Article Text

Abstract
Background Arteriovenous malformations (AVMs) are vascular lesions that may be treated by an endovascular approach using liquid embolic agents but the control of the liquid embolic agent remains poor and a potential complication may be distal migration of embolic material. The TIGERTRIEVER 13 is a new stent retriever designed for stroke thrombectomy and has a version ideal for distal occlusions. We report our experience in the removal of embolic agent which had migrated into the distal vessels using the TIGERTRIEVER during PHIL/Onyx embolization of AVMs.
Clinical presentations Three patients with brain and spinal AVMs underwent endovascular embolization. During trans-arterial embolization of the AVM with PHIL/Onyx, retrograde filling of distal arterial feeders was followed by migration into the normal arterial branches (cortical middle cerebral artery, distal posterior cerebral artery, and anterior spinal artery). This resulted in occlusion or sluggish distal flow in these branches with potential significant neurological deficits. In all three cases, a Headway Duo microcatheter was navigated distally in the occluded vessel beyond the embolic material using a Traxcess microwire. The TIGERTRIEVER 13 was deployed with recanalization of the vessel after a single attempt. In all three patients there were no complications related to the retrieval of embolic agent.
Conclusion Distal migrated embolic agents such as PHIL or Onyx can be removed from various arterial vascular territories using stent retrievers dedicated to small vessels.
- arteriovenous malformation
- technique
- thrombectomy
- intervention
- liquid embolic material
Statistics from Altmetric.com
Introduction
Brain and spinal arteriovenous malformations (AVMs) may be treated with a variety of different modalities, including microsurgical resection, endovascular embolization, radiosurgery, and a combination of these techniques (table 1). The most used embolic agents are EVOH (Onyx; eV3 Neurovascular, Irvine, California, USA), Squid (Balt, Montmorency, France), and PHIL (Microvention Inc, California, USA). Despite the advances in technology, ischemic complications in brain AVM embolizations are still reported to occur, with an incidence ranging from 2.6% to 5.4% of all procedures.1–4 One cause of ischemia is reflux in normal arteries with potential fragmentation and further migration of the embolic material, leading to an infarct. Liquid embolics may migrate via arterio-arterial anastomoses or can reflux alongside the microcatheter, which is the justification for using either the pressure cooker technique5 or a double lumen balloon microcatheter6 when injecting liquid embolic agents. Nonetheless, if the migrated embolic agent occludes an artery in an eloquent area, significant functional impairment may occur. The embolic agent also blocks off the vessel, resulting in an inability to re-access the vessel for further embolization attempts.
Summary of clinical characteristics
There are only a few case reports describing removal of refluxed Onyx from large vessels, such as the M1 segment of the middle cerebral artery (MCA) and the basilar artery,7–11 using standard thrombectomy tools. The TIGERTRIEVER 13 (Rapid Medical, Yoqneam, Israel) is a new stent retriever with a specific design developed for mechanical thrombectomy in small vessels. We describe the use of the TIGERTRIEVER 13 for the retrieval of embolic material which had migrated into distal vessels.
The device
TIGERTRIEVER 13 is a stent retriever with a degree of expansion and is controlled by a core wire using a dedicated handle (figure 1). By sliding the handle, the mesh of the TIGERTRIEVER 13 can be expanded or contracted, allowing a degree of expansion to adapt to the diameter of the vessel in which it has been placed. It is available in different diameters, ranging from 0.5 mm to 6 mm. The smallest size can be navigated through a microcatheter with an internal diameter of 0.013 inches.

The TIGERTRIEVER 13 revascularization device with integrated slider.
