Article Text

Abstract
Background and purpose The real-life application of DAWN and DEFUSE-3 trials has been poorly investigated. We aimed to identify the proportion of patients with acute ischemic stroke (AIS) eligible for late endovascular treatment (EVT) in our stroke center based on trial and more liberal selection criteria.
Methods All consecutive patients in our stroke registry (2003–2017) admitted within 5–23 hours of last proof of good health were selected if they had complete clinical and radiological datasets. We calculated the proportion of patients eligible for late EVT according to trial (DAWN and/or DEFUSE-3) and more liberal clinical/imaging mismatch criteria (including lower admission National Institutes of Health Stroke Scale score and Alberta Stroke Program Early CT Score for core estimation).
Results Of 1705 patients with AIS admitted to our comprehensive stroke center in the late time window, we identified 925 patients with complete clinical and radiological data. Among them, the proportions of late EVT eligibility were 2.5% (n=23) with DAWN, 5.1% (n=47) with DEFUSE-3, and 11.1% (n=103) with more liberal criteria. Considering late-arriving patients with large vessel occlusion (n=221), the percentages of eligible patients were 10.4%, 21.3%, and 46.6%, respectively. A favorable outcome was observed at comparable rates in treated patients selected by trial or liberal criteria (67% vs 58%, p=0.49).
Conclusions In a long-term stroke registry, the proportion of late EVT eligibility varied greatly according to selection criteria and referral pattern. Among late-arriving patients referred to our comprehensive stroke center, we found 5.6% eligible according to trial (DAWN/DEFUSE-3) and 11.1% according to liberal criteria. These data indicate that late EVT could be offered to a larger population of patients if more liberal criteria are applied.
- thrombectomy
- stroke
- CT angiography
- CT perfusion
Statistics from Altmetric.com
Introduction
Endovascular treatment (EVT) for patients with acute ischemic stroke (AIS) with proximal intracranial large vessel occlusion (LVO) is well demonstrated within the first 6 hours after onset when most patients have limited irreversible damage and significant amounts of salvageable brain tissue.1 Recently, two randomized clinical trials showed the effectiveness of late EVT up to 24 hours, based on radiological selection of patients with AIS having small core volume and either severe clinical symptoms (clinical-core mismatch in the DAWN trial) or a large perfusion deficit (perfusion mismatch in the DEFUSE-3 trial).2 3
Scant data exist on the number of late-arriving patients who are eligible for EVT in the real world.4 The calculation of the proportion of patients eligible for such treatment is of major importance for implementing DAWN and DEFUSE-3 results and, consequently, reorganizing stroke systems of care. Moreover, the precise measurement of lesion volumes with sophisticated imaging may be difficult in the acute stroke scenario due to patient agitation, contrast product contraindications, or technical problems with perfusion imaging. Therefore, simpler and more liberal criteria to determine the clinical/imaging mismatch could be useful in clinical practice.
The main purpose of our study was to identify the proportions of patients with AIS eligible for late EVT in our endovascular-capable stroke center using strict trial (DAWN and/or DEFUSE-3) criteria and more liberal clinical/imaging mismatch criteria. Moreover, we searched for clinical and laboratory variables independently associated with late EVT eligibility according to trial and liberal criteria. Then, we provided a description of our real-life cohort treated by late EVT and the outcome analysis at 3 months.
Materials and methods
Study design
We performed a retrospective analysis of all patients with AIS admitted to our comprehensive stroke center from January 2003 to December 2017, using the Acute STroke Registry and Analysis of Lausanne (ASTRAL) as our data source.5 ASTRAL is a single center-based cohort of all AIS patients admitted to the stroke unit and/or intensive care unit of the Lausanne University Hospital within 24 hours after last proof of good health (LPGH). It incorporates more than 250 prespecified demographic, clinical, laboratory variables and modern multimodal brain imaging items on over 4500 consecutive patients with AIS. The STROBE method (Strengthening the Reporting of Observational Studies in Epidemiology) was applied. The local ethics commission approved the scientific use of anonymized data from the ASTRAL registry.
Patient selection
We included late-arriving/treatable patients—that is, those admitted 5–23 hours after LPGH (including patients with unknown daytime stroke onset and wake-up stroke). This time window allowed patients to be potentially treated by an endovascular procedure between 6 and 24 hours. We then selected patients with complete datasets allowing an eligibility calculation according to trial criteria, including availability of good quality CT perfusion (CTP).
Patients were defined eligible according to the DAWN and DEFUSE-3 enrolment criteria, as reported previously.6 7 In our study cohort we applied the DEFUSE-3 criteria up to 23 hours; this allowed a combined evaluation of trial eligibility in the late time window and was based on the assumption that clinical outcomes were better in later than earlier treated patients.8
In addition, we proposed more liberal and pragmatic selection criteria for late EVT that included less severe stroke on admission (National Institutes of Health Stroke Scale (NIHSS) score ≥5), mild pre-stroke disability (modified Rankin Scale (mRS) ≤2), non-contrast CT (NCCT) Alberta Stroke Program Early CT Score (ASPECTS) cut-offs for core volume estimation (≥5), and presence of internal carotid artery (ICA), M1, proximal M2 or basilar artery occlusions on CT angiography (CTA). Moreover, the liberal criteria required a clinical/imaging mismatch in the anterior circulation strokes defined as: NIHSS 5–9 and ASPECTS ≥8; or NIHSS ≥10 and ASPECTS ≥7; or NIHSS ≥20 and ASPECTS ≥5. For posterior circulation (pc) stroke, eligibility required pc-ASPECTS ≥8 and absence of bilateral (transverse) pontine or midbrain infarction. The choice of ASPECTS for infarct core estimation reflects the intent of the liberal criteria to offer EVT to a wider proportion of late-arriving patients, even in centers where access to advanced imaging is limited.
We measured clinical outcome at 3 months using the mRS, either in person at the outpatient stroke clinic or in a standardized telephone interview by Rankin-certified medical personnel. A favorable outcome was defined as mRS ≤2.
Neuroimaging protocol
Multimodal CT-based imaging including NCCT, CTP, CTA, and post-contrast series, was performed in patients with suspected AIS as standard of care unless contrast contraindication existed. We performed CT on a 16-detector CT scanner until November 2005 and on a 64-multidetector CT scanner thereafter (LightSpeed VCT or Revolution, GE Healthcare, Milwaukee, Wisconsin, USA). We acquired NCCT and post-contrast series in axial scan mode from the skull base to the vertex (16 cm z-axis coverage) using the following imaging parameters: 120 kV peak tube voltage, 320 mA tube current, 5 mm slice thickness, 32 cm scan field of view (SFOV), 512×512 matrix. All CTP series were acquired with 80 kV peak tube voltage, 240 mA tube current, 32 cm SFOV, and 512×512 matrix. Images were centred on the level of the basal ganglia and third ventricle. We used 40 mm z-axis coverage until November 2005, 80 mm z-axis coverage until November 2015, and 120 mm z-axis coverage thereafter. CTP images were acquired for 50 s in cine mode before January 2011 and in shuttle mode thereafter. Delay was 5–7 s after beginning injection of 50 mL of iodinated contrast (Accupaque 300, iohexol 300 mg/mL, GE Healthcare, Glattbrugg, Switzerland) in an antecubital vein at a flow rate of 5 mL/s followed by 50 mL of 0.9% NaCl solution at the same flow rate.
We previously assessed inter-rater variability using Cohen's kappa on 100 consecutive CT scans of acute anterior circulation occlusive strokes and found an excellent agreement for ASPECTS (kappa 0.82). The use of ASPECTS for core volume estimation was supported by unpublished data from ASTRAL showing a moderate correlation between ASPECTS and core volume on CTP in the presence of LVO and in a late time window (Spearman ρ=−0.58, p<0.001). This assumption is in agreement with previous reports9 10 and supported by the fact that hypoattenuation on CT was proved to be highly specific for irreversible ischemic brain damage.11
We analysed CTP data using the Brilliance Workspace Portal (Philips Medical Systems, Cleveland, Ohio, USA) deconvolution software. The core and penumbra volumes were automatically generated using the appropriate mean transit time (MTT) and cerebral blood volume (CBV) thresholds (penumbra: MTT >145% of the contralateral side value, CBV ≥2.0 mL/100 g; core: MTT >145% of the contralateral side value, CBV <2.0 mL/100 g).12 We calculated the mismatch ratio as the ratio of the total ischemic volume (ie, core plus penumbra volumes) to the core volume.
Statistical analysis
We calculated the numbers of late EVT eligible patients according to the three sets of selection criteria (DAWN, DEFUSE-3, liberal). We chose the following denominators: (a) all AIS patients arriving within 24 hours; (b) all late-arriving patients (5–23 hours); (c) late-arriving patients with the necessary multimodal imaging available; (d) late-arriving patients with emergent LVO. We selected two scenarios: (1) the stroke population arriving at our comprehensive stroke center; and (2) the population from the primary catchment area (ie, patients for whom our institution is the hospital of reference, independently of the need for specialized stroke treatment).
We first performed a univariate comparison of the three groups of eligible patients according to their baseline characteristics. In order to account for correlations between the criteria, we used the method of generalized estimation equations (GEE).13 This method allows modelling correlated multiple outcomes using an approach inspired by quasi-likelihood. In our situation, the estimated parameters are OR, quantifying the association between a variable and the probability to satisfy each criterion, and ratios of odds ratios (ORR), quantifying the relative strength of the associations.
We then performed a multivariate analysis to identify independent variables associated with late EVT eligibility according to trial and liberal criteria. All demographic, clinical, and laboratory variables at baseline, as well as pre-stroke treatments and vascular risk factors, were included in this analysis. We used a logistic regression model and implemented a variable selection method via backwards elimination of variables with least significant ORs, until all ORs were significant. When needed, we inserted the last eliminated variable back into the model until good calibration was reached. We used non-significance of the Hosmer–Lemeshow test as the criterion for good calibration. In all analyses the level of significance was set at 5%. All analyses were performed with R version 3.4.2 software.
Results
Study population
During the observational period, four denominators emerged according to the methods described above: we identified (A) 4653 patients with AIS arriving between 0 and 24 hours; (B) 1705 (36.6%) late-arriving (5–23 hours from LPGH) AIS patients; (C) 925 (19.9%) late-arriving AIS patients with complete clinical and radiological datasets for investigating eligibility criteria; and (D) 221 (4.7%) late-arriving patients with LVO. The flow chart of eligible patients is depicted in figure 1. Additional information on the population selection process is available in online supplementary table e–1.
Supplemental material
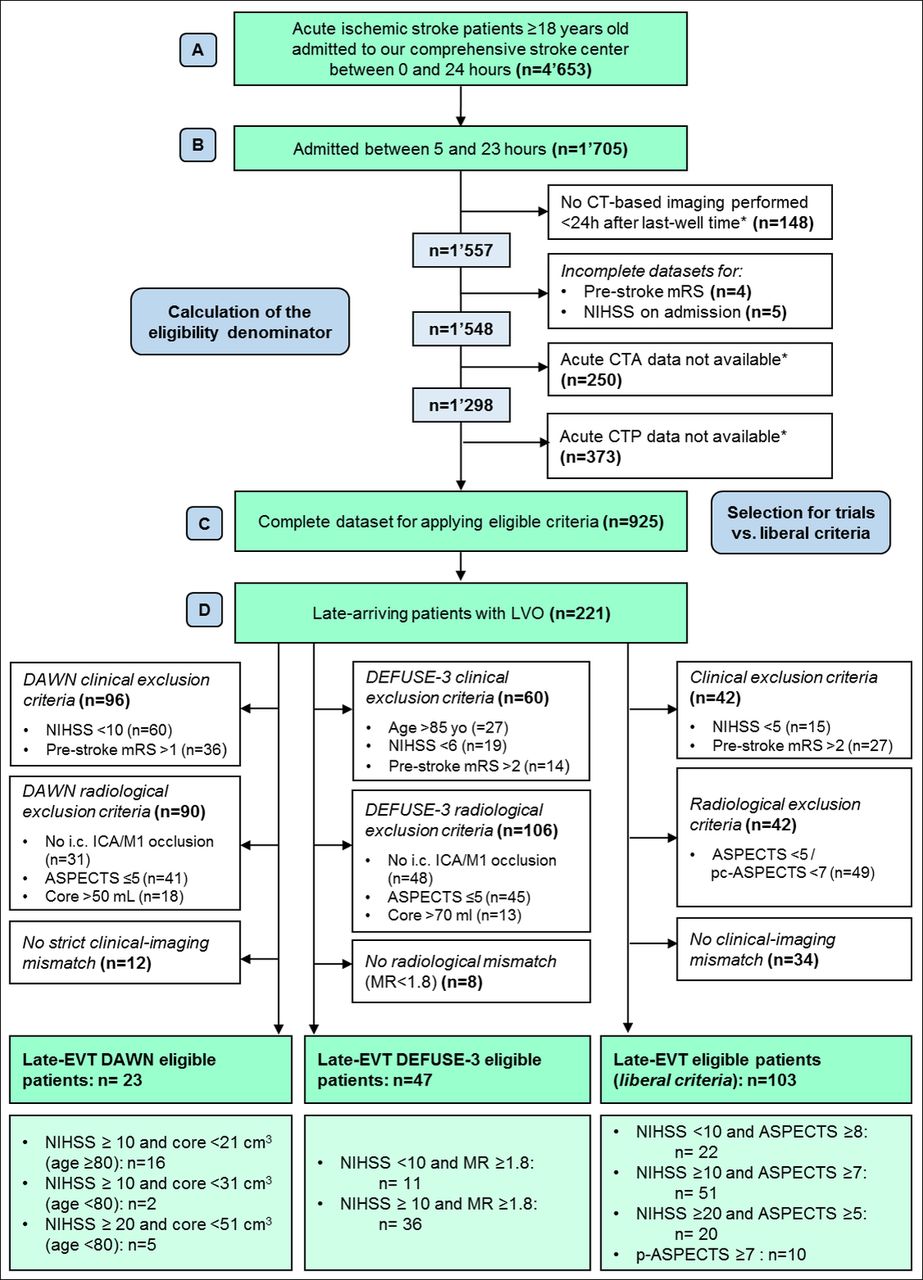
Flow chart eligibility in our comprehensive stroke center. We first identified four denominators: (A) total number of patients with acute ischemic stroke (AIS) admitted to our institution between 0 and 24 hours over the study period; (B) number of patients with AIS admitted late (5–23 hours); (C) number of late AIS patients with complete datasets; and (D) late-arriving patients with emergent LVO. We then applied the DAWN criteria, DEFUSE-3 criteria, and more liberal selection criteria to identify patients with AIS eligible for late endovascular treatment (EVT) accordingly. *See online supplementary table e–1 for additional information about radiological exclusion criteria.
In the main group of interest (C), the median age was 72.3 (IQR 20.5) years, 444 (48.0%) patients were female, and median NIHSS score on admission was 5 (8). Two hundred and twenty-seven (24.5%) patients were distant referrals, sent from community hospitals or bypassing distant emergency departments. Other characteristics of group C are shown in online supplementary table e–2.
Frequency of late EVT eligibility
For DAWN eligibility, 96 patients were excluded for clinical reasons, mainly lower stroke severity on admission (NIHSS <10, n=60) (figure 1). In addition, 90 patients did not meet the radiological criteria. A small number of patients (n=12) did not have the minimal clinical/core mismatch. Finally, only 23 patients were eligible for late EVT according to the DAWN criteria.
When applying the DEFUSE-3 criteria, 60 patients were excluded on a clinical basis. Moreover, approximately half of the patients did not have radiological inclusion criteria, mainly due to the distal site of vascular occlusion (n=48). The required radiological mismatch was absent in 8 patients, leading to 47 eligible patients according to DEFUSE-3 trial criteria. Overall, 52 patients satisfied DAWN and/or DEFUSE trial criteria.
Using our more liberal evaluation, we excluded 42 patients for clinical reasons, mainly based on higher pre-stroke disability. An additional 42 patients did not exhibit the radiological criteria. We did not find the more liberal clinical/core mismatch in 34 patients and finally identified 103 eligible patients. Ten of the patients presented with a posterior stroke from basilar artery occlusion which we considered eligible.
In the population from the primary catchment area only (n=698), 12 patients were eligible for late EVT based on DAWN criteria, 18 on DEFUSE-3 criteria, and 53 with less stringent criteria (online supplementary figure e–1).
Supplemental material
The proportions of late EVT eligibility for the three denominators A, B, and C are shown in figure 2 for the primary catchment area (figure 2a) and comprehensive (figure 2b) populations. Among late-arriving patients with complete clinico-radiological assessment (ie, denominator C), the proportions of late EVT eligibility were 2.5% with DAWN, 5.1% with DEFUSE-3, and 11.1% with more liberal criteria. Considering only the primary catchment area, the percentages were 1.7%, 2.6%, and 7.6%, respectively.
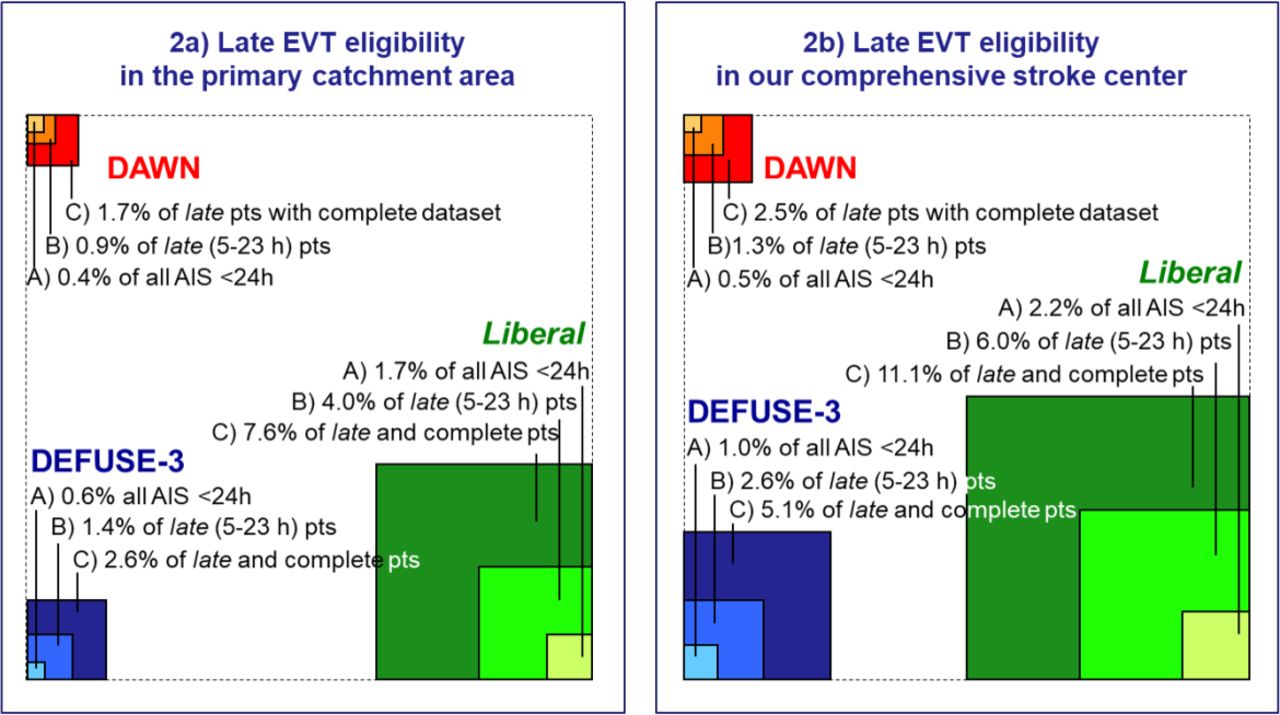
Proportion of patients with acute ischemic stroke (AIS) eligible for late endovascular treatment (EVT) according to DAWN, DEFUSE-3, and more liberal criteria from all patients with AIS admitted in the first 24 hours of last proof of good health, patients admitted late (5–23 hours), and patients admitted late with complete neuroimaging protocols. The data refer to our primary catchment area (A) and our comprehensive stroke centre (B).
The proportions of late EVT eligibility for patients with emergent LVO (ie, denominator D) are shown in online supplementary figure e–2. DAWN criteria would allow treating 10.4% of late-arriving patients with LVO, while 21.3% would be eligible according to DEFUSE-3 selection criteria. Adopting our liberal approach, 46.6% of patients with LVO would be suitable for late EVT.
Supplemental material
Characteristics of the eligible patients
We found a partial overlap between the three eligibility groups. Fifty-two patients fulfilled the strict trial criteria (DAWN and/or DEFUSE-3). All but five DAWN-eligible patients were also DEFUSE-3-eligible (18/23, 78.3%) and 18/47 (38.3%) DEFUSE-3-eligible patients were also DAWN-eligible. Among the 103 liberal criteria patients, 45 fulfilled the strict trial criteria. Only seven trial-based patients did not match the liberal criteria; these patients did not present the less stringent clinical/core mismatch but all showed the pure radiological mismatch (figure 3).

{kind=link}
{kind=link}
{kind=link}
DAWN (n=23, in red), DEFUSE-3 (n=47, in green), and liberal (n=103, in blue) late endovascular treatment (EVT)-eligible patients in our late-arriving acute ischemic stroke population. Circles show the partial overlaps between the three groups of patients: 52 patients fulfilled DAWN and/or DEFUSE-3 criteria whereas 45 liberal patients also matched the trial criteria. All but five DAWN-eligible patients were also DEFUSE-3-eligible, and 18/47 (38.3%) DEFUSE-3-eligible patients were also DAWN-eligible. Only seven trial-eligible patients did not present the liberal criteria.
In the univariate comparison of baseline characteristics (online supplementary table e–3), the two groups of trial criteria patients appeared similar, except for a higher NIHSS on admission and a higher prevalence of smoking in the DAWN-eligible patients. When comparing the trial and liberal eligible patients (table 1), we found the following radiological differences: trial-based patients had lower ASPECTS, higher frequency of M1 occlusions, higher core volumes, higher penumbra volumes, and higher mismatch ratio.
Demographics, clinical, and radiological characteristics of patients eligible for late EVT according to trial (DAWN and/or DEFUSE-3) and liberal criteria
Factors associated with late EVT eligibility
Among all late-arriving patients with AIS, EVT eligibility based on the strict trial criteria was independently associated with neurological signs such as hemiparesis, visual field defects and eye deviation, and with a shorter delay to hospital arrival. The variables implicated in determining EVT eligibility using the more liberal criteria were: lower pre-stroke disability, higher NIHSS on admission, eye deviation, hypercholesterolemia, and shorter delay to hospital arrival (table 2).
Independent predictors for late EVT eligibility according to trial and liberal criteria in late-arriving patients with AIS (n=925)
EVT procedures performed in real life and outcome analysis
Sixty-four patients arriving in the late time window underwent EVT over the study period. Four (6.4%) and 13 (20.3%) treated patients fulfilled the DAWN and DEFUSE-3 criteria, respectively. Thirty-nine of the treated patients (60.9%) complied with the proposed liberal approach. The proportion of late EVT among all revascularization procedures increased from 7% in the 5 years preceding presentation of the DAWN results (May 2017) to 21% after presentation, resulting in a relative increase of 200% in the last 8 months of the study period (online supplementary figure e–3). A favorable outcome was observed at comparable rates in treated patients selected by trial or liberal criteria (67% vs 58% respectively, p=0.49) (table 1).
Supplemental material
Discussion
In this study we performed a single-center analysis to determine the percentage of patients who could benefit from EVT in the extended time window. We found that the proportion of patients with late EVT eligibility varied greatly according to the selection criteria and referral patterns. Among patients with AIS admitted late to our comprehensive stroke center and assessed with a multimodal neuroimaging protocol, we found that 2.5% were eligible according to DAWN trial criteria and 5.1% according to DEFUSE-3 trial criteria. This proportion reached 11.1% when more liberal selection criteria were applied. Considering only the local population in the primary catchment area, these percentages fell to 1.7%, 2.6%, and 7.6%, respectively.
A previous study performed in our stroke center reported that 10.5% of all patients with AIS presenting within 6 hours of symptom onset were eligible for EVT according to the American Heart Association/American Stroke Association guidelines.14 The frequency of EVT eligibility was higher (17.7%) if less restrictive criteria were adopted. We expected these percentages to be lower in the late-arriving AIS population, mainly because of the strict selection criteria used in the randomized clinical trials, but also because patients with LVO seem to arrive earlier at the hospital.15 Another published study on late EVT eligibility in a stroke center found that 1.7% of all patients with AIS qualified for enrolment in the DAWN trial and 2.2% for enrolment in the DEFUSE-3 trial.4 To the best of our knowledge, our study is the first to examine late EVT eligibility in a real-life scenario.
Several factors could contribute to the low eligibility for late EVT in real life. First, a substantial proportion of late-arriving patients were excluded due to lack of a complete neuroimaging protocol. In addition to the well-known contraindications to iodinated contrast (allergy, renal impairment), we did not obtain perfusion imaging for a non-negligible number of patients in our CT-based emergency center due to ordering failures or moving patients. Second, we found that approximately two-thirds of late-presenting AIS patients did not meet the clinical inclusion criteria required by the trials due to age (>85 years), important pre-stroke disability (mRS >2), or too low NIHSS score on admission. Third, late-presenting LVO strokes commonly had larger core volumes than the thresholds (50 and 70 mL) needed for trial eligibility.
As a meaningful finding, we identified a LVO in 23.9% of late-arriving patients with AIS. This defines a target subpopulation of stroke patients that should be promptly identified as potentially suitable for revascularization treatment. Our analysis showed that about one out of four late-arriving patients with LVO could be treatable if trial criteria were adopted. The application of more liberal criteria in this population could allow treating up to one of two patients.
We showed that DEFUSE-3 criteria, including patients with lower NIHSS score, higher pre-stroke disability, and larger core volumes, allowed enrolling a higher proportion of patients compared with the DAWN trial criteria. As a result, all DAWN-eligible patients except for those aged >85 years were also eligible for the DEFUSE-3 trial in our cohort. Taken together, patients satisfying criteria of at least one of the two trials (DAWN and/or DEFUSE-3) extended EVT eligibility to 5.6% (n=52/925) of AIS patients admitted late to our comprehensive center. Our proposed more liberal selection criteria, characterized by lower NIHSS on admission and mRS of up to 2, extended EVT eligibility to twice as many patients. Moreover, using ASPECTS for core volume estimations, the liberal approach seems more feasible in the real-word clinical practice.
In our study, eligible patients according to trial criteria were best identified using clinical factors including hemiparesis, visual field defects, and eye deviation. As predictors of liberal eligibility, we confirmed eye deviation but also found hypercholesterolemia and the expected lower pre-stroke disability and higher admission NIHSS. In keeping with infarct growth over time16 and the usual associated reduction of salvageable tissue, we found that delay from stroke onset (or LPGH) to hospital arrival predicts lower eligibility according to both trial and liberal criteria. Despite the fact that carefully selected late and unknown onset patients have major benefit from recanalization,2 3 8 'time is still brain' both in the pre- and intra-hospital phase.
Although the number of late-treated patients in our center is insufficient for an appropriately adjusted clinical outcome analysis, we showed a similar rate of favorable outcome in late-treated patients satisfying strict or liberal criteria. This finding might indicate that a proportion of trial-ineligible patients may still benefit from late treatments if less stringent criteria are used, as recently suggested.17 18 Moreover, data from EVT-treated patients in earlier phases (up to 8 hours from onset) showed that revascularization therapy was still associated with a favorable clinical outcome in the presence of higher core volumes (ie, ASPECTS ≤5 on diffusion-weighted imaging).19 Similarly, it has been shown that patients not fulfilling guideline criteria for EVT within 6 hours after onset still benefit from mechanical thrombectomy, even in cases exceeding recommendations for onset-to-groin puncture time.20 These studies might support a progressive widening of EVT selection criteria in the late time window.
Our study could have several and significant implications for triage, resource allocation, and hospital referral re-organization in order to maximize patient selection for mechanical thrombectomy in the extended time window. The higher frequency of patients who could receive late EVT in the comprehensive stroke center compared with the local catchment area shows that endovascular-capable centers need to develop emergency medical services and close collaborations with referral facilities in order to deliver advanced treatments. Moreover, we observed a large increase in registered late EVT procedures after presentation of the DAWN results, suggesting that recanalization procedures could be implemented rapidly and successfully in clinical practice.
The strengths of our single-center study are the large number of patients with AIS with a thorough homogeneous work-up and the consecutive availability of patients with advanced acute neuroimaging since 2003.
Our study has several limitations, mainly due to its retrospective and single-center nature. First, eligibility in our wider catchment area might not be entirely representative because of fewer referrals before the presentation of the DAWN results; however, our analysis of the primary catchment area should correct for this error. Moreover, advanced neuroimaging information, especially regarding perfusion imaging of referred patients, was not available for a minority (n=373, 21.9%) of late-arriving AIS patients and this likely underestimated the proportion of patients with late EVT criteria. Regarding the neuroimaging protocol, we included only patients with AIS with CT-based assessment of core and penumbra volumes due to the small number of MRI-assessed patients in the ASTRAL registry (n=42, 0.05% of late-arriving population); therefore, we were not able to investigate the imaging modality differences on eligibility and outcome analyses. In addition, the threshold model used for core and penumbra volume reconstructions was different from that adopted in the CT arms of the recent EVT trials,21 which may affect the evaluation of the DAWN and DEFUSE-3 criteria in clinical practice. Even if not validated in a clinical trial setting, it is a well-established model, based on a systematic evaluation of all perfusion-CT parameters.12 Finally, our number of treated patients is too small for meaningful interpretation and therefore outcome analysis results should be treated with caution.
Conclusions
In our comprehensive stroke center, depending on the inclusion criteria used (trial vs liberal), 5.6% to 11.1% of late treatable AIS patients with complete neuroimaging protocols may be eligible for revascularization procedures. This translates to 23.5% and 46.6%, respectively, of late-arriving AIS patients with LVO admitted to our institution. Overall, we showed that, by applying a more liberal approach than strict trial criteria, EVT could be offered to twice as many patients. Efforts should be invested to re-organize stroke care systems and achieve comparable rates in real life.
Acknowledgments
The authors thank Melanie Price Hirt for English language correction and editing.
References
Footnotes
Twitter @stanfordNRAD
Contributors SN studied the concept and design, helped with analysis and interpretation, and prepared the article. DS, GSi and PV helped with interpretation of data and critical revision of the article for important intellectual content. MA carried out data analysis and interpretation and helped with preparation of the article. AE helped with data acquisition and analysis. VD and GSa helped with radiological data acquisition and critical revision of the article for important intellectual content. MW contributed to the conception and design and helped with the interpretation of data. PM studied the concept and design, helped with data acquisition, analysis and interpretation, critical revision of the article for important intellectual content, and study supervision.
Funding This work was supported by the Swiss National Science Foundation (grant number: 320030_182654).
Competing interests GSi: research grant from the Swiss Heart Foundation, congress travel support from Bayer and Shire and consultant for scientific advisory boards for Amgen and Daiichi-Sankyo. PV: research grants from the National Institute of Disease and Health Insurance (NIDHI/Belgium) through his institution; speaker fees from Daiichi-Sankyo, Pfizer and Alexion; honoraria from scientific advisory boards from Boehringer-Ingelheim. PM: research grants from the Swiss Heart Foundation and the Swiss National Science Foundation.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Anonymized data can be shared by request from any qualified investigator