Article Text

Abstract
Background Transvenous embolization of brain arteriovenous malformations (AVMs) can be curative. We aimed to evaluate the cure rate and safety of the transvenous retrograde pressure cooker technique (RPCT) using coils and n-butyl-2-cyanoacrylate as a venous plug.
Methods All AVM patients treated via transvenous embolization between December 2004 and February 2017 in a single center were extracted from our database. Inclusion criteria were: inability to achieve transarterial cure alone; AVM < 3 cm; and single main draining vein. Outcome measures were immediate and 90 days' angiographic AVM occlusion rate, and morbidity and mortality at 30 days and 12 months, according to the modified Rankin Scale (mRS) score.
Results Fifty-one patients (20 women; median age 47 years) were included. A majority (71%) were high grade (3 to 5 in the Spetzler–Martin classification). AVMs were deeply seated in 30 (59%) and cortical in 21 patients (41%). Thirty-three patients were previously embolized transarterially (65%). All patients but one were cured within a single session with the RPCT (96%). Cure was confirmed on follow-up digital subtraction angiography at 3 months in 82% of patients. Three patients experienced intracranial hemorrhage (6%), one requiring surgical evacuation. There were no deaths. One treatment-related major permanent deficit was observed (2.0%). Mean mRS before treatment, at 30 days, and 12 months after RPCT was 1.5, 1.5, and 1.3, respectively.
Conclusions The retrograde pressure cooker technique can be curative in carefully selected high-grade AVMs. Long-term follow-up and prospective studies are needed to confirm our results.
- arteriovenous malformation
- brain
- liquid embolic material
- vein
Data availability statement
Data are available upon reasonable request. The datasets during and/or analyzed during the current study available from the corresponding author on reasonable request.
Statistics from Altmetric.com
Introduction
Embolization of brain arteriovenous malformations (AVMs) is often used to facilitate microsurgical resection or radiosurgery.1 Stand-alone curative transarterial embolization, however, rarely exceeds 50%,2 despite the use of ethylene vinyl alcohol (EVOH) copolymers.3 4
The transarterial pressure cooker technique can improve the rate of curative embolization.5 Nonetheless, some feeders may be too tiny or tortuous to be accessed antegradely, as opposed to retrograde embolization through a transvenous approach.6
Our aim was to evaluate the safety and efficacy of the transvenous retrograde pressure cooker technique (RPCT) in AVMs considered incurable transarterially.
Methods
This cohort study complies with the STROBE (Strengthening the Reporting of Observational Study in Epidemiology) statement.7
For this retrospective study, all patients consented that their data be anonymized and generally used for future studies. Our institutional review board waived specific consent for the present study.
Study population
Our database was searched for patients who underwent transvenous embolization between December 2004 and February 2017. Baseline demographics, including age, gender, mode of presentation, and modified Rankin Scale (mRS) score before, at 30 days, and 1 year after embolization were retrieved, as well as AVM characteristics including size (mm), location (cortical or deep), side [right, left, or midline], number of outflow veins, type of drainage [superficial, deep, both], and grade8 and number of previous treatments.
The three standard criteria for a transvenous approach were: inability of transarterial cure, AVM <3 cm, and a single outflow vein.
The retrograde pressure cooker technique for transvenous embolization
Under general anesthesia and placement of a 6F or 7F arterial guiding catheter, a 1.2F Magic microcatheter (Balt Extrusion, Montmorency, France) was used to superselectively explore all feeders and understand the associated venous segmentation. A 7F-guiding catheter (Fubuki, Asahi Intecc, Amsterdam, Netherlands) was then navigated from the jugular vein to the straight or the superior sagittal sinus. An 8F guiding catheter (Guider Softip, Boston Scientific, Marlborough, MA) was used instead of a 7F whenever accessing the outflow vein of the AVM was difficult. A third additional microcatheter, either a large remodeling balloon (Copernic RC 8×80/10x80 or Eclipse 6×30, Balt Extrusion) or a Comaneci Device (Rapid Medical, Yokneam, Israel) was then placed in the sagittal sinus in order to get support when accessing the cortical outflow vein (figure 1). A retrograde micro-catheterization of the main outflow vein was then achieved with two microcatheters: a first detachable-tip microcatheter (Apollo 3 cm or 5 cm detachable tip, Medtronic, Dublin, Ireland; or Sonic 1.2 F-35, Balt Extrusion) for injection of EVOH and a second microcatheter (Apollo or Magic 1,2 F, Balt Extrusion) to create the plug. The first detachable-tip microcatheter was placed in the main outflow vein at the merging point of the primary veins. A selective 3D rotational angiography from the arterial feeder best depicting the primary veins and main outflow vein was obtained and used to determine the best roadmap view for the subsequent retrograde venous navigation.