Clinical presentation
Case No 1
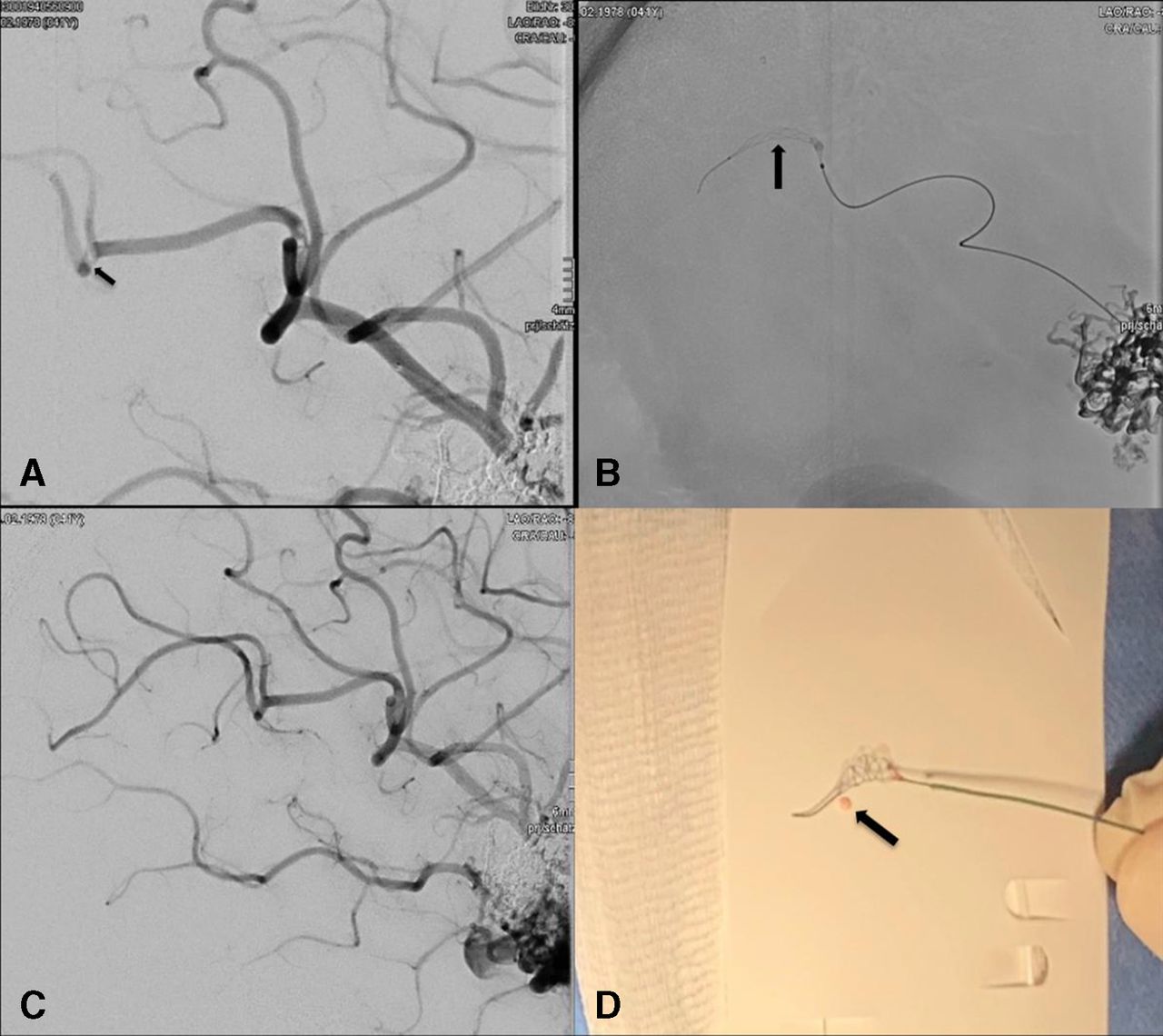
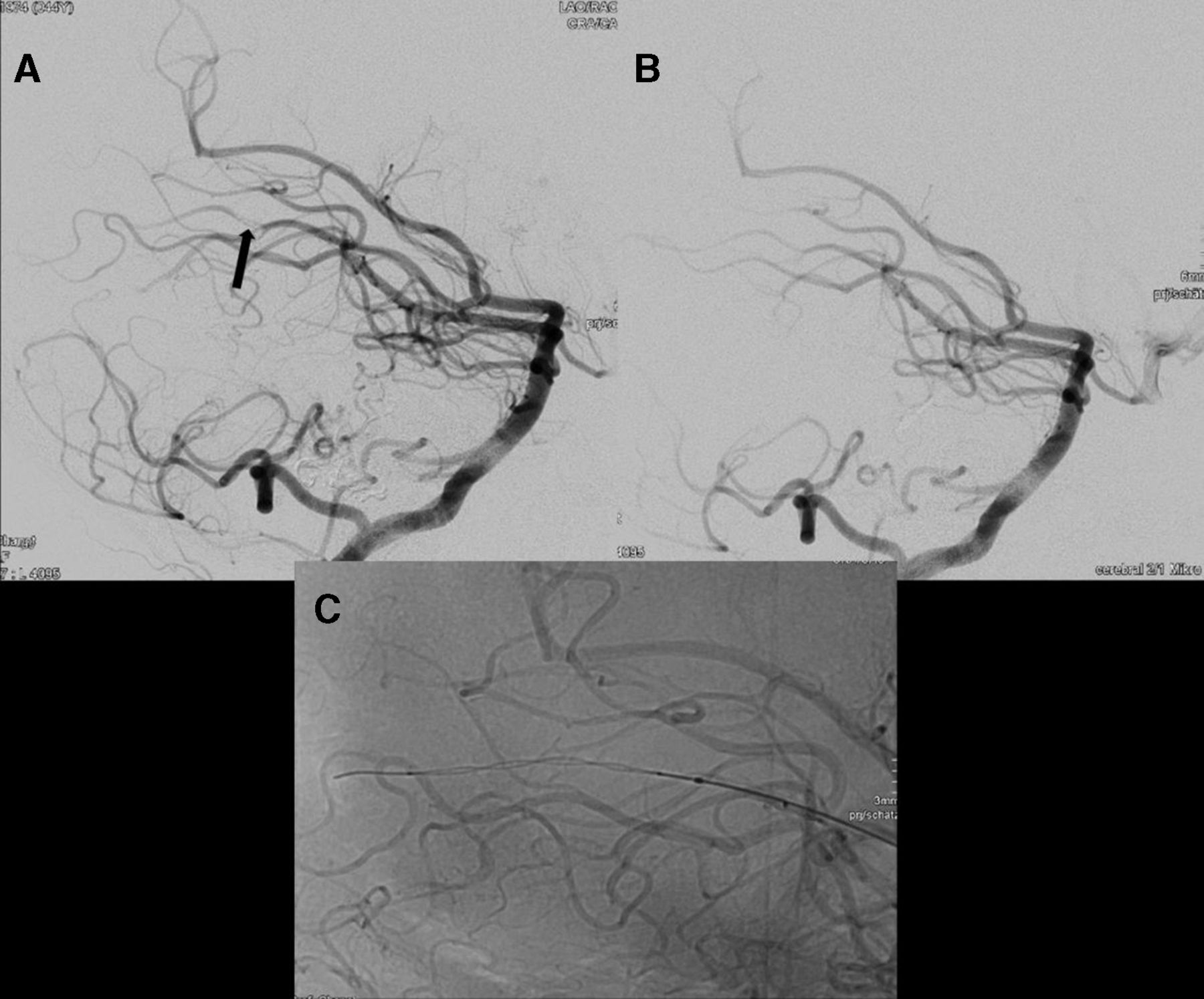
Second staged transarterial embolization of a ruptured insular AVM using low viscosity PHIL via the left MCA branches with a Sonic 1.2 F microcatheter was performed with the pressure cooker technique (table 1). During the course of embolization, embolic material refluxed through the transmedullary arteries to the M2 segment of the MCA and migrated further distally. A Headway Duo microcatheter was navigated into an MCA cortical branch beyond the embolic agent. The TIGERTRIEVER 13 removed the embolic material after one pass (figure 2). The segment was patent during transvenous embolization 6 weeks later with complete obliteration of the AVM.
