Article Text

Abstract
Background There are no reports that describe complete flow control using concurrent transient rapid ventricular pacing or intravenous (IV) adenosine and afferent arterial balloon flow arrest to aid transvenous embolization of cerebral arteriovenous malformations (AVM). We describe our experience with the use of this technique in patients undergoing transvenous AVM embolization.
Methods Consecutive patients in whom transvenous embolization was attempted at our institute between January 2017 and July 2019 were included. Anatomical AVM features, number of embolization stages, technique of concurrent transient rapid ventricular pacing and afferent arterial balloon flow arrest, complications, and clinical and radiological outcomes were recorded and tabulated.
Results Transvenous AVM embolization was attempted in 12 patients but abandoned in two patients for technical reasons. Complete embolization was achieved in 10 patients, five of whom had infratentorial AVMs. All 10 had a single primary draining vein. Rapid ventricular pacing was used in nine cases; IV adenosine injection was used in one case to achieve cardiac standstill. Complete AVM nidus obliteration was achieved with excellent neurologic outcome in nine cases, with transvenous embolization alone in two cases, and with staged transarterial followed by transvenous embolization in the others. Two patients developed hemorrhagic complications intraprocedurally. One patient was managed conservatively and the other operatively with AVM excision and hematoma evacuation; both made an excellent recovery without any neurologic deficits at 3 months.
Conclusion Complete flow control using concurrent transient rapid ventricular pacing with afferent arterial balloon flow arrest technique is safe and feasible for transvenous embolization of select AVMs.
- arteriovenous malformation
- balloon
- intervention
- liquid embolic material
- technique
Statistics from Altmetric.com
Background
Transvenous embolization alone or following transarterial embolization has emerged as an effective treatment option for select cases of cerebral arteriovenous malformation (AVM).1–4 Several reports have demonstrated the safety and feasibility of this technique with a high cure rate.4 This is in sharp contrast to a far lower cure rate with transarterial embolization alone.5 However, transvenous embolization is a technically challenging procedure because it is difficult to selectively catheterize the draining vein and deliver embolizate into the nidus retrogradely against the high fistulous flow without incurring nidal rupture and hemorrhage.4 Systemic hypotension and temporary balloon occlusion of arterial feeders have been described for transvenous embolization.1 6
Transient cardiac standstill is well described in cerebrovascular surgery, where it is used to achieve a relatively bloodless surgical field during treatment of complex intracranial aneurysms.7 It was originally established via placing a patient on cardiopulmonary bypass with hypothermia, as described by Charles Drake.8 This goal is effectuated by creating severe controlled transient hypotension. The use of transient rapid ventricular pacing (RVP) for transvenous embolization of cerebral AVMs is an innovative strategy to achieve the same goal. This can also be achieved through systemic administration of an adenosine bolus, which results in a temporary cardiac pause.7 However, systemic administration results in a varied pharmacological response in terms of duration and severity of bradycardia and can lead to heart block and other cardiac dysrhythmias. Similar to cardiopulmonary bypass, RVP results in severe hypotension (<30 mmHg) with flattening of pulse pressure; however, anterograde bulk flow continues unabated in contrast to adenosine, which halts all forward flow during asystole.
To our knowledge, the previous literature on RVP is limited to case and technical reports or pertains to open cerebrovascular procedures.9–11 Use of total flow control with concurrent transient venous pacing and afferent arterial balloon occlusion to achieve complete flow arrest for transvenous embolization of AVMs is novel. We routinely use concurrent transient RVP and afferent arterial balloon occlusion to perform all transvenous embolizations for cerebral AVMs. In this case series, we describe the safety and effectiveness of this technique to facilitate transvenous embolization of AVMs.
Methods
Study population
We included consecutive patients with cerebral AVMs treated using transvenous embolization at our institution during a 2.5- year period (January 2017–July 2019) and performed a retrospective data analysis. All procedures were performed after patients or their family members provided informed consent. The institutional review board approved the study. Patients were identified using International Classification of Diseases 10th Revision (ICD-10) Q28.2 codes. The list was further screened by reviewing medical charts to identify patients who underwent transvenous embolization as a standalone strategy or in combination with transarterial embolization.
Transvenous AVM embolization was performed for small AVMs (≤3 cm) with a single primary draining vein where transarterial embolization was not feasible due to lack of a definite arterial pedicle, presence of multiple small feeders, or supply by tiny perforating arteries or en passage feeding arteries. Combined transarterial and transvenous approaches were used when both were feasible and had potential for complete obliteration of the nidus. For larger (>3 cm) AVMs, staged transarterial embolization procedures were performed to reduce the size of the nidus. Transvenous embolization was additionally considered if after staged transarterial embolization the AVM was not obliterated and its features were favorable for a transvenous approach. Every patient underwent preoperative brain magnetic resonance imaging (MRI) and cerebral angiography to elucidate the anatomy of the AVM.
We recorded demographics, clinical presentation, rupture status, Spetzler–Martin AVM grade, angiographic anatomical details, treatment modalities, angiographic follow-up, and clinical outcomes at last follow-up evaluation. Procedure-related complications were also recorded. Clinical outcomes were measured using the modified Rankin Scale (mRS). AVM obliteration was confirmed on a digital subtraction angiogram (DSA) obtained at 6 months. Further follow-up was done with an MRI study at 1 year.
Procedural details
The procedure was performed under general anesthesia with the patient intubated on mechanical ventilation and complete paralysis with continuous electroencephalography (EEG), somatosensory evoked potential (SSEP), and brainstem auditory evoked response (BAER) neuromonitoring. A left radial arterial line was established for continuous arterial pressure monitoring by an anesthesiologist. The bilateral femoral region and right neck were prepared and draped in sterile fashion. A local anesthetic was injected in both groin regions after which a 6-French (6F) right common femoral artery sheath and left femoral 6F venous sheath were inserted using a micropuncture set and modified Seldinger technique and confirmed fluoroscopically. The right internal jugular vein was accessed under ultrasound guidance, and the sheath was advanced under fluoroscopic guidance to the jugular bulb region, along with a 6F Benchmark catheter (Penumbra Inc., Alameda, CA, USA). In cases where we needed additional arterial access, we used a 6F right radial artery sheath. After establishing all vascular access, a 50 U/kg IV dose of heparin was infused, and an activated coagulation time (ACT) of >190 s was measured on the i-STAT analyzer (Abbott Laboratories, Lake Bluff, IL, USA), which is equivalent to an ACT of >250 s on most analyzers. This ACT was checked every hour and maintained for the duration of the case and reversed at the end of the case with systemic administration of protamine. From right common femoral artery access, a second 6F Benchmark guide catheter was advanced into the distal cervical internal carotid artery (for anterior circulation lesions) or vertebral artery (for posterior circulation lesions). A Scepter microcatheter balloon (MicroVention-Terumo, Tustin, CA, USA) was then parked in the main feeding artery. Left femoral 6F venous access was used to place a cardiac pacer in the right ventricle.
The 6F Benchmark catheter in the right internal jugular vein was brought up to the right sigmoid sinus and into the right transverse sinus, straight sinus, or superior sagittal sinus, depending on the location of the draining vein. Using a road map of the venous phase of the arterial injection, the target draining vein was catheterized using a Headway Duo microcatheter (MicroVention-Terumo) over a Synchro-2 Guidewire (Stryker, Kalamazoo, MI, USA). Arterial injections and roadmaps were repeated as necessary for safe navigation of the target draining vein or veins. This was routinely the most difficult and time consuming phase of the case. If the draining vein was small, a smaller catheter, such as a 0.013 in Marathon (Medtronic, Dublin, Ireland), over a 0.010 in Synchro-10 Guidewire (Stryker) was utilized. These were placed in the primary draining vein so that simultaneous injection of Onyx 34 embolizate (Medtronic) was possible into all secondary and tertiary veins. This is a key step ensure no secondary vein is excluded without adequate penetration of its draining nidus. Blockage of outflow from a draining vein without nidal penetration can lead to hemorrhage. If the venous pedicle was large enough, a second microcatheter (0.0165 in SL-10, Stryker) was parallel parked alongside the more distal microcatheter. This second catheter was kept farther out in the primary draining vein and used to deliver coils and subsequently n-butyl cyanoacrylate (NBCA) to anchor the more distal Onyx delivery catheter and for complete occlusion of the draining vein to maximize retrograde Onyx injection into the nidus (reverse pressure cooker technique).12 Additional maneuvers were performed as required, including the use of distal access catheters to deliver the venous catheter to overcome venous tortuosity as well as hybrid craniotomy for direct venous access and clip occlusion for reverse pressure cooker setup.
Once the draining vein was satisfactorily catheterized, the patient was placed in burst suppression confirmed by continuous intraprocedural EEG to minimize the cerebral metabolic rate of oxygen (CMRO2). The patient’s core temperature was allowed to drift to the 34°C–35°C range. An interventional cardiologist placed the right ventricular pacer wire through the left femoral vein access and performed tests to ensure cardiac capture at minimal settings. The pacing rate was preset at 180–200 beats per minute (bpm) and blood pressure was measured to assess the effectiveness of RVP. For younger patients, higher rates of 220 bpm were employed to achieve a sustained arterial pressure under 30 mmHg.
On ensuring that the desired severe systemic hypotension was effectively achieved through RVP, the systolic blood pressure (SBP) was lowered to 80 mmHg. Two experienced neurointerventionists were involved in the procedure: one in charge of the Scepter balloon and the Onyx catheter, and the other responsible for the transvenous coils and the NBCA delivery catheter. At this point, if there was a second venous catheter for complete venous occlusion, we started placing coils rapidly through this catheter to create a dense nidus of coils to help reduce anterograde venous flow and create a resistive body into which we would shortly place NBCA. This consisted of three to six coils slightly oversized to nominal vein diameter because they can easily expand compared to arteries. A mixture of NBCA and tantalum was prepared at 50% concentration and diluted with Lipiodol (Guerbet, Villepinte, France). The microcatheter was prepared for injection by flushing it with a solution of dextrose and water. Simultaneously, the second neurointerventionist prepared the Onyx catheter with DMSO, followed by loading the catheter with Onyx until the Onyx was just about to exit the catheter. At this point, all team members reviewed their respective roles, including the cardiologist, who was informed about the pace and stop commands. Burst suppression and hypotension were confirmed, and all unnecessary conversation in the interventional suite was halted.
Next, the principal feeding artery or arteries (basilar, vertebral, internal carotid, middle, or anterior cerebral) were occluded through inflation of the Scepter dual-lumen balloon. A timer was started so that the occlusion time was kept less than 5 min at a time, followed by 2 min of balloon deflation for revascularization prior to the next inflation.
At this time, with the Scepter balloon inflated, RVP was started; NBCA was injected to create complete venous outflow obstruction; and the second venous catheter was removed. We were therefore able to establish total flow control using cardiac RVP, arterial balloon flow arrest, and venous occlusion with coils and NBCA. Simultaneously, Onyx was aggressively injected retrogradely into the nidus. This was continued until we were at approximately 60–75 s of RVP for the first injection. At this point, the pacing was stopped and the heart was allowed to reperfuse for 30–60 s, followed by repeat RVP for less than 60 s with multiple cycles of RVP during a single balloon inflation. As Onyx injection continued, the RVP durations became shorter, averaging 20–30 s at a time. The Onyx injection was continued until every aspect of the previously noted nidus was completely opacified by Onyx. An outline of the original nidus was drawn on the monitor to guide this assessment. In all cases, we employed multiple cycles of balloon inflation and deflation and many more cycles of RVP during each balloon inflation to transvenously embolize the AVM.
Multiple angiographic runs were performed to assess any residual filling. Any residual nidus of concern was aggressively managed by continued Onyx embolization. It should be noted that as soon as the venous outflow was obstructed, visualization of the nidus became complicated and careful assessment of the delayed capillary and venous phases was required to see if any residual nidus was still filling. Postembolization angiographic runs were obtained to confirm complete AVM obliteration. On satisfactory occlusion of the entire nidus, anticoagulation was reversed and all catheters, balloons, and sheaths were removed. Often, the Onyx microcatheter remained adherent to the Onyx 34 cast, and it was retracted and cut at the right internal jugular vein percutaneous access site.
The patients were kept intubated and hypotensive (SBP <90 mmHg) overnight. They were extubated the following morning, with SBP parameters increased slowly by 10 mmHg per day.
Results
During the study period, we performed 70 AVM embolization procedures, of which 12 were attempted using the transvenous technique (table 1). In two of these cases, the draining vein could not be selectively catheterized due to complex venous anatomy (Cases 7 and 11), and the procedure was abandoned (these cases were treated with hybrid craniotomy or radiosurgery). Transvenous embolization was completed in 10 cases (table 2). All of these patients had a single draining vein. Five (of 10) patients had infratentorial AVMs. The detailed anatomical location of each AVM is provided in table 1. Ventricular pacing was utilized in nine cases; an IV injection of adenosine was used in one case (Case 8). Complete nidal obliteration was achieved in nine cases. It was achieved with transvenous embolization alone in two patients (Cases 1 and 9) and with staged transarterial followed by transvenous embolization in eight patients. Two patients developed hemorrhagic complications during the procedure. In one patient (Case 3) the hemorrhage was managed operatively with AVM excision and hematoma evacuation. In this case, retrospective analysis demonstrated a residual nidus that was difficult to appreciate during the case. The second patient (Case 10) had an intraventricular hemorrhage that was noted during the procedure. In this case, the cause appeared to be too distal a location of the primary venous catheter close to the nidus resulting in occlusion of a secondary vein without nidal penetration. This was managed by continued Onyx embolization under complete flow control until the intraventricular bleeding site was embolized and the bleeding stopped. The patient was managed with a ventriculostomy and made an excellent recovery. One patient (Case 2) died as a result of a pulmonary embolism 2 months after the embolization procedure. The nine other patients had favorable outcomes (mRS scores 0–2). The average clinical follow-up was 13 (range 6–36) months.
Clinical characteristics of patients in the study
Treatment details and functional outcomes
In one case (Case 7) we performed a small temporal craniotomy in the hybrid suite (hybrid craniotomy) for direct access of the vein. We used flow probes given the direct access to assess venous outflow during various stages of flow arrest. Controlled flow through the vein prior to RVP was 127 mL/min. On RVP this dropped to 37 mL/min. This finding attests that bulk anterograde flow still continued during RVP. After balloon inflation (during RVP) in both the middle cerebral artery and the anterior cerebral artery, the flow dropped to 2 mL/min. This confirmed our impression that concurrent RVP and arterial balloon arrest was effective in complete flow control.
figures 1–3 demonstrate a case of complete flow control with concurrent arterial balloon occlusion and RVP during transvenous embolization of a left cerebellar AVM. The patient presented with a Spetzler–Martin grade IV AVM in the left superior and middle cerebellar peduncle (Case 12). The AVM was fed by branches of the left superior cerebellar artery and the left anterior inferior cerebellar artery. Transarterial embolization of the left superior cerebellar artery feeders was performed, followed 2 months later by transvenous embolization for complete obliteration of the nidus.

Case 12. T2-weighted axial (A) and coronal (B) magnetic resonance images showing an arteriovenous malformation (AVM) in the left cerebellar hemisphere (arrows). Dilated draining vein can be appreciated as a large flow void (arrowhead). Anteroposterior (AP) projections of a left vertebral artery injection showing a left cerebellar AVM filling from the branches of the left superior cerebellar artery and left anterior inferior cerebellar artery (arrows) on AP (C) and lateral (D) projections. The main drainage is into the vein of Galen (solid arrow) and indirectly to the torcula (open arrow) with an area of venous stenosis past the AVM nidus on lateral projection (arrowhead) (E).
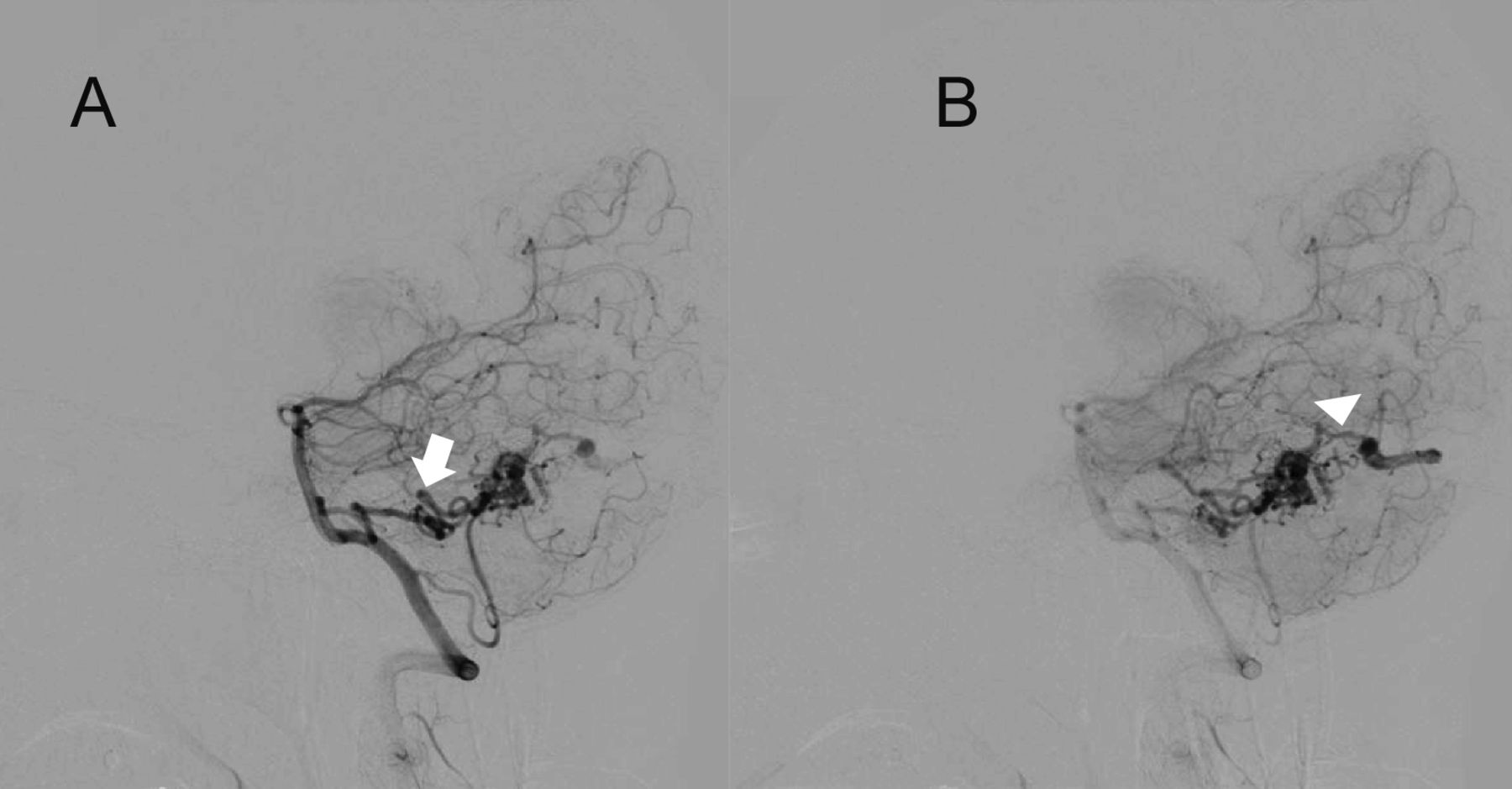
Same case. Lateral projections of a left vertebral artery injection showing obliteration of the nidus previously fed by the left superior cerebellar artery. Significant reduction in the size of the arteriovenous malformation (AVM) nidus can be appreciated. The AVM nidus is filling from the left anterior inferior cerebellar artery with significant tortuosity close to the AVM nidus (arrow in A). The draining vein with an area of stenosis past the nidus can be appreciated (arrowhead in B).

{kind=link}
{kind=link}
{kind=link}
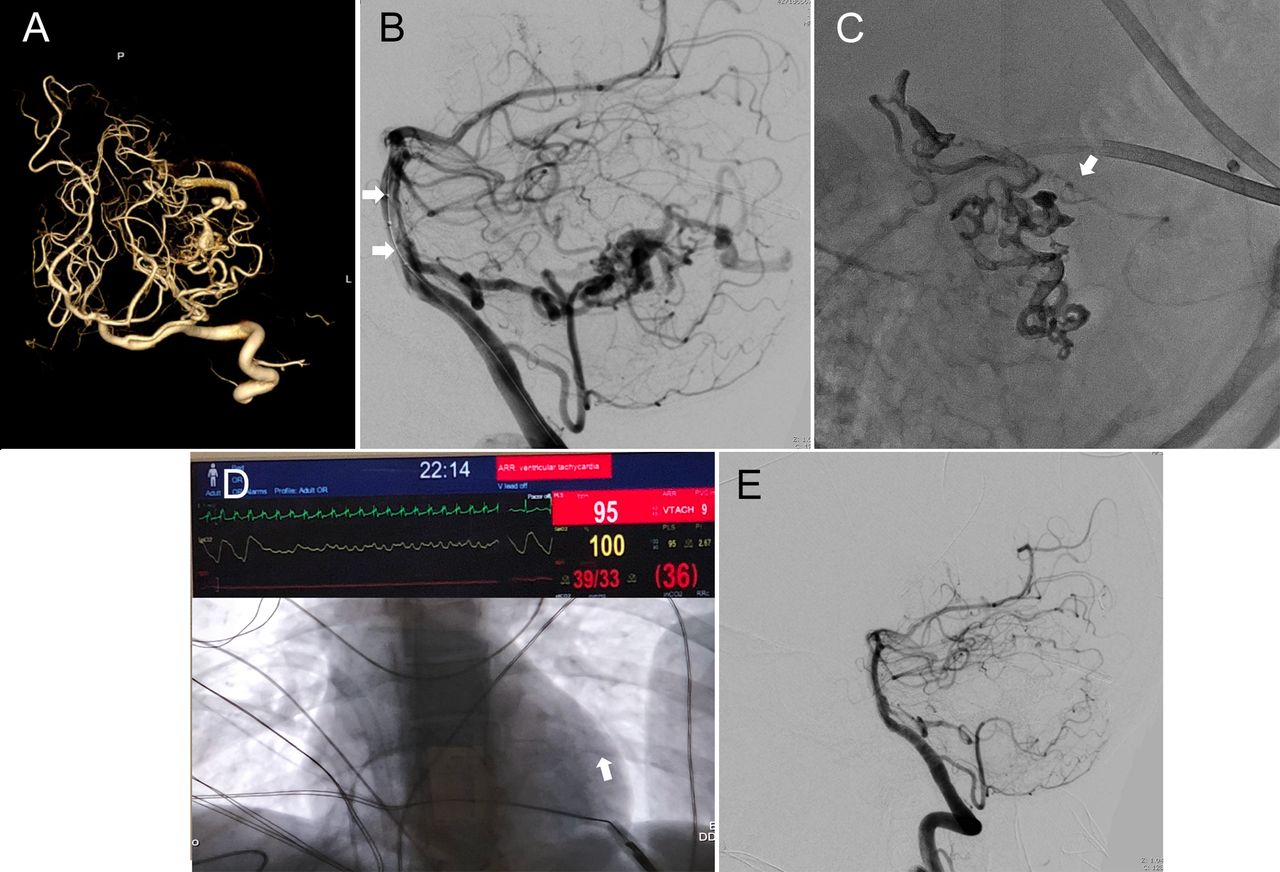
Same case. Three-dimensional reconstruction of left vertebral artery cranial spin injection showing the arteriovenous malformation (AVM) nidus (A). Lateral projection of the left vertebral artery injection showing a Scepter balloon (MicroVention-Terumo) positioned in the basilar artery (B, arrows). The microcatheter is brought into the draining vein (C, arrow). Onyx injected via transvenous catheter and transvenous pacing (D). Complete obliteration of the AVM is achieved (E).
Discussion
Transvenous embolization is curative for select AVMs.1 2 4 6 The greatest technical challenge of the procedure is selectively catheterizing the draining vein and safely penetrating the nidus with the embolizate. In this case series we demonstrate the safety and effectiveness of total flow control using concurrent arterial balloon occlusion and RVP (and IV adenosine administration) for transvenous embolization. The cardiac standstill (severe hypotension) technique has been described in vascular neurosurgery, where it has been utilized in the surgery of complex cerebral aneurysms.7 11 13 Adenosine-induced asystole, RVP, and hypothermia with circulatory arrest are methods used to achieve severe systemic hypotension. We used RVP in most of our cases. The mechanism of RVP is through the induction of ventricular tachycardia, resulting in ineffective ventricular filling. This results in reduced cardiac output and hypotension. The RVP is achieved through the placement of the bipolar pacing electrode into the right ventricle. The effect of RVP is instantaneous, efficacious, and immediately reversible. The use of RVP reduces flow from feeders that cannot be occluded with a balloon. It is important to recognize that although the heart is ineffective in filling up during RVP, the bulk anterograde flow continues. The utilization of RVP has been described previously for aneurysm clipping. In an 11 patient case series, RVP was used to help with dissection and clipping of intracranial aneurysms.11 No intraoperative rupture or surgical- or anesthesia-related complication was seen. The current case series supports the safety of RVP, as no complication related to RVP or general anesthesia was noted. Compared to RVP, adenosine-induced cardiac standstill may result in prolonged hypotension and is contraindicated in patients with asthma, chronic obstructive pulmonary disease, and coronary artery disease. No contraindications to RVP have been reported in the literature. However, the utilization of RVP is invasive and requires the assistance of an interventional cardiologist.
In one case (the first case in this series) cardiac standstill was achieved with a systemic adenosine injection. For this case, an anesthesiologist administered an 18 mg test dose of adenosine followed by 60 mg adenosine to achieve complete cardiac asystole. The remainder of the protocol was unchanged.
Perioperative hemorrhage occurred in two cases in our series. In Case 3, immediately after transvenous embolization, the patient developed an intraparenchymal hemorrhage noted on computed tomography. The patient was taken for an immediate craniotomy and excision of the AVM. Retrospective review of the procedural angiogram did not demonstrate bleeding; however, it suggested incomplete transvenous embolization of the nidus based on comparison with the pre-embolization angiogram and the Onyx cast. This highlights the importance of total obliteration of the AVM. The patient made an excellent recovery when seen in follow-up at 6 months. In Case 10, intraventricular hemorrhage was noticed during the procedure as noted above. This was managed by continued embolization using total flow control until the bleeding site was embolized. The patient was managed with a ventriculostomy and made an excellent recovery with an mRS score of 0 at 6 months. Complete obliteration was confirmed on the 6-month DSA. There was one death (Case 2) in this series. This patient died 2 months after the embolization procedure from a pulmonary embolism. The patient had initially presented with a ruptured cerebellar AVM.
To our knowledge, this is the first and the largest case series to describe total flow control using concurrent transient afferent arterial balloon occlusion and RVP for transvenous embolization of cerebral AVMs. The technique allowed safe obliteration of the nidus with a low risk of embolizate reflux. The largest case series on transvenous embolization was published by Mendes et al using temporary balloon occlusion of the arterial feeders.2 Venous access was established via the jugular vein and the microcatheter was cut at the conclusion of the procedure. We and other authors have used a similar technique.1 Mendes et al reported a complete AVM obliteration rate of 92.6% with transvenous embolization.2 Those authors reported one case of venous infarction and another of hemorrhagic complication. However, we did not observe any case of venous infarction in our series, which could be due to minimal venous reflux of Onyx. Several other authors have described the safety and feasibility of the transvenous approach.14–16 Chen et al performed a literature review that included 13 studies, yet only 69 patients.6 Those authors reviewed various technical aspects of transvenous embolization of which it is important to mention transvenous retrograde nidus sclerotherapy under controlled hypotension (TRENSH). The technique initially proposed by Massoud et al in animal and theoretical models relies on temporary systemic hypotension with or without balloon occlusion of the main arterial feeder to achieve nidal penetration of the embolizate.17–19
Systemic hypotension would not only decrease intranidal pressure to facilitate embolization but also reduce the risk of hemorrhage.17–19 Our technique has the same conceptual foundation with the goal of systemic hypotension achieved through RVP or IV adenosine in a controlled and precise fashion.
Although this is not a comparative study, we believe a combination of flow control with balloon occlusion and RVP or IV adenosine facilitates transvenous embolization by controlling the flow through large and small feeders. Several articles have elaborated on the role of proximal flow control for transvenous embolization. We view rapid ventricular pacing as a safe adjunct for transvenous AVM embolization because none of the patients in our series experienced complications associated with RVP. No patient had a cardiac event or evidence of cerebral ischemia from hypoperfusion.
Limitations of the study include the small sample size and retrospective study design from a single center. However, the study provides evidence of the safety of total flow control using transient concurrent afferent arterial balloon occlusion and RVP for AVM embolization and supports the curative value of transvenous embolization for select AVMs. Larger sample size, multicenter studies are needed to validate the findings presented in this study. Future studies should evaluate the impact of repeated RVP bursts on cognitive function, especially in asymptomatic patients.
Conclusion
Total flow control using transient concurrent afferent arterial balloon occlusion and RVP is a safe and feasible adjunct to transvenous embolization of selected AVMs.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the University at Buffalo Institutional Review Board (STUDY00003286).
Acknowledgments
The authors thank Paul H Dressel BFA for formatting the illustrations and Debra J Zimmer for editorial assistance.
References
Footnotes
Twitter @MikeTso1
Correction notice This article has been corrected since it first published. The provenance and peer review statement has been included.
Contributors Conception and design: AHS, MW. Acquisition of the data: MW, HHR, FC. Analysis and interpretation of the data: all authors. Drafting the manuscript: MW. Critically revising the manuscript: all authors. Reviewing submitted version of the manuscript: all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests KVS: Consulting and teaching for Canon Medical Systems Corporation, Penumbra Inc., Medtronic, and Jacobs Institute; Co-Founder: Neurovascular Diagnostics, Inc. JMD: Research grant: National Center for Advancing Translational Sciences of the National Institutes of Health under award number KL2TR001413 to the University at Buffalo; Consulting: Medtronic; Honoraria: Neurotrauma Science, LLC; Shareholder/ownership interests: Cerebrotech, RIST Neurovascular. EIL: Shareholder/ownership interests: NeXtGen Biologics, RAPID Medical, Claret Medical, Cognition Medical, Imperative Care (formerly the Stroke Project), Rebound Therapeutics, StimMed, Three Rivers Medical; National Principal Investigator/Steering Committees: Medtronic (merged with Covidien Neurovascular) SWIFT Prime and SWIFT Direct Trials; Honoraria: Medtronic (training and lectures); Consultant: Claret Medical, GLG Consulting, Guidepoint Global, Imperative Care, Medtronic, Rebound, StimMed; Advisory Board: Stryker (AIS Clinical Advisory Board), NeXtGen Biologics, MEDX, Cognition Medical, Endostream Medical; Site Principal Investigator: CONFIDENCE study (MicroVention), STRATIS Study—Sub I (Medtronic). AHS: Financial interest/investor/stock options/ownership: Amnis Therapeutics, Apama Medical, Blink TBI Inc., Buffalo Technology Partners Inc., Cardinal Consultants, Cerebrotech Medical Systems, Inc., Cognition Medical, Endostream Medical Ltd, Imperative Care, International Medical Distribution Partners, Neurovascular Diagnostics Inc., Q’Apel Medical Inc, Rebound Therapeutics Corp., Rist Neurovascular Inc., Serenity Medical Inc., Silk Road Medical, StimMed, Synchron, Three Rivers Medical Inc., Viseon Spine Inc.; Consultant/Advisory Board: Amnis Therapeutics, Boston Scientific, Canon Medical Systems USA Inc., Cerebrotech Medical Systems Inc., Cerenovus, Corindus Inc., Endostream Medical Ltd, Guidepoint Global Consulting, Imperative Care, Integra LifeSciences Corp., Medtronic, MicroVention, Northwest University–DSMB Chair for HEAT Trial, Penumbra, Q’Apel Medical Inc., Rapid Medical, Rebound Therapeutics Corp., Serenity Medical Inc., Silk Road Medical, StimMed, Stryker, Three Rivers Medical, Inc., VasSol, W.L. Gore & Associates; Principal Investigator/steering comment of the following trials: Cerenovus NAPA and ARISE II; Medtronic SWIFT PRIME and SWIFT DIRECT; MicroVention FRED & CONFIDENCE; MUSC POSITIVE; and Penumbra 3D Separator, COMPASS, and INVEST.
Provenance and peer review Not commissioned; externally peer reviewed.