and multivariate logistic regression analysis as well as multivariate linear regression were performed to assess the impact of collateral status on edema formation and clinical outcome in this group of patients (online supplementary figure I–II).
Supplemental material
Supplemental material
A sub-analysis was performed using volumetrically derived ischemic core volumes from cerebral blood volume maps, as reported elsewhere.19 22 Ischemic core volume was analyzed in a multivariable logistic regression model including collateral scores, recanalization status, and age. Moreover, patients with very high ischemic core volumes >50 mL and >70 mL were analyzed separately using multivariable logistic regression models, to evaluate whether recanalization status and collateral scores were significantly and independently associated with clinical outcome.
A statistically significant difference was accepted at a value of p<0.05. Analyses were performed using MedCalc (version 11.5.1.0; Mariakerke, Belgium) and R (R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing. Vienna, Austria, 2017).
Results
One hundred patients fulfilled the inclusion criteria and were analyzed. Patient characteristics are listed in table 1. In total, 10 patients of the study cohort died before follow-up imaging could be performed. In 74 patients, endovascular recanalization was attempted (74%) and succeeded in 50 patients (68%) with TICI 2b/3. The mean (SD) age was 71 (13) and 35 patients (35%) were women. The mean (SD) NIHSS was 17.8 (4.5) and patients received admission imaging after a mean (SD) of 3.8 (1.8) hours after symptom onset. The median ASPECTS was 4 (IQR 4–5) and the median collateral score was 1 (IQR 0–2). Twenty-seven patients had good collaterals with a score of 2–4 (27%) and 71 patients had poor collaterals with a score of 0–1 (71%) (CS0=33 patients, CS1=38 patients, CS2=14 patients, CS3=10 patients, CS4=3 patients). At admission imaging, there were no significant differences in collateral score (1.1 vs 0.9) or edema formation (NWU 9.6% vs 11%) between patients with and without vessel recanalization.
