Article Text

Abstract
Purpose To report the first use of distal radial artery (dRA) access for a variety of neurointerventions and to demonstrate the safety and feasibility of this approach.
Methods A retrospective review of our prospective neurointerventional database of endovascular interventions was conducted and, between May and October 2019, all patients in whom the intervention was performed via dRA in the anatomical snuffbox were identified. Patient demographics, clinical information, procedural and radiographic data were collected.
Results 48 patients with a mean age of 64.4 years (range 35–84 years) were included. 27 patients were female. dRA access was achieved in all cases. Conversion to femoral access was required in five cases (10.4%) due to tortuous vessel anatomy and limited support of the catheters in the aortic arch. Interventions performed included aneurysm treatment (with flow diverters, Woven EndoBridge device placement, coiling or stent-assisted coiling), arteriovenous malformation and dural arteriovenous fistula embolization, carotid artery stentings, stroke thrombectomy, thrombolysis for central retinal artery occlusion, intracranial stenting, middle meningeal artery embolization, vasospasm treatment, and spinal angiography with embolization. Radial artery vasospasm was seen in two cases and successfully treated with antispasmolytic medication. No symptomatic radial artery occlusion or ischemic event was observed.
Conclusion dRA access is safe and effective for a variety of neurointerventions. Our preliminary experience with this approach is very promising and shows high patient satisfaction.
- aneurysm
- flow diverter
- angiography
- intervention
Statistics from Altmetric.com
Introduction
The neurointerventional field has recently adopted the transradial approach for diagnostic angiographies and interventional procedures.1–6 Faster postprocedural recovery, higher patient satisfaction, and fewer access site complications are some of the major advantages of wrist access over the transfemoral approach. The distal radial artery (dRA) approach in the anatomical snuffbox for endovascular procedures can be regarded as a refinement of the standard transradial approach.7 Puncture of the dRA preserves palmar collateral flow and is associated with limited risk of hand ischemia, decreased rates of radial artery occlusion, and preservation of the radial artery for possible future interventions.7–10 Recent cardiology studies evaluating the dRA approach have shown it to be a safe and feasible option for patients as well as operators.7–10 Distal radial access from the right side is comfortable for the patient as it allows for a natural hand position without wrist rotation as opposed to wrist supination for the traditional right transradial approach.7 11
However, only limited experience with the dRA access for neuroendovascular procedures exists and available literature mainly focuses on diagnostic cerebral angiography.12 13 Only two case reports are presently available which describe dRA access for mechanical thrombectomy in two patients14 and aneurysm treatment in one patient.15
In this study we describe our initial experience with a variety of neurointerventions via the dRA approach.
Materials and methods
This study was approved by our hospital institutional review board.
Between May and October 2019 we retrospectively analyzed our prospective neurointerventional database of endovascular interventions and identified all patients in whom the intervention was performed via dRA access in the anatomical snuffbox. Procedural and radiographic data were collected. Information on patient demographic data including age and gender was also obtained.