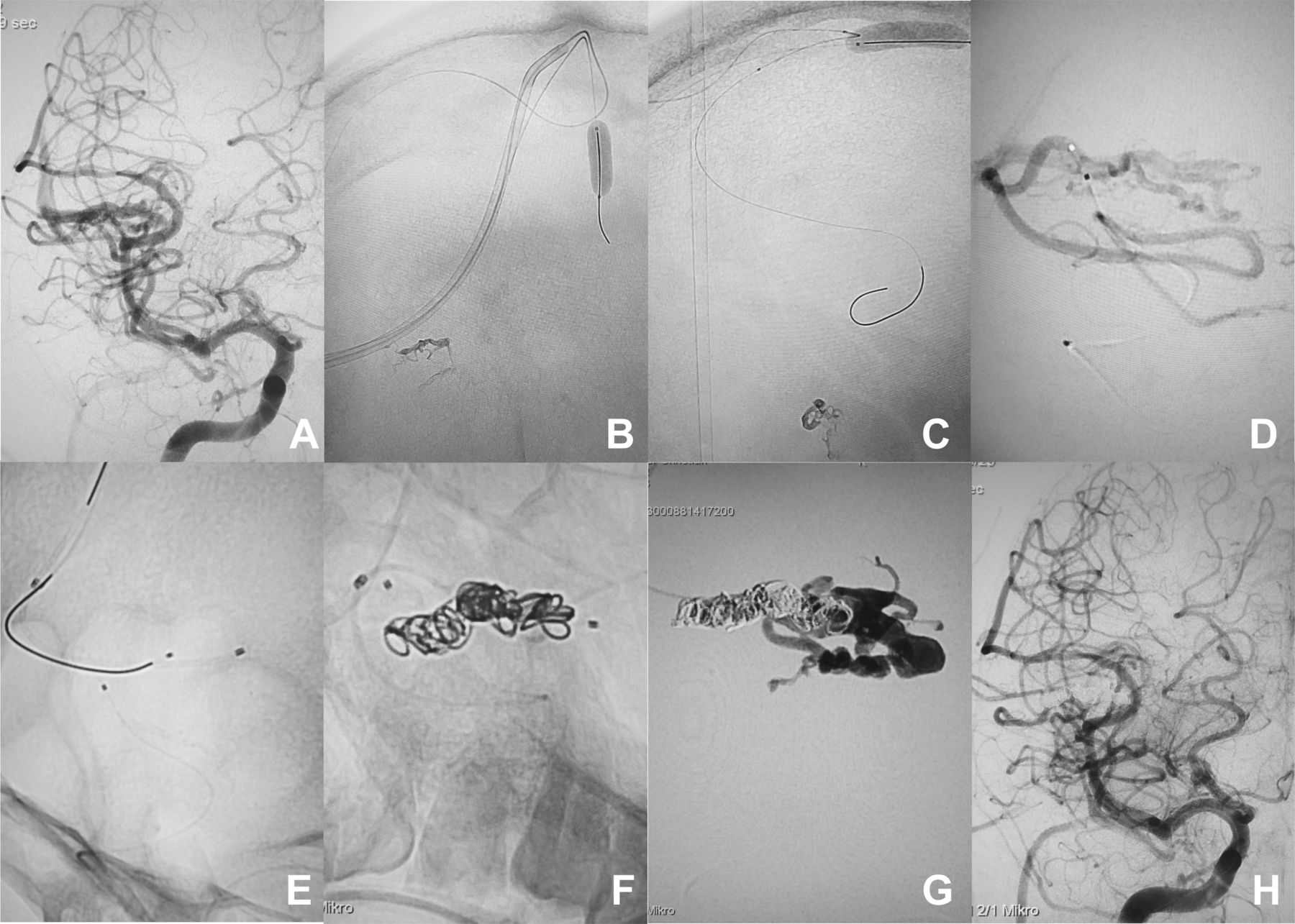
A patient with an arteriovenous malformation (AVM) who had already undergone transarterial embolization.(A) Anteroposterior (AP) view of right internal carotid angiography showing residual AVM in the right distal Sylvian fissure. (B,C) Nonsubtracted AP view (B) and lateral view (C) showing the inflated balloon in the superior sagittal sinus facilitating microcatheter retrograde entry into the cortical vein. (D) AP view of superselective angiography from arterial feeding vessel demonstrating the microangioarchitecture of the AVM. (E) Nonsubtracted AP view showing the successful navigation of the two microcatheters from the venous side, and one microcatheter from the arterial side. (F) Nonsubtracted AP view depicting the placement of coils between the tip and the detachment zone of the detachable tip microcatheter (both in the draining vein). (G) Fluoroscopic frontal image during embolization with ethylene vinyl alcohol (EVOH) copolymer. Coils with n-butyl-2-cyanoacrylate prevented excessive venous reflux of EVOH copolymer and allowed rapid diffusion into the primary veins and arterial feeder. (H) Final AP view of right internal carotid angiography showing complete obliteration of the AVM.
The second microcatheter was navigated alongside the first microcatheter according to the principle of the sheeping technique9 until its tip reached the same level. Systolic blood pressure was then reduced below 70 mmHg to diminish the outflow pressure and limit the risk of venous embolic material migration. For veins<3 mm in diameter, a 1.2F Magic microcatheter was used to deliver flow coils (SPIF Flow Coils 2.5×5–20, Balt Extrusion) along the detachment tip of the other. For