Comparing patients with good clinical outcome (mRS 0–3) to patients with poor clinical outcome we observed significant differences in the median initial collateral score, which was 2 (IQR 0–3) in patients with good outcome and 1 (IQR 0–1) in patients with poor outcome (p=0.02). Moreover, patients with good outcome were significantly younger (63 years vs 74 years; p=0.003) and had a lower initial NIHSS (15 vs 19, p=0.001). Admission NWU was by trend lower in patients with good outcome (7.8% vs 10.0%; p=0.1). There were no significant differences in time from onset to imaging or ASPECTS. In the FCT after treatment, the mean (SD) NWU was significantly higher in patients with poor outcome (23.4% vs 17.5%; p=0.009) and infarct volume was higher (147.5 mL vs 79.5 mL; p=0.009). Functional outcome according to recanalization status and collateral score is displayed in figure 2.
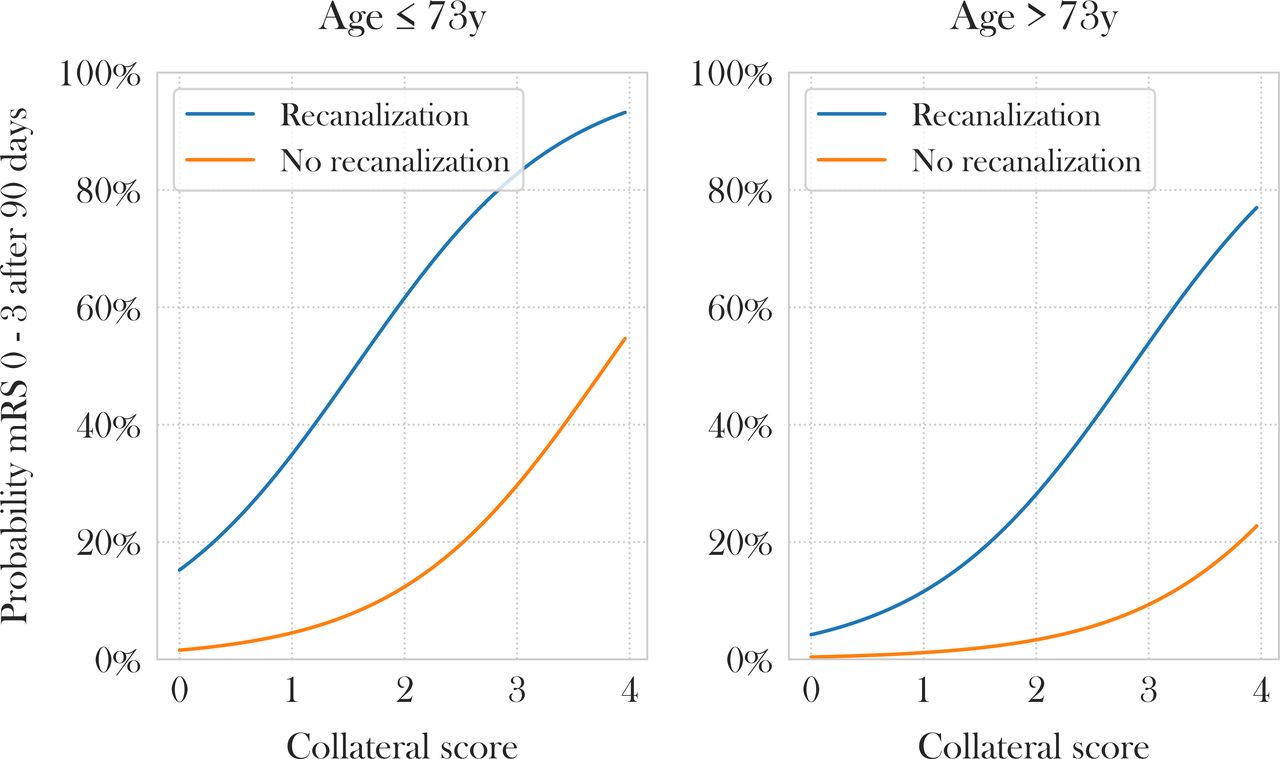
Impact of collateral scores and age on functional outcome. Multivariable logistic regression analysis displaying the impact of collateral scores (x-axis) on functional outcome (y-axis) separated by median age (73 years) and recanalization status. mRS, modified Rankin Scale.
The expected model based probabilities for good clinical outcome depending on recanalization status and collateral scores were: no recanalization/poor collaterals: 1.9%; no recanalization/good collaterals: 14.0%; successful recanalization/poor collaterals: 19.6%; successful recanalization/good collaterals: 67.1%. The interaction term ‘successful vessel recanalization * good collateral status’ was not a significant predictor of clinical outcome (OR 2.01, 95% CI 0.06 to 68.65; p=0.669).
In univariable logistic regression analysis, age, admission NIHSS and collateral score were significantly associated with good functional outcome (mRS 0–3) (online supplementary table I). NWU in FCT was by trend associated with good functional outcome. A 1-point increase in collateral score increased the likelihood for good outcome by 2.68 (OR, 95% CI 1.60 to 4.49; p<0.001). In multivariate logistic regression analysis, the independent parameters that remained in the model were age, collateral score, and recanalization status (online supplementary figure I). The OR for good outcome in this cohort was 12.2 (95% CI 1.85 to 80.18) for successful vessel recanalization, 3.01 (95% CI 1.46 to 6.16) for collateral score, and 0.93 (95% CI 0.88 to 0.98) for age (per 1 year increase).
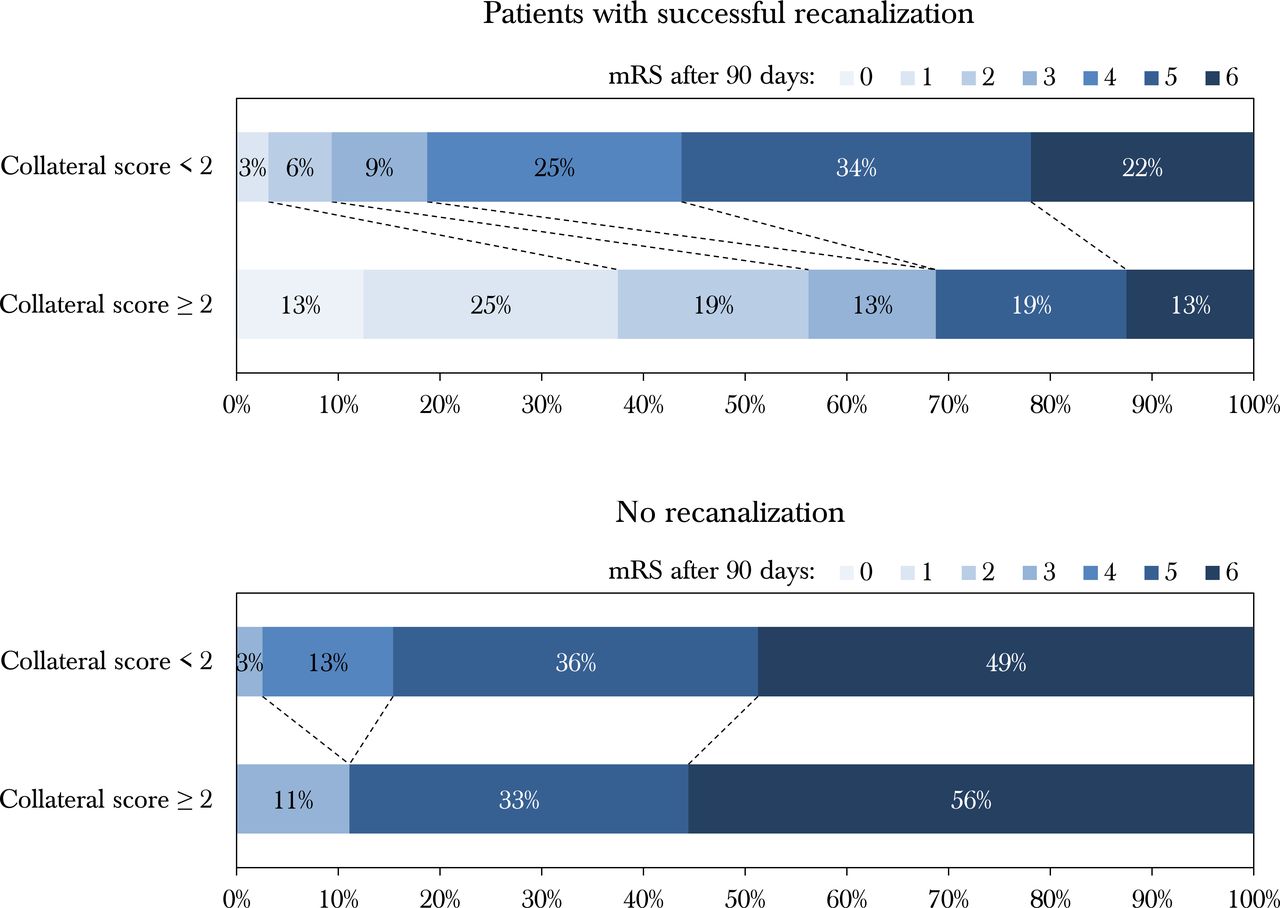
Subsequently, only patients with successful MT were analyzed. Comparing patients with collateral score 0–1 (53%) versus 2–4 (47%), the median mRS was significantly lower in patients with better collaterals (2 vs 5; p<0.001). Moreover, the mean NWU was significantly lower in patients with better collaterals (15.7% vs 19.6%; p=0.049). In multivariate logistic regression analysis for patients with successful MT, lower patient age (OR 0.93, 95% CI 0.88 to 0.98; p=0.009) and higher collateral score (OR 2.61, 95% CI 1.32 to 5.18; p=0.006) were significantly associated with good clinical outcome, adjusted for ASPECTS and NIHSS. Figure 3 shows bar graph diagrams with functional outcome after 90 days according to collateral score and recanalization status.

{kind=link}
{kind=link}
{kind=link}
Modified Rankin scale (mRS) scores at 90 days in the study cohort bar graph illustrating functional outcome for patients with vessel recanalization (upper bars) and persistent vessel occlusion (lower bars), according to their collateral status.
Finally, we performed a linear regression analysis to show the impact of collaterals on edema formation (NWU). A 1-point increase in collateral score was significantly associated with reduced NWU in the FCT of 1.9% (95% CI 0.2% to 3.8%; p=0.03) (online supplementary figure IV).
Supplemental material
Sub-analysis ischemic core volume
In multivariable logistic regression analysis ischemic core volume was not a significant independent predictor. Second, we analyzed the impact of collateral scores and recanalization specifically in patients with higher core volumes (>50 mL and >70 mL) (online supplementary material).
In patients with an ischemic core volume >50 mL, both recanalization status and collateral scores were significantly and independently associated with clinical outcome (recanalization: OR 17.5, 95% CI 1.39 to 219.6; p=0.03; collateral scores: OR 5.1, 95% CI 1.1 to 25.2; p=0.04).
In patients with a core volume >70 mL, collateral score was significantly associated with clinical outcome (OR 6.23, 95% CI 1.11 to 34.89; p=0.04). Recanalization status, however, failed to be significantly associated with clinical outcome.
Discussion
To our knowledge, this is the first study to investigate the impact of collateral status on edematous lesion pathophysiology and functional outcome in patients with ischemic stroke who presented with an initial ASPECTS of ≤5 due to large vessel occlusion in the anterior circulation. The main finding of this study was that despite large early infarct lesions, vessel recanalization with good collateral status and younger patient age were independent predictors of improved functional outcome. In patients with successful vessel recanalization, collateral status was the only independent parameter of good functional outcome. Correspondingly, a favorable effect with regards to formation of ischemic brain edema was observed suggesting that proficient collateral circulation may decelerate lesion water uptake.
Good collaterals increased the probability for good outcome by 12.1% in patients without vessel recanalization (1.9% vs 14%) and by 47.5% in patients with successful vessel recanalization (19.6% vs 67.1%). The interaction term ‘successful vessel recanalization * good collateral status’ was no significant predictor of good outcome. Therefore, vessel recanalization improved outcome across all collateral scores in patients with a low ASPECTS, based on our data.
Currently, there is an increasing trend to select low ASPECTS patients for endovascular treatment. A recent subgroup analysis of the HERMES meta-analysis suggested that patients with an ASPECTS of 3–5 may benefit from endovascular treatment (OR 2.0, 95% CI 1.16 to 2.45) assessed by mRS score at 90 days.4 Nevertheless, clinical outcome ranged significantly, emphasizing the need for treatment selection.
Our findings confirm the importance of collaterals on clinical outcome in patients following endovascular treatment, although patients with lower ASPECTS regularly have worse collaterals.13 Nevertheless, it has also been described that up to 32% of low ASPECTS patients may have good collaterals.10 In our patient cohort, patients with low ASPECTS, successful recanalization and poor collaterals had a median mRS score of 5, while patients with low ASPECTS, successful recanalization but good collaterals showed improved outcome with a median mRS score of 2. Prior research indicated that patients with large early infarcts but good collaterals should receive intravenous lysis and it was concluded that good collaterals may trump low ASPECTS.10 We conducted a sub-analysis separately for patients with a large ischemic core (ie, >50 mL and >70 mL). Both collateral and recanalization status remained significant and independent predictors of clinical outcome (>50 mL). For patients with an ischemic core >70 mL, collaterals remained a significant independent parameter while recanalization status failed to reach statistical significance. The main reason may be the low number of patients for this sub-analysis cohort.
Degree of collateral supply in CTA may be regarded as the visible abundance of arterial vasculature within the ischemic hemisphere distal to the clot in comparison to the contralateral hemisphere. Usually, collateral vasculature is not seen within the early infarct lesion; however, perilesional collateral supply may contribute to beneficial tissue outcome in two ways. First, it may stop penumbral loss and further infarct growth, which may be significant even in low ASPECTS patients.18 Second, it may prevent malignant edema by counteracting the disbalance of water homeostasis with lower levels of lesion water uptake, as suggested by our data.22
Collateral vasculature within tissue affected by early infarct is not seen regularly in CTA; however, it may occur with the phenomenon of clot migration or spontaneous recanalization of branches. Any visible collateral vasculature within early infarct cannot contribute to tissue salvage obviously; however, the effect on edema progression may be significant by reducing water uptake.5 15
Prior observations indicated that poor intracranial collaterals are associated with elevated edema formation at the time of follow-up imaging after endovascular treatment.23 Poor collaterals may lead to increased formation of edema, but vice versa, ischemic edema may also cause elevated interstitial pressure, which increases the resistance of downstreams perforating arterioles and may therefore lead to early collateral failure.15 16
Along with the results of the present study, a specific interaction between collateral status, formation of edema and clinical outcome thus becomes apparent. It is conceivable that only patients with lower lesion water uptake profit from thrombectomy, otherwise the edematous mass effect may lead to detrimental compression of perilesional collateral vasculature.24 Lower levels of NWU within early infarct is likely to be a factor of sustained collateral circulation, which reciprocally stabilizes edema progression and surrounding penumbra over time. Other factors may tie into this process, such as aquaporin-4 polymorphisms.25
The ASPECTS rating itself is based on detecting visually evident hypoattenuation, although the degree of hypoattenuation is not encoded. Any hypoattenuated ischemic lesion is physically equivalent to early infarct with vasogenic edema which can be quantified by NWU.20 26 Thus, two patients may show the same ASPECTS with comparable lesion extent but a significantly different degree of hypoattenuation—that is, different lesion water uptake. In this cohort of low ASPECTS patients, water uptake in the admission CT ranged from <1% to 21.8% and was significantly correlated with the status of the collateral circulation. Accordingly, low uptake of water in low ASPECTS patients was associated with comparably better collaterals, which may result in both improved response to endovascular treatment and better functional outcome, as suggested by the results of this study.11 13
While quantification of ischemic edema in multimodal CT in the setting of acute patient triage is technically not yet feasible and time-consuming, collateral scoring is fast and straight forward; it could therefore serve as selection criterion for different treatment options in low ASPECTS patients such as endovascular treatment with or without adjuvant anti-edematous medication to limit malignant edema.22 27 28 Our findings affirm the lately observed effect of vessel recanalization on lesion pathophysiology with reduced edema progression, which was directly associated with the observed effect on clinical endpoints.29–31 Furthermore, quantification of NWU in these patients may introduce new opportunities to specifically monitor treatment effects of potential adjuvant drugs targeting the formation of ischemic brain edema, such as glyburide.27 32
Limitations of our study include the small number of patients, due to strict inclusion and exclusion criteria. Second, a limited number of screened patients with a large early infarct received endovascular recanalization. Furthermore, patient selection for mechanical thrombectomy was not randomized which might cause a potential selection bias in this retrospective study. Recanalization status in patients who received alteplase but no endovascular procedure (n=12) was only deducted using follow-up NECT and sonography, which is not equivalent to recanalization status derived from angiographic images. However, the number of patients with false recanalization status is expected to be very low (approximately 1–2 patients) based on prior reference on vessel recanalization after alteplase alone in large vessel occlusions.33 Another important limitation is the already lower collateral status in patients with low ASPECTS and therefore a limited number of patients with good collaterals. Future studies involving more patients are needed to validate our observations, and prospective studies should be undertaken to identify optimal selection criterion for low ASPECTS patients.
Conclusions
Collateral status may be relevant to clinical outcome in acute ischemic stroke patients despite an initial low ASPECTS of ≤5. Poor intracranial collaterals were directly associated with aggravated edema formation and impaired clinical outcome, while better collaterals attenuated ischemic brain edema with improved outcome. Based on the results of this study, collateral status could serve as selection criterion for treatment of low ASPECTS patients.
Supplemental material
References
Footnotes
Contributors GB: Study design. Acquisition of data. Image processing. Data analysis. Statistical analysis. Drafting the manuscript and revising it critically. HK: Data analysis. Acquisition of data. Drafting the manuscript and revising it critically. PS: Data analysis. Statistical analysis. Acquisition of data. Drafting the manuscript and revising it critically. UH: Data analysis. Statistical analysis. Acquisition of data. Drafting the manuscript and revising it critically. FF: Data analysis. Acquisition of data. Drafting the manuscript and revising it critically. MS: Data analysis. Drafting the manuscript and revising it critically. LM: Data analysis. Statistical analysis. Drafting the manuscript and revising it critically. GS: Data analysis. Statistical analysis. Drafting the manuscript and revising it critically. BM: Study design. Drafting the manuscript and revising it critically. GR: Study design. Drafting the manuscript and revising it critically. JF: Study design. Drafting the manuscript and revising it critically. AK: Study design. Acquisition of data. Image processing. Data analysis. Statistical analysis. Drafting the manuscript and revising it critically.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests JF: Consultant for Acandis, Boehringer Ingelheim, Codman, Microvention, Sequent, Stryker. Speaker for Bayer Healthcare, Bracco, Covidien/ev3, Penumbra, Philips, Siemens. Grants from Bundesministeriums für Wirtschaft und Energie (BMWi), Bundesministerium für Bildung und Forschung (BMBF), Deutsche Forschungsgemeinschaft (DFG), European Union (EU), Covidien, Stryker (THRILL study), Microvention (ERASER study), Philips. AK: research collaboration agreement: Siemens Healthcare. All other authors: No conflicts.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.