Results
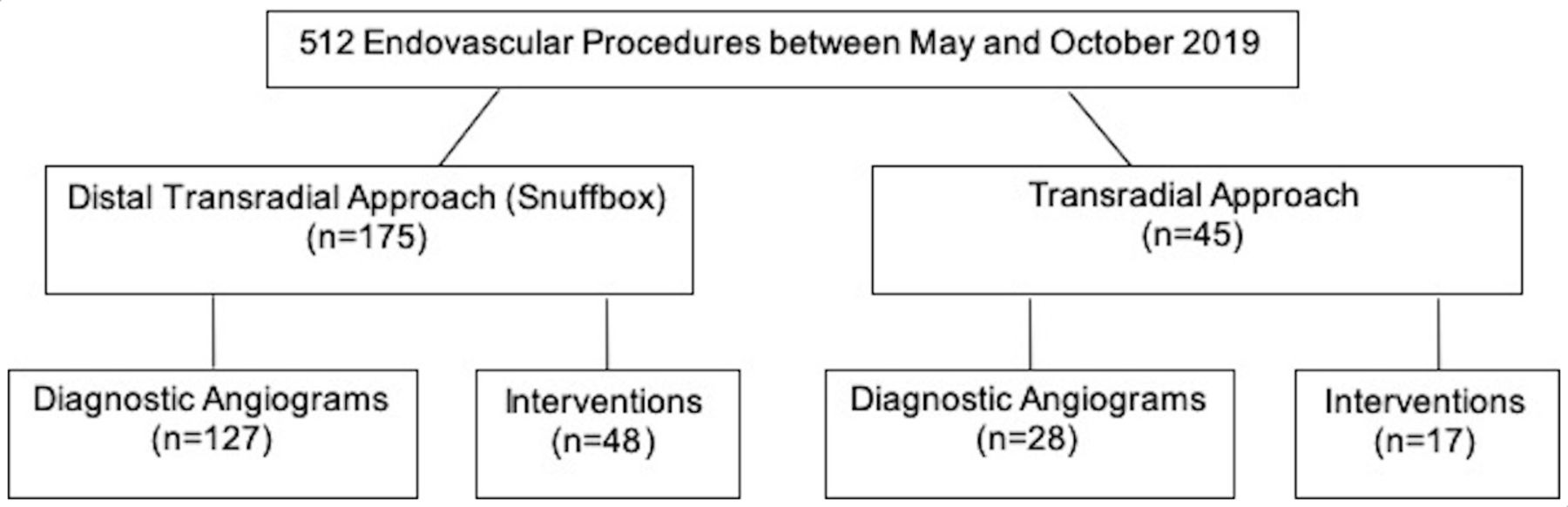
In a 6-month period between May and October 2019 we identified 48 interventions in 46 patients via dRA puncture in the anatomical snuffbox (figure 1). dRA access was achieved in all cases. However, five of our cases (10.4%) required conversion to femoral access, mainly due to tortuous anatomy and limited support of the catheters in the aortic arch. All other interventions (n=43) were successfully carried out via the dRA approach; no conversion to standard transradial access was necessary.

Overview of radial and distal radial artery procedures performed at our institution between May and October 2019.
Nineteen patients were male and 27 were female. Mean patient age was 64.4 years (range 35–84 years). Interventions performed included aneurysm treatment (with flow diverters, Woven EndoBridge (WEB) device placement, coiling or stent-assisted coiling), arteriovenous malformation or dural arteriovenous fistula embolization, carotid artery stenting, stroke thrombectomy, thrombolysis for central retinal artery occlusion, intracranial stenting, middle meningeal artery embolization, vasospasm treatment, and spinal angiography with embolization. A summary of patient demographics and procedural data is shown in table 1.
Summary of patient demographics and procedural data
Initial dRA access was obtained with a 6F Prelude Ideal hydrophilic sheath introducer (Merit Medical, South Jordan, Utah, USA) in all interventions. This particular sheath was used mainly for its braided design, providing stability for coaxial and triaxial catheter assembly systems. The periarterial soft tissues at the anatomical snuffbox were infiltrated with 1 mL lidocaine and 200 µg nitroglycerine for tumescent anesthesia. This technique of vasodilators and anesthetic medications in the snuffbox provided a window for ultrasound guidance for the micropuncture access and prevented the artery from vasospasm. The dRA was accessed under ultrasound guidance in the anatomical snuffbox for all interventions. Mean radial artery diameter was 2.3 mm (range 1.6–3.6 mm) with measurements available in 12/48 cases. In our practice, measurements were more often taken during the initial learning period when mostly diagnostic cerebral angiograms were performed via the dRA approach, with 41/127 measurements available showing a mean dRA diameter of 2.1 mm (range 1.6–3.0 mm) which is similar to the intervention group. With more operator experience, vessel size was deemed appropriate by visual inspection with only occasional measurements performed.
After insertion of the sheath, all patients received antispasmolytic agents (verapamil 5 mg, 200 µg nitroglycerin) and heparin 5000 IU. The administration of heparin is paramount for preventing radial artery occlusions. Prior to catheter exchanges, another dose of spasmolytic agents was administered through the radial sheath. In cases where an AXS Infinity LS Long Sheath (Stryker Neurovascular, Fremont, California, USA) or Fubuki guide catheter (Asahi Intecc, Tokyo, Japan) was used, the 6F sheath was also removed and the catheter was directly inserted into the dRA over the exchange wire (sheathless or bareback catheter use). The pulse oximeter probe was attached to the patient's thumb at the site of dRA access and oxygen saturation levels were monitored throughout the case. Activated clotting time (ACT) was measured at baseline and throughout the procedure with ACT goals of twice baseline. Additional intravenous doses of heparin were administered as needed.
Closure of the dRA access site was performed with the PreludeSYNC DISTAL radial compression device (Merit Medical). Patent hemostasis was achieved by slow release of air from the initially fully inflated (10 mL) balloon until a small amount of blood was visualized from the puncture site followed by reinflation of the balloon with 1–2 mL of air.
No symptomatic radial artery occlusions (RAO) or ischemic events occurred. Six patients underwent prior dRA access for diagnostic angiograms and four patients had prior traditional transradial artery access. One patient who previously underwent a transradial approach for a diagnostic angiogram was found to have a RAO at the time of intervention. In this case, we were able to recanalize the radial artery from a dRA approach and proceed with the intervention.
Four patients underwent dRA access for their follow-up angiogram and one patient had traditional transradial access. One patient who underwent dRA access for an intervention was found to have a distal and RAO on follow-up angiography. In this case we were not able to recanalize the vessel and converted to femoral access.
In this study we experienced two cases of radial artery vasospasm which were successfully treated with spasmolytic medication intraprocedurally.
Illustrative cases
Case 1
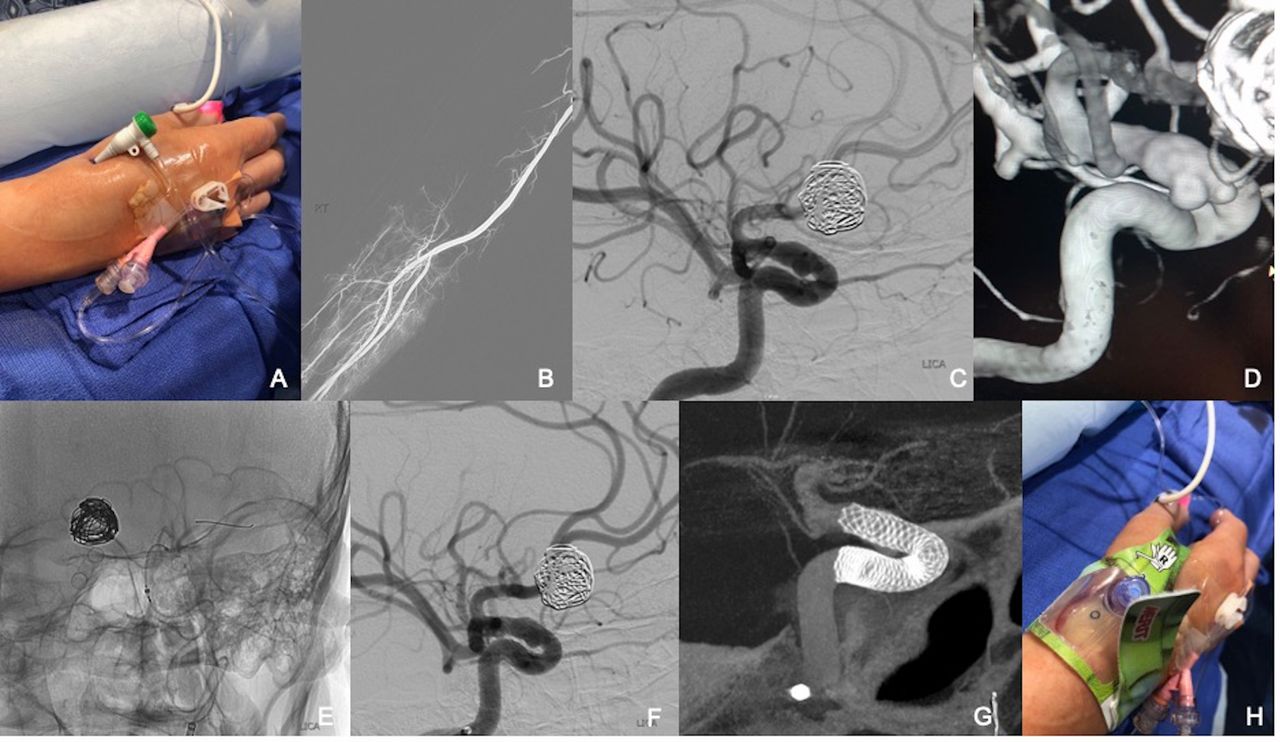
The right dRA was accessed under ultrasound guidance and a 6F Prelude Ideal hydrophilic sheath introducer was inserted (figure 2A). After administration of the spasmolytic medications and heparin via the radial sheath, a right radial angiogram was performed and the diagnostic catheter (Sim 2 glide catheter; Terumo, Fremont, California, USA) was advanced over the wire under roadmap guidance (figure 2B). The left internal carotid artery was selectively catheterized and digital subtraction angiography (figure 2C) as well as 3D-rotational angiography (figure 2D) was performed which revealed a multilobulated 8.8 mm left paraclinoid internal carotid artery aneurysm. The diagnostic catheter was exchanged for a Benchmark guide catheter (Penumbra, Alameda, California, USA). Coaxially through the Benchmark guide catheter, a Phenom Plus intermediate catheter (Medtronic, Irvine, California, USA) and a Phenom 27 microcatheter (Medtronic) were navigated over a Synchro 2 0.014 inch microwire (Stryker Neurovascular) into the left middle cerebral artery. A 4.25×25 mm Pipeline Embolization Device (Medtronic) was then successfully deployed across the neck of the left paraclinoid internal carotid artery aneurysm (figure 2E and F). Postprocedural Vaso-CT showed good wall apposition of the device (figure 2G). All catheters were withdrawn and the dRA access site was closed using a PreludeSYNC DISTAL radial compression device (figure 2H).

Successful deployment of a Pipeline Embolization Device via distal radial access.
Case 2
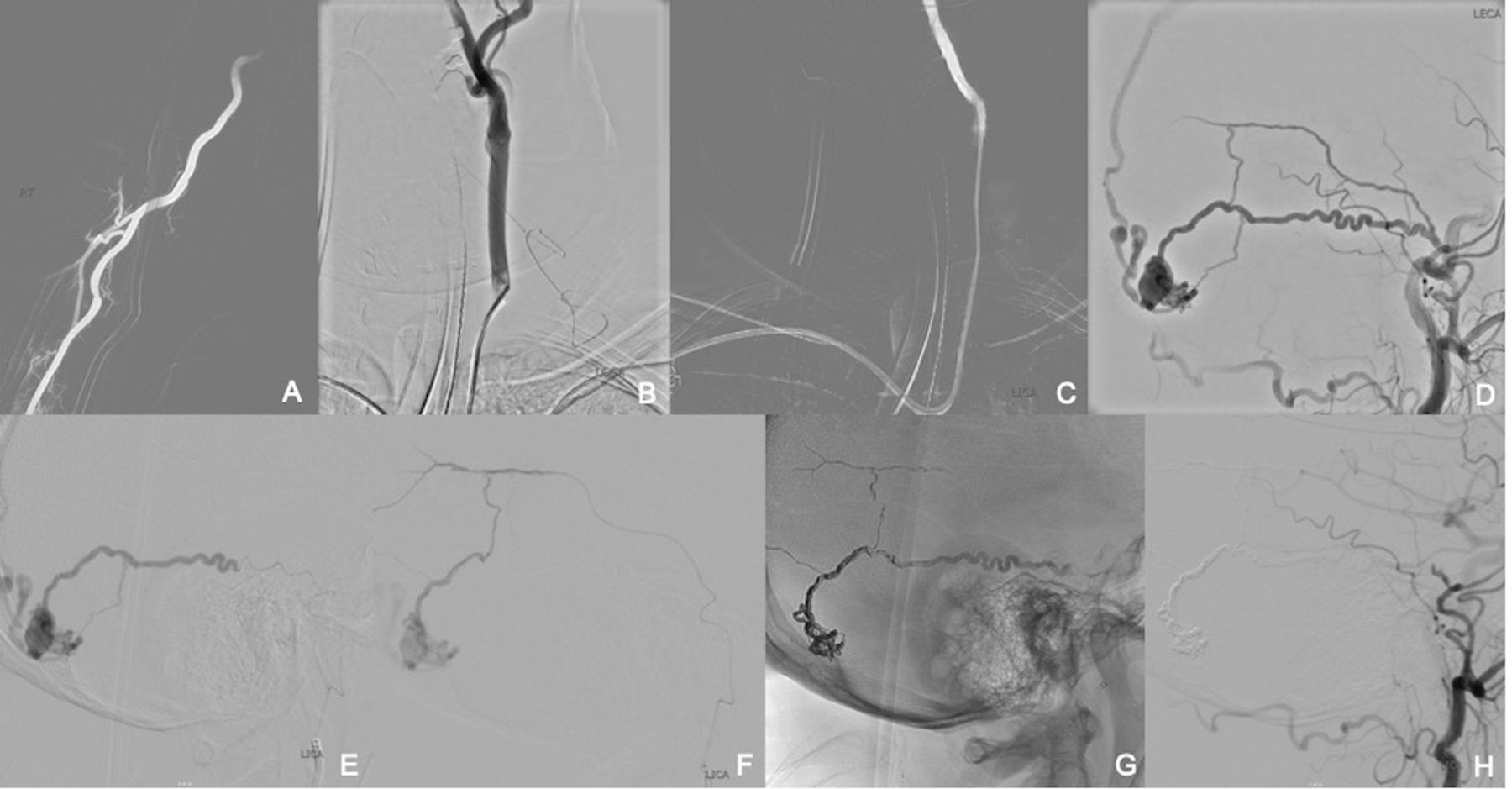
The right dRA was accessed under ultrasound guidance and a 6F Prelude Ideal hydrophilic sheath introducer was inserted. After administration of the spasmolytic medications and heparin via the radial sheath, a right radial angiogram was performed and the diagnostic catheter (Sim 2 glide catheter) was advanced over the wire under roadmap guidance (figure 3A). The left common carotid artery and subsequently the left external carotid artery was catheterized (figure 3B and C) followed by digital subtraction angiography which revealed a tentorial dural arteriovenous fistula with antegrade venous drainage into the superior sagittal sinus and the presence of a venous outflow pseudoaneurysm (figure 3D). The diagnostic catheter was exchanged for a Benchmark guide catheter. Within the Benchmark guide catheter a 5F Sophia intermediate catheter (MicroVention, Tustin, California, USA) and through that an Echelon 10 microcatheter (Medtronic) was advanced over a Synchro 0.014 inch microwire (Stryker Neurovascular) and into an arterial feeder of the fistula (figure 3E). The vessel was successfully embolized with glue (n-butyl cyanoacrylate) and the microcatheter was subsequently removed. A second arterial feeder of the fistula was then selectively catheterized using a Headway Duo microcatheter (MicroVention) (figure 3F) and embolized using Onyx 18 (Medtronic). A radiograph of the lateral skull showed the glue and Onyx cast (figure 3G). A follow-up angiogram of the left external and left internal carotid artery showed complete obliteration of the dural arteriovenous fistula and venous pseudoaneurysm. All catheters were withdrawn and the dRA access site was closed using a PreludeSYNC DISTAL radial compression device.
{kind=link}
{kind=link}
{kind=link}
Successful glue (n-butyl cyanoacrylate) and Onyx embolization of a left tentorial dural arteriovenous fistula via distal radial access.
Discussion
The transradial approach for endovascular procedures in cardiology was introduced in 198916 and several large interventional cardiology studies have shown a clear benefit of wrist access over the transfemoral approach, providing evidence of decreased morbidity and mortality, faster patient recovery time, higher patient satisfaction post-procedure, and even reduced cost.17–22
The neurointerventional field has been a little reluctant to switch from the transfemoral approach to an unfamiliar radial artery access. A few institutions have been performing occasional radial access procedures but, as in the majority of neurointervention practices, transfemoral access has remained the primary vascular access site for the past years.
However, given the indisputable advantages of wrist access, some neurovascular centers have recently accepted the challenge and switched their approach to a transradial access for diagnostic and interventional procedures with great success.1–6
The dRA puncture in the anatomical snuffbox is a little more difficult than the standard transradial approach as the vessel is smaller and requires ultrasound guidance for safe access. There is a learning curve when transitioning from femoral to radial and radial to distal radial access. Data on the use of the dRA approach for endovascular procedures are currently still limited in the interventional cardiology and neurointerventional literature,12 but available studies suggest that dRA access has additional advantages over the standard transradial access such as decreased rates of dRA occlusion and theoretically fewer ischemic events,7–10 significantly shorter post-procedural duration of hemostasis as well as slightly higher patient satisfaction.23 Although critical hand ischemia after transradial access is infrequent, the dRA approach may offer a theoretical advantage of reduced risk for ischemic hand complications as the origin of the superficial palmar branch lies proximal to the anatomical snuffbox access site and antegrade blood flow remains preserved in the event of a dRA injury or occlusion.24 25
In this study we were able to show that dRA access can be used for a variety of neurointerventional procedures. No intraprocedural access-related complications were encountered. We even used sheathless large-bore catheters up to 8F outer diameter (2.7 mm, Fubuki 6F, Asahi Intecc) through the dRA for our endovascular procedures. All our patients received an additional dose of antispasmolytic agents prior to catheter exchanges which, we believe, is a crucial part of the procedure in order to minimize the occurrence of radial artery vasospasm and the potential need for access conversion. Despite some complex interventions and the need for triaxial catheter systems, our access conversion rate was 10.4% which is within the 0.3–11% range currently reported in the literature.7–10 23
We encountered two patients with asymptomatic RAO, one after a diagnostic traditional transradial access procedure and the other at follow-up post dRA access intervention. In the case of radial artery thrombosis after traditional transradial access, we were able to recanalize the occluded radial artery in a retrograde fashion via the dRA approach—another advantage of dRA access previously described in the literature.26
RAO after transradial access is most commonly asymptomatic and occurs in 1–10% of cases.27–29 The occurrence of RAO in the cardiac literature based on sheath sizes used was summarized in a recent article30 showing RAO rates of 0% for 3F sheathless guiding catheters and 4F sheaths, up to 13.7% RAO rates for 5F sheaths, 30.5% for 6F sheaths, and 19% for 7F sheaths. Some of the information may be limited given the different time points at which RAO was evaluated and the possibility of spontaneous resolution of the thrombosis over time.
Conclusion
dRA access is a safe and effective approach for a variety of neurointerventional procedures. Several advantages previously described for diagnostic cerebral angiography via this approach such as decreased access site complications compared with the transfemoral approach, higher patient satisfaction rates, and shorter recovery times also apply for neurointerventions.
References
Footnotes
Contributors Study design: ALK, ASP. Data acquisition: all authors. Literature research: ALK, KdMR, FM. Data analysis and interpretation: ALK, ASP. Manuscript preparation: ALK, KdMR, ASP. Revision of manuscript for important intellectual content: FM, JS. Approval of final version of manuscript: all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests ASP is a consultant for Stryker, Cerenovus, CereVasc, Merit and Medtronic; received a research grant from Stryker Neurovascular and Medtronic; and has stocks in InNeuroCo.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.