larger veins, a 1.5F Apollo or Marathon microcatheter (Medtronic) was used to deliver electrically detachable coils (ED coil, Kaneka Medix Corporation, Osaka, Japan; or Barricade coils, Blockade Medical, Irvine, CA). Coiling was achieved through the second microcatheter, backwards from the tip of the first microcatheter on a 20 mm segment of length, trying to achieve the highest possible density.
EVOH copolymer (Onyx-18, Medtronic; and later Squid-12, Emboflu, Gland, Switzerland) was then injected through the first microcatheter. EVOH first diffused downstream to the coils. Injection was stopped as soon as EVOH reached the coils and repeated a few times until the flow in the vein was almost disrupted. At that stage, acrylic glue (50% n-butyl-2-cyanoacrylate – 50% Lipiodol [Guerbet, Paris, France]) was injected into the coils through the second microcatheter until a complete filling of this venous segment was achieved. After this stage, further EVOH was retrogradely injected until the whole AVM was filled. The AVM was considered cured once the final cast of embolic material matched with the pre-interventional angiographic aspect on the same working projection (figure 2). Care was taken to avoid overfilling of the AVM with excessive reflux into the normal arteries. In case of doubtful residual micro-shunts, a selective catheterization with a Magic 1.2F microcatheter was achieved to search for potential feeders with a remaining flow to the AVM, followed by transarterial embolization if needed. After removal of the detachable-tip microcatheter, a cone-beam CT was systematically performed to exclude any hemorrhagic complication. Systolic blood pressure was maintained 20 mmHg below normal pressure for 24 hours.

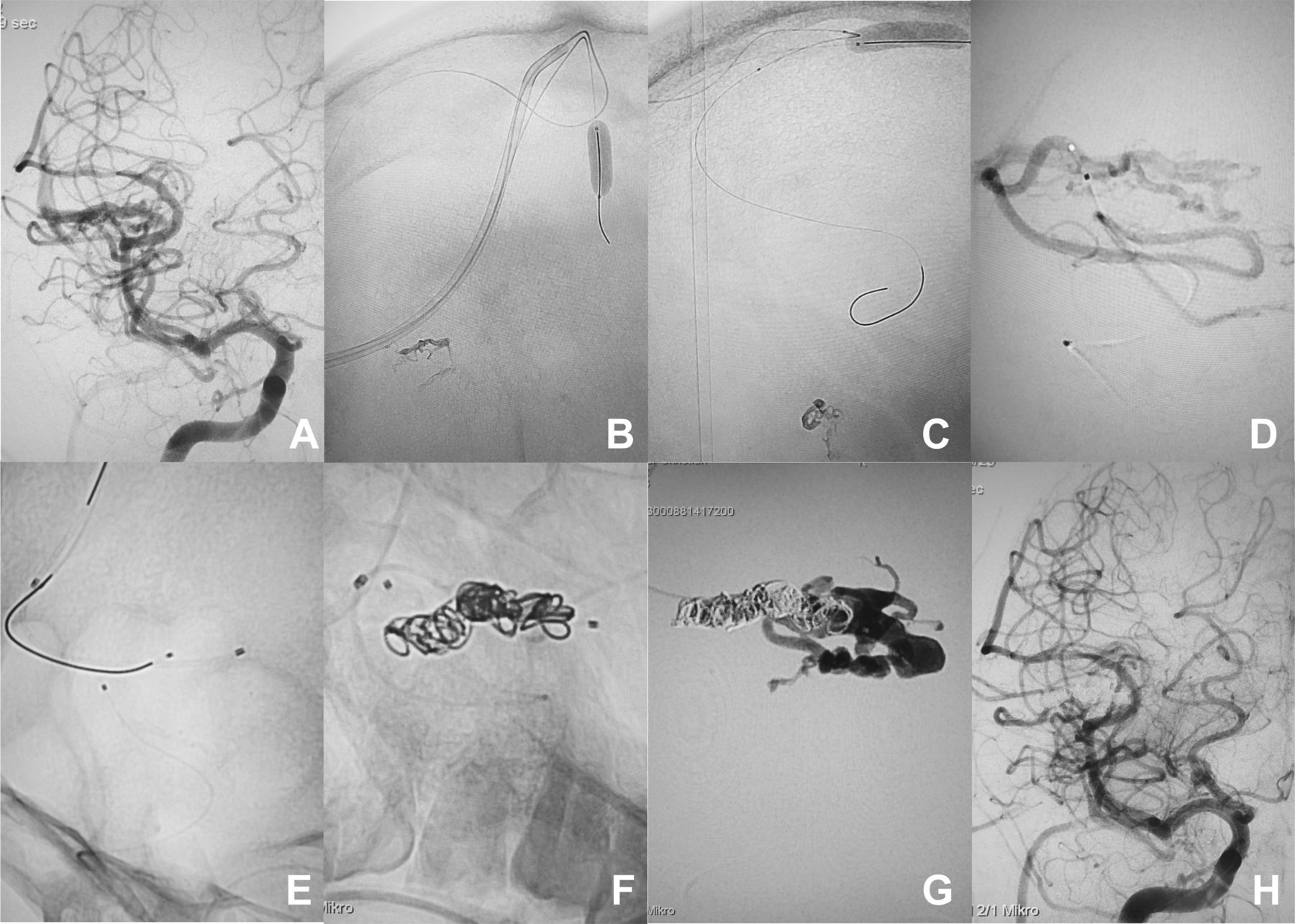
A patient with a brainstem arteriovenous malformation (AVM). (A) Lateral view of vertebral angiogram showing residual nidus in the dorsal midbrain. (B) Lateral view of superselective angiography from the arterial feeding vessel revealing the microangioarchitecture of the AVM. (C) Nonsubtracted lateral view depicting the navigation of the detachable tip microcatheter and second microcