Article Text

Abstract
Background Substantial clinical evidence supporting the benefit of mechanical thrombectomy (MT) for distal occlusions within the posterior circulation is still missing. This study aims to investigate the procedural feasibility and safety of MT for isolated occlusions of the posterior cerebral artery.
Methods We retrospectively reviewed patients from three stroke centers with acute ischemic stroke attributed to isolated posterior cerebral artery occlusion (IPCAOs) who underwent MT between January 2014 and December 2019. Procedural and safety assessment included successful recanalization rates (defined as Thrombolysis in Cerebral Infarction Scale (TICI) ≥2b), number of MT attempts and first-pass effect (TICI 3), intracranial hemorrhage (ICH), mortality, and intervention-related serious adverse events. Treatment effects were evaluated by the rate of early neurological improvement (ENI) and early functional outcome was assessed with the modified Rankin Scale (mRS) at discharge. A systematic literature review was conducted to identify and summarize previous reports on MT for IPCAOs.
Results Forty-three patients with IPCAOs located in the P1 (55.8%, 24/43), P2 (37.2%, 16/43), and P3 segment (7%, 3/43) were analyzed. The overall rate of successful recanalization (TICI ≥2b) was 86% (37/43), including a first pass-effect of 48.8% (21/43) leading to TICI 3. sICH occurred in 7% (3/43) and there were two cases with iatrogenic vessel dissection and one perforation. ENI was observed in 59% (23/39) and excellent functional outcome (mRS ≤1) in 46.2% (18/39) of patients who were discharged. The in-hospital mortality rate was 9.3% (4/43).
Conclusion Our study suggests the technical feasibility and safety of thrombectomy for IPCAOs. Further studies are needed to investigate safety and long-term functional outcomes with posterior circulation stroke-adjusted outcome assessment.
- stroke
- thrombectomy
- thrombolysis
Statistics from Altmetric.com
Introduction
Multiple randomized clinical trials (RCTs) have shown the effectiveness of mechanical thrombectomy (MT) for proximal large vessel occlusion (LVO) stroke within the anterior circulation.1 2 Even though randomized data are still missing, retrospective case series suggest a similar treatment benefit for proximal vessel occlusion stroke within the posterior circulation.3 4 Nevertheless, clinical evidence supporting MT for more distal vessel occlusions is still sparse, especially within the posterior circulation.5 6 Isolated posterior cerebral artery occlusions (IPCAOs) account for approximately 5–10% of all acute ischemic strokes.7 Due to the variability of vascular anatomy and occlusion sites, patients with IPCAO can have a wide range of clinical symptoms potentially leading to delayed hospital admission without acute treatment options for recanalization such as intravenous thrombolysis (IVT) and MT.8 9 Currently, stroke guidelines endorse MT for IPCAOs only on a class IIb level based on expert opinions and small study results.10 11 Therefore, decision-making for endovascular treatment of IPCAOs in daily clinical routine depends on the neurointerventionalist in charge as well as on local hospital stroke protocols.12
Recently, rapid advances in the development of smaller devices and concurrent neuroendovascular expertise have increased the possibilities of device navigation expanding boundaries to smaller cerebral arteries as possible targets for endovascular reperfusion techniques.13 14
Since MT could be a valuable treatment option for both primary isolated and secondary distal occlusions due to iatrogenic thrombus fragmentation during MT, further evidence is needed to determine whether initial recanalization attempts and secondary rescue maneuver are beneficial and safe.15
We conducted a retrospective multicenter study to investigate the endovascular treatment for IPCAOs, and hypothesized that thrombectomy is feasible and safe in this subgroup.
Methods
Systematic literature review
Two independent reviewers searched systematically for case reports and studies on thrombectomy of IPCAOs in the period between January 2010 and February 2020. The PubMed database was accessed using the following search term combinations: tigertriever OR preset lite OR baby trevo OR catch mini OR 3max OR (Isolated) posterior cerebral artery occlusion(s) OR distal AND thrombectomy(ies) OR Vessels OR artery(ies) OR cerebral artery(ies) OR occlusion OR arterial occlusion(s) OR vessel occlusion(s) arterial occlusion(s). Online supplementary figure 1 shows a flow chart of the conducted systematic literature search. Reasons for exclusion were recorded and listed. The literature search was generally confined to studies in English language.
Supplemental material
Patient selection
We analyzed prospectively collected patient data from three high-volume stroke centers treated consecutively with MT for ischemic stroke between January 2014 and December 2019. Inclusion criteria were defined as: (1) endovascular therapy for acute ischemic stroke due to (2) primary IPCAO, (3) without involvement of the basilar artery tip. Two independent neuroradiologists who were not participating in the intervention performed the retrospective case evaluation and selection for final analysis. To compare the efficacy of the endovascular treatment to patients with IPCAOs who received medical treatment only, a single-center chart review was performed (see online supplementary table 3).
Supplemental material
Procedural and functional outcome
The angiographic outcome was evaluated post-interventionally by digital subtraction angiography using the Thrombolysis in Cerebral Infarction Scale (TICI). The TICI classification was applied similarly to the anterior circulation adjusted to the relevant downstream territory of the posterior cerebral artery, with TICI 2b defined as successful with ≥50% of reperfusion.16 Further procedural feasibility assessment included the number of thrombectomy attempts with a first-pass effect (FPE) defined as TICI 3 after the first maneuver, time from groin puncture to first and final recanalization result, the rate of intervention-related serious adverse events such as iatrogenic dissections, new distal embolization, or the occurrence of asymptomatic and symptomatic intracerebral hemorrhage (aICH, sICH). sICH was defined in accordance with the Second European-Australasian Acute Stroke Study (ECASS II).17 Early treatment effects were evaluated by the rate of early neurological improvement (ENI), defined as a decrease in the National Institutes of Health Stroke Scale (NIHSS) score from baseline of at least 8 points or reaching 0–1, in accordance with previous studies.2 Functional outcome was assessed with the modified Rankin Scale (mRS) at discharge; early excellent and favorable functional outcome were defined as mRS ≤1 and mRS ≤2 at discharge, respectively. In four cases outcome data at discharge were not available due to a direct retransfer after the intervention to the referring hospital.
Statistical analysis
Standard descriptive statistics were used for all study endpoints. Univariable distribution of metric variables was described with median and IQR. For comparison of categorical variables, Fisher’s exact test was used. The Mann–Whitney U test (non-normally distributed data) and the unpaired Student’s t-test (normally distributed data) were used to compare continuous variables. The Wilcoxon signed-rank test was used to compare outcome data on hospital admission and at discharge. The significance level was set at α=0.05. All statistical analyses were carried out using SPSS Version 22 (SPSS, Chicago, Illinois, USA).
Results
Systematic literature review
A total of 10 retrospective studies and two case reports met the criteria and were included in the final review with an overall number of 82 IPCAO cases (online supplementary table 1). The largest series were published recently by Strambo et al (ASTRAL Registry) and Clarençon et al (TREVO registry), who reported on 21 and 22 cases, respectively. Both studies observed a potential benefit of MT for IPACO with successful recanalization (TICI ≥2 b) rates up to 100% and a cumulative excellent functional outcome (mRS ≤1) of 50% (21/42) at 90 days.18 19 Further studies on distal thrombectomy included mostly occlusions of the anterior circulation and reported on only a few IPCAO cases. In three studies the included cases derived from secondary downstream emboli after performing MT initially for LVOs. The primary choice of device favored stent retrievers over aspiration catheters (89%, 73/82). Successful recanalization of TICI ≥2b was achieved in up to 93% (76/82) of all cases. Cerebral hemorrhage was observed in two cases. In cases with available details on outcome information, four patients died early after MT including one patient with an initial basilar artery occlusion and secondary IPCAOs.
Baseline characteristics
Forty-three patients met the inclusion criteria and were treated between January 2014 and December 2019 (online supplementary table 2 provides exact time frames of each participating center). The median age was 78 (IQR 70–83) and 32.6% (14/43) were female. The relative frequency of patients treated with MT for IPCAO in relation to all thrombectomies performed during the study period at the participating center was 0.9% (95% CI 0.7% to 1.3%). Patients were admitted to the hospital with a median NIHSS score of 7 (IQR 4–10). The most common cardiovascular risk factors were arterial hypertension (72%, 31/43) and atrial fibrillation (42%, 13/43). Occlusions were located within the P1 (55.8%, 24/43), P2 (37.2%, 16/43), and P3 segment (7%, 3/43). Bilateral occlusions of the P1 segment occurred in four cases (9.3%, 4/43) and of the P2 segment in one case 2.3% (1/43). IVT was administered in 55.8% (24/43) of all patients prior to MT.
Procedural & Functional outcome
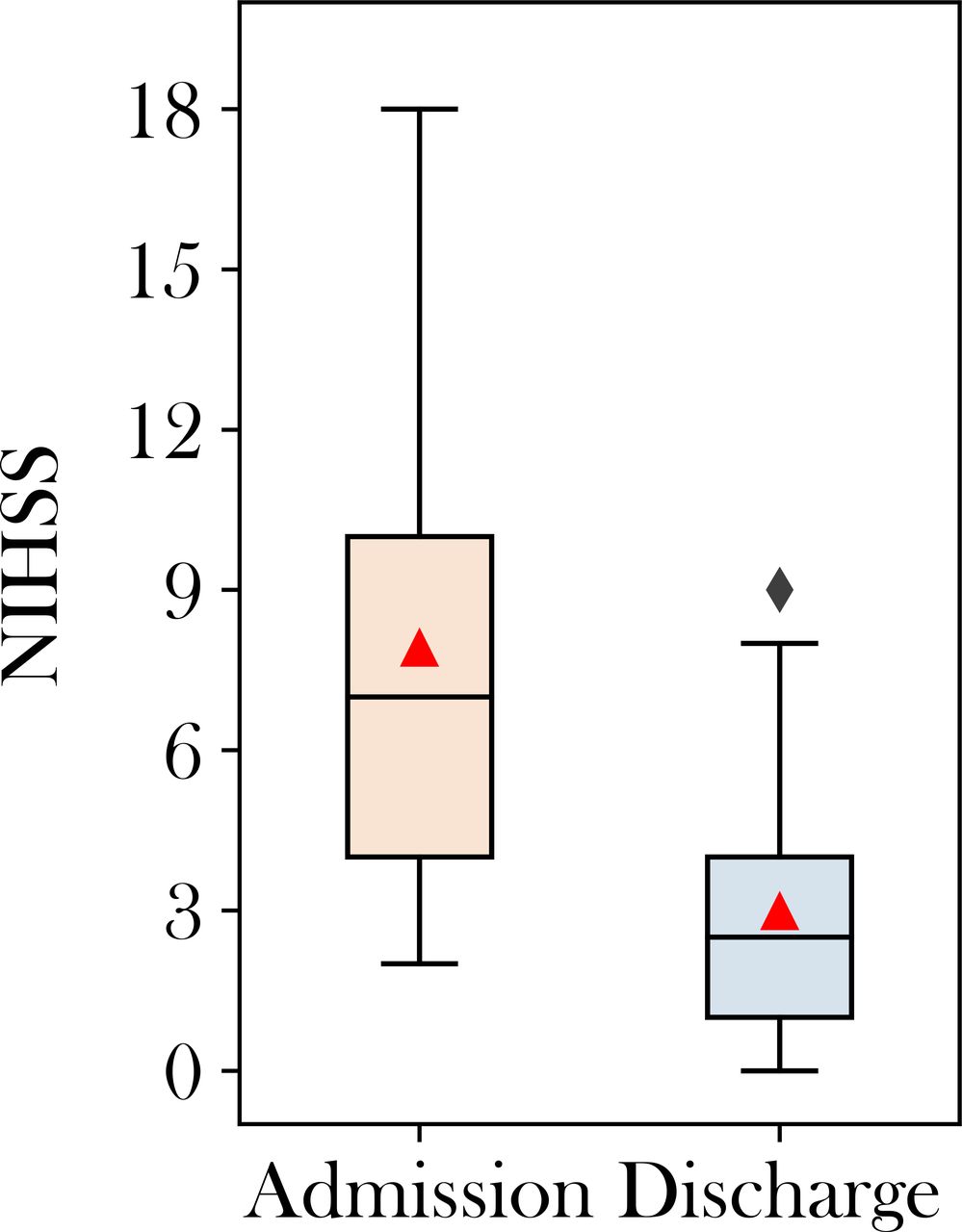
The median time from symptom onset to groin puncture was 181 min (IQR 151–267) and from groin puncture to the final recanalization result was 41 min (IQR 22–62). In 48.8% (21/43) of all cases the first recanalization maneuver led to a successful FPE of TICI 3. In cases with a successful FPE, the primary device was a stent retriever in 81% (17/21). Further MT attempts increased the overall rate of TICI 3 to 81.4% (35/43) with a median number of 1 (IQR 1–2) recanalization maneuvers. All cases with bilateral occlusions were completely recanalized (TICI 3) with one pass for each site. A comparison of baseline characteristics on admission showed no significant differences between patients with and without ENI (table 1). The median NIHSS score decreased significantly (p<0.001) from admission (7, IQR 4–10) to discharge (2.5, IQR 1–4; figure 1). Accordingly, ENI was observed in 59% (23/39) of all cases. At discharge, excellent (mRS ≤1) and favorable (mRS ≤2) functional outcomes were observed in 46.2% (18/39) and 66.7% (26/39), respectively. sICH and aICH occurred in 7% (3/43) and 2.2% (1/43), respectively. There were two cases of iatrogenic dissection (P1 segment 1/43; P2 segment 1/43) without being hemodynamically relevant and one case with iatrogenic perforation. In one case (2.3%, 1/43) a distal embolization to a new vessel territory occurred. The in-hospital mortality rate was 9.3% (4/43), including two patients with sICH of which one was attributed to the aforementioned iatrogenic vessel perforation which occurred during the successful treatment of a patient with bilateral P2 occlusions and concomitant basilar artery stenosis. Further deaths occurred in one patient who was referred from a peripheral hospital receiving IVT and underwent an unsuccessful thrombectomy attempt 8 hours after onset, and one patient with cardiac decompensation during in-hospital recovery.

{kind=link}
Boxplot comparison of National Institutes of Health Stroke Scale (NIHSS) on admission and discharge.
Overview of baseline characteristics with group comparison of patients with and without successful first-pass effects
Discussion
Whether isolated distal occlusions should be treated with endovascular thrombectomy or with best medical treatment only is still a matter of debate. Our retrospective multicenter analysis underlined that thrombectomy for IPCAOs is rarely performed.20 The use of endovascular thrombectomy to treat these occlusions seems to be technically feasible and safe, leading to successful recanalization in most cases, even after a failed FPE, with overall low rates of ICH.
To our knowledge, this study represents the largest case series published so far on the endovascular treatment of IPCAOs, and provides important procedural insights into this particular subgroup. The relative frequency of MT performed for IPCAOs in relation to the cumulative thrombectomy case volume treated at the three high-volume stroke centers during the study period was low (0.9%, 95% CI 0.7% to 1.3%). This finding may be explained by the low incidence of patients with IPCAO eligible for MT often arriving at the hospital outside of acute therapeutic time windows and the currently missing evidence supporting endovascular treatment for this subgroup.7–9
Evaluating the technical feasibility of thrombectomy for IPCAOs, we observed successful recanalization (TICI ≥2b) rates of 86% (37/43), which is comparable to previous large thrombectomy studies investigating proximal LVOs within the anterior and posterior circulation.3 21 22 Additionally, the systematic literature review showed similar results with successful recanalization in the vast majority of the published cases. However, in small retrospective case series and case reports, a selection bias cannot be ruled out, especially if reporting on novel devices. In our cohort, the technical efficacy was underlined by the high rate of successful FPEs (48.8%, 21/43), in some cases even with direct bilateral complete TICI 3 recanalization. This is an important finding, since the FPE is known to be strongly associated with a favorable functional outcome.23 If the FPE was not reached, further thrombectomy attempts still increased the TICI 3 rate up to 81.4% (35/43). A previous study observed that the first recanalization attempt has the highest per pass rate of successful recanalization and up to three attempts are safe, still leading to increased successful recanalization rates with favorable outcomes.24 Smaller vessels are known to be more fragile and, therefore, iatrogenic endovascular manipulation in these vessels during the endovascular procedure may be associated with higher rates of cerebral hemorrhage.25 In this study, sICH was observed in 7.1% (3/43) of cases, which is slightly higher than in previous thrombectomy landmark studies.2 Corroborating these findings, latest studies on MT for distal occlusions in the anterior circulation reported similar ICH rates, suggesting a safe endovascular procedure in smaller sized target vessels.5 6 26 Periprocedural thrombus fragmentation causing downstream embolism is a feared complication preventing complete recanalization and, subsequently, limits treatment effects of thrombectomy.27 Thus, the procedural feasibility and safety of our data and of previous studies are encouraging, since primary IPCAOs and also secondary distal occlusions could be possible targets attributed to iatrogenic thrombus fragmentation.28 Highlighting the relevance of the question whether or not IPCAOs should be treated endovasculary, Yeo et al recently reported that posterior circulation strokes are significantly associated with distal embolism when treated endovasculary.29
An early excellent outcome (mRS ≤1) was observed in 46.2% (18/39) of cases, which is in line with the two largest case series on IPCAOs published to date (55%, 11/20; 45%, 10/22)18 19 but exceeded those of previous RCTs (26.9%, 170/633).2 Even though discharge and 90-day functional outcomes cannot be compared directly, it has been shown that they are closely linked and mRS at discharge serves as a reliable surrogate for long-term outcome.30 Furthermore, these high rates of good outcome underline the problem that functional outcome assessment requires different interpretation for smaller vessel occlusions presenting at the hospital with mild symptoms compared to proximal LVOs. Outcome assessment of future RCTs for distal medium vessel occlusions might serve as a benchmark with global functional outcome measures such as the mRS stratified by the affected vascular territory.12 Furthermore, the NIHSS, as the most frequently applied scale for initial stroke assessment, tends to under-represent stroke symptoms of the posterior circulation.31 32 Accordingly, the median admission NIHSS score was lower (7, IQR 4–10) than in cohorts including only distal occlusions of the anterior circulation (mean 12±1, 95% CI 11 - 14).5 Since current clinical evidence supporting the benefit of MT for mild strokes (NIHSS ≤5) derives from retrospective (meta)-analyses, the association of lower NIHSS scores with IPCAOs might lead to less frequent decision-making for MT.33 Supplying eloquent brain areas such as the primary visual cortex and parts of the thalami, IPCAOs can lead to devastating life changes with a reduced quality of life and high rates of permanent disability, especially in cases with visual impairment.34 35 However, in this study the median NIHSS score had decreased significantly (p<0.001) to 2.5 (IQR 1–4) points at discharge, with high rates of ENI (59%, 23/39) suggesting a substantial treatment effect, especially in the context of low admission NIHSS scores (figure 1). Comparing the data with a single-center chart review (see online supplementary table 3) of patients treated with medical treatment only with and without IVT, the mean NIHSS score did not decrease significantly in these groups at discharge; however, the median NIHSS score on admission was non-significantly higher within the MT cohort (7 (IQR 4–10) vs 4 (IQR 2–10)). Nevertheless, there was only one patient with aICH in the medical cohort and no patient died during the hospital stay.
Limitations
Our study has certain limitations that derive from the retrospective study design. Additionally, long-term functional follow-up and outcome data for four patients at discharge were missing due to a direct retransfer to a peripheral hospital; however, even if these patients were classified as unfavorable, the overall outcome rates would still be favorable. Furthermore, the TICI scale was initially not designed for the posterior circulation and might carry inter-rater variability; however, most studies on posterior circulation stroke depend on the TICI scale.16
Conclusion
In times of advancing catheter technology, clinical evidence of thrombectomy for medium vessel occlusions is urgently needed to evaluate risk-benefit ratios. Our study suggests that thrombectomy for IPCAOs is feasible and relatively safe, at least at tertiary stroke centers with extensive neuroendovascular treatment experience. Further studies are needed to evaluate the efficacy and safety of thrombectomy for primary and secondary IPCAOs as well as the long-term functional outcome with posterior circulation stroke-adjusted functional outcome assessment.
References
Footnotes
CPS and HL contributed equally.
Contributors LM, HL, and CPS made substantial contributions to the conception and design of the work. Data acquisition was performed by CPS, LM, and HL. HL and LM performed the data analysis. Interpretation of the data was done by JF, PP, AK, MP, GB, HK, LM, CK, SMPP, MW and RC. LM drafted the manuscript and all of the other authors revised it critically for important intellectual content. All authors approved the final version to be published. They agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the manuscript are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests JF: Consultant for Acandis, Boehringer Ingelheim, Codman, Microvention, Sequent, Stryker. Speaker for Bayer Healthcare, Bracco, Covidien/ev3, Penumbra, Philips, Siemens. Grants from Bundesministeriums für Wirtschaft und Energie (BMWi), Bundesministerium für Bildung und Forschung (BMBF), Deutsche Forschungsgemeinschaft (DFG), European Union (EU), Covidien, Stryker (THRILL study), Microvention (ERASER study), Philips. PP: Consultant for Penumbra. RC: Consultant and/or proctor for BALT, Stryker, Microvention, Rapid Medical, Siemens Medical Systems. CPS: Consultant and/or proctor for Acandis, Balt, and Rapid Medical.
Patient consent for publication Not required.
Ethics approval Anonymized data were recorded in accordance with ethical review board approval and no informed consent was necessary after review (Ethics Committee of the Chamber of Physicians, Hamburg, Germany)
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data supporting the findings are available upon reasonable request from any qualified investigator for the purposes of replicating procedures and results, after clearance by the ethics committee.