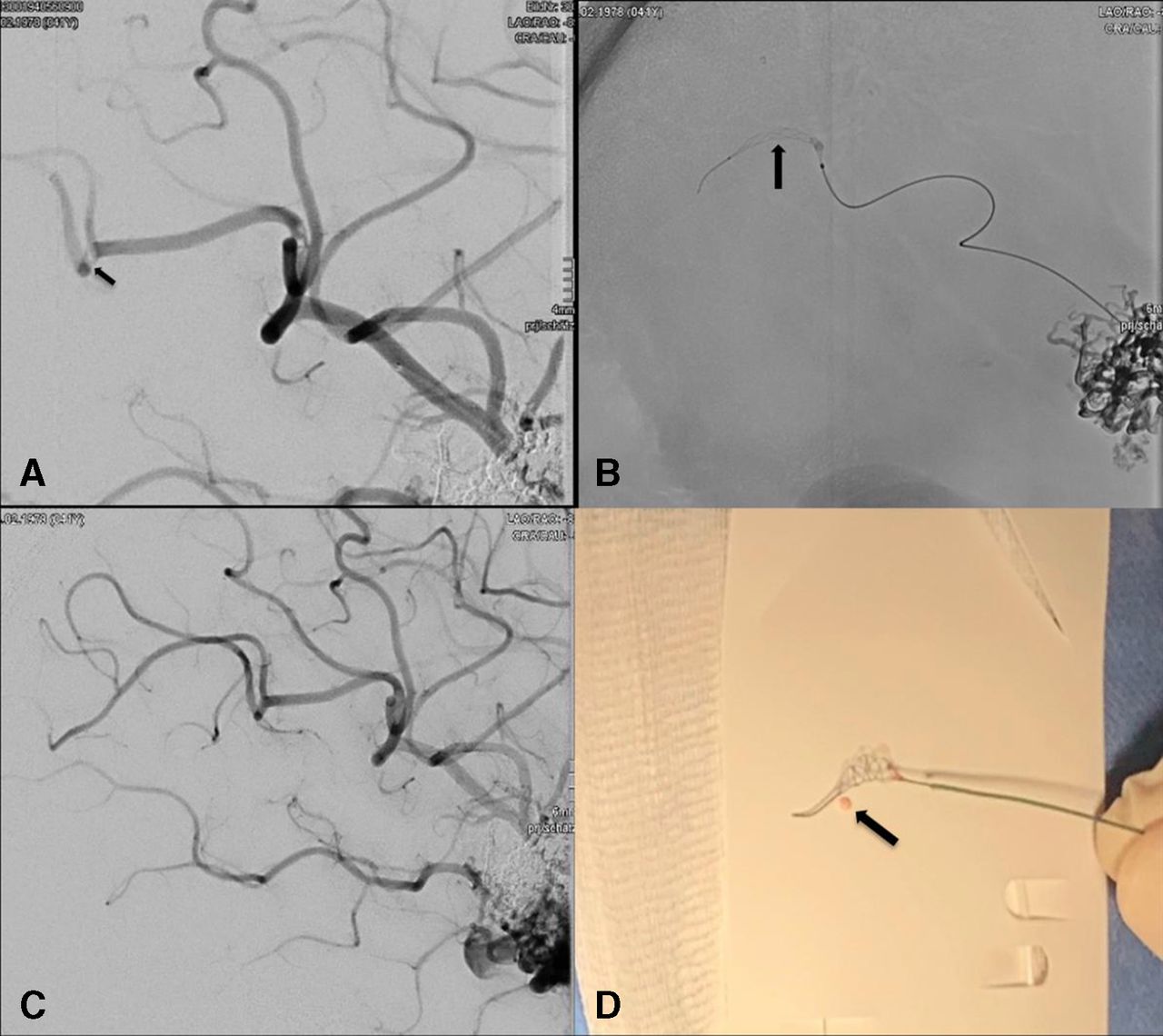
(A) The refluxed PHIL causing a filling defect in the distal M4 of the left middle cerebral artery (arrow). (B) A TIGERTRIEVER 13 (arrow) was deployed into the distal M4 segment for removal of PHIL. (C) Post removal DSA showed no further filling defect and good reperfusion. (D) The removed PHIL piece (arrow) and the TIGERTRIEVER 13 stent on gauze.
Case No 2
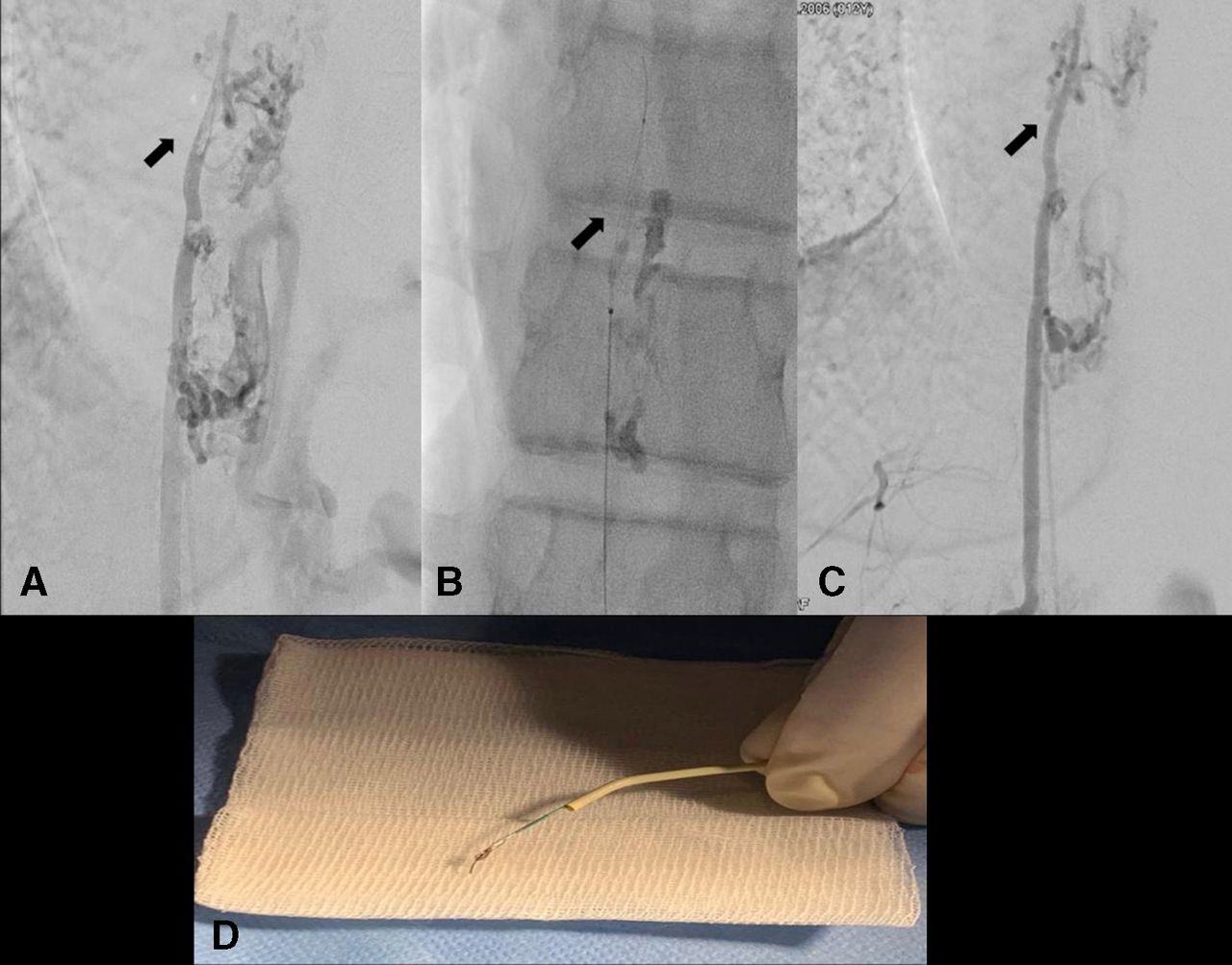
Elective transarterial embolization of a ruptured thoracic spinal AVM was performed with low viscosity PHIL embolic material injected through an Apollo microcatheter under protection of the anterior spinal artery with a Scepter XC balloon. The use of a balloon did not prevent two fragments of PHIL refluxing into the anterior spinal artery. Progressive flow reduction in the anterior spinal artery was noted. Embolized PHIL material was retrieved by the TIGERTRIEVER 13, allowing normal flow to be restored (figure 3). The patient was clinically unchanged with normal motor and sensory function on awakening.
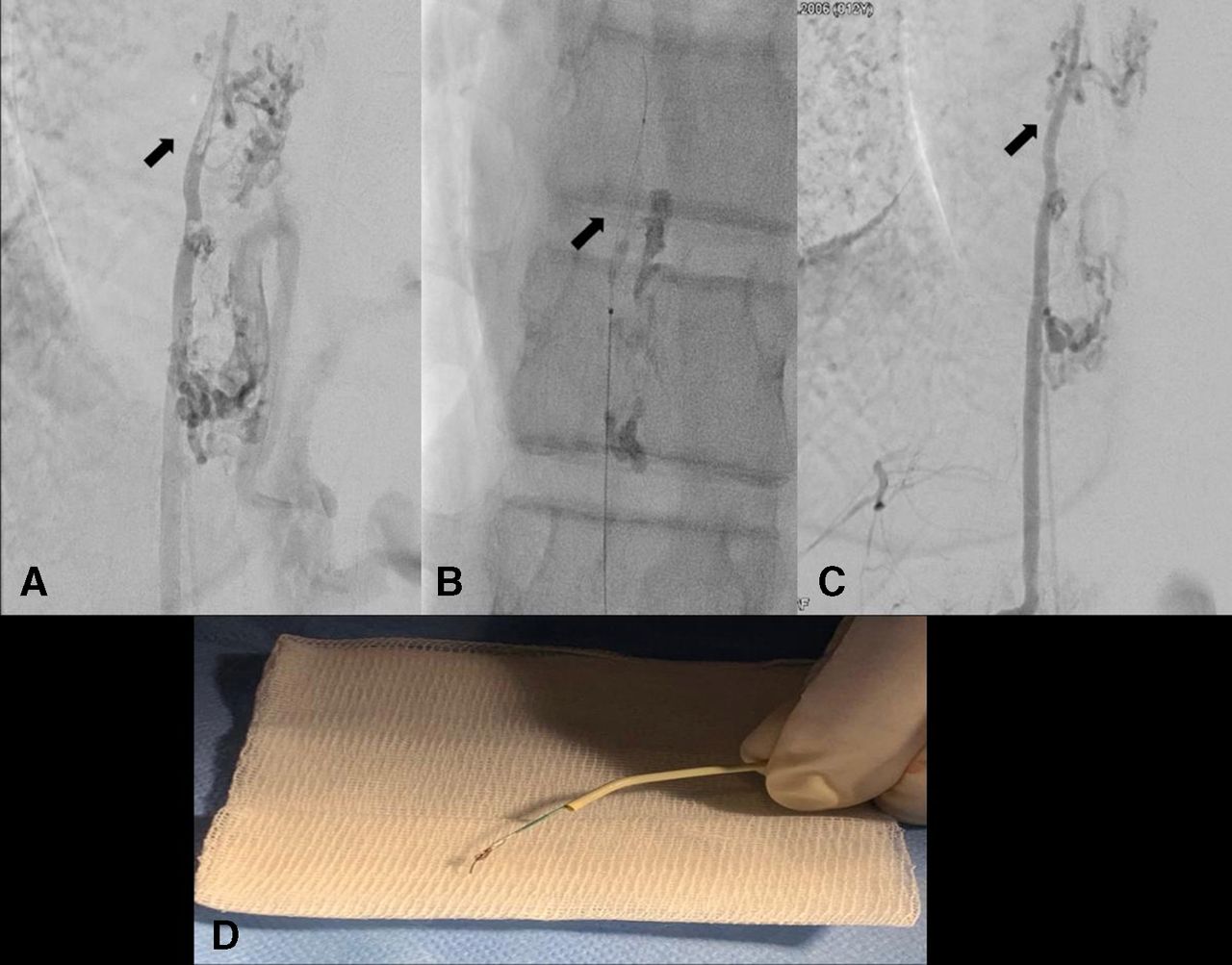
(A) The refluxed PHIL causing a filling defect in the thoracic anterior spinal artery (arrows). (B) A TIGERTRIEVER 13 (arrow) was opened into the anterior spinal artery for removal of PHIL. (C) Post removal DSA showed no filling defect in the anterior spinal artery. (D) The removed PHIL piece (arrow) and the TIGERTRIEVER 13 stent on gauze.
Case No 3
Left cerebellar AVM transarterial embolization was performed via a Sonic microcatheter at the left distal posterior cerebral artery (PCA) feeder with Onyx 18. Some Onyx material migrated to the left distal PCA artery, which was probably due to reflux from another feeder. Embolized Onyx material was retrieved by a TIGERTRIEVER 13 (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) The refluxed Onyx causing a filling defect in the distal segment of the left posterior cerebral artery (PCA) (arrow). (B) A TIGERTRIEVER 13 (arrow) was deployed at the level of the migrated embolic agent in the distal PCA. (C) Post removal DSA showed no filling defect and normal perfusion of the PCA.
Technique
All three cases were performed with a similar technique to retrieve the migrated embolic material. A Headway Duo 17 microcatheter (Microvention) was navigated over a Traxcess microwire (Microvention) beyond the embolic agent into the distal M4 segment of the MCA (case No 1), the thoracic anterior spinal artery (case No 2), and the distal PCA (case No 3). A TIGERTRIEVER 13 was inserted through the microcatheter and positioned over the embolic agent. The TIGERTRIEVER 13 was unsheathed and opened using the slider. The mesh of TIGERTRIEVER 13 was controlled with the slider to expand further. Under fluoroscopic guidance, the radiopaque embolic material was captured and with partial retraction of the TIGERTRIEVER 13 both the microcatheter and the TIGERTRIEVER 13 were retrieved, allowing successful removal of the distal embolic material in all three cases. There were no complications related to the procedure. Hemorrhage was excluded by cone beam CT immediately postprocedure, and a follow-up MRI 3 days later did not demonstrate any infarct in the corresponding area. All three patients were asymptomatic post thrombectomy.
Discussion
Liquid embolic material is an indispensable tool in the endovascular treatment of AVMs. Embolization related morbidity ranges from 3% to 11%. While the most feared complication is hemorrhage by rupture of the AVM, ischemic complications are also possible due to occlusion of normal neighboring arteries but also by migration of embolic material after reflux into normal branches. This may result in major disability even in distal arterial occlusions if an eloquent area is involved.
Stentrievers were introduced 10 years ago. Their efficiency in the successful removal of thrombi in stroke has been demonstrated in the meta-analysis of multiple randomized controlled trials.12 We also initially reported on the efficacy of stentrievers for the removal of coils13 and there have been a few case reports7–11 describing the use of stent retrievers in removing refluxed Onyx in parent arteries, such as the M1 segment of the MCA and basilar artery (table 2). However, the ability to obtain access to distal vessels is limited due to the size of the microcatheters that can be used and the potential risk of hemorrhage related to straightening of the vessels with subsequent bleeding from transmedullary arteries when the stentrievers are removed. Dedicated smaller devices, such as the Catch Mini (Balt, Montmorency, France) compatible with a 0.17 microcatheter, or the TIGERTRIEVER 13, compatible with a 0.13 microcatheter, have been developed to allow thrombectomy in small arteries distal to the sylvian point. Removal of migrated embolic agent requires distal navigation with microcatheters which carries a potential hemorrhagic risk and requires cautious progression with low traumatic microguidewires.
Reports published in the literature regarding mechanical removal of refluxed embolic material in arteriovenous malformation embolization
The efficacy of the TIGERTRIEVER 13 in distal thrombectomy led us to attempt its use for the removal of migrated embolic agent in distal branches. In the three patients reported in this study, we successfully employed the new stent retriever, TIGERTRIEVER 13, to extract the dislodged embolic material in small arterial branches in different arterial vasculatures. The TIGERTRIEVER 13 provided the following technical advantages during distal embolic material removal. First, the new stent retriever could be deployed in a microcatheter with a small outer diameter of 1.3 F which allowed not only access to small vessels but also the ability to navigate alongside and beyond the migrated embolic agent in order to deploy the stentriever in front of the embolus. Second, the degree of expansion of the stentriever can be controlled with the dedicated handle. Therefore, the TIGERTRIEVER 13 can be expanded without pushing or pulling on the device as with conventional stentrievers and an expansion can be obtained in a reliable way. To avoid hemorrhage caused by excessive friction and increased force during retraction, we chose to partially close the TIGERTRIEVER 13 before retrieving it. Care must be taken to avoid complete collapse of the device that may free the embolus again. The TIGERTRIEVER 13 appeared to be equally effective in retrieving different embolic agents, PHIL or Onyx, which have different consistencies.
It may be argued is it worth retrieving a small embolus in a distal artery. The added potential hemorrhagic risk must be balanced with the expected clinical impact. These may vary significantly with the functionality of the territory and degree of hypoperfusion according to the anastomosis. In all reported patients, the decision to remove the embolus was taken after progressive reduction of flow, as seen on fluoroscopy within a waiting period of 20 min.
To bring the Headway Duo microcatheter beyond the migrated embolic agent in the distal brain vessels, we used the smallest microcatheter compatible with the TIGERTRIEVER 13 in combination with an atraumatic wire, such a Traxcess (Microvention) or a Hybrid 7 (Balt). The wire itself was navigated as much as possible in a J shape in order to reduce the risk of perforation of a side branch. The microcatheter was brought 2 cm beyond the migrated embolic agent to avoid pushing onto the TIGERTRIEVER 13 when unsheathing it from the microcatheter. After progressively expanding the TIGERTRIEVER 13, it was contracted again and further reopened three times before partial contraction and slow extraction
Conclusion
Distal migrated embolic agents in various vascular territories may be retrieved using new generation stentrievers.
Footnotes
Contributors FLYH prepared the manuscript while RC provided important intellectual support. Both authors agreed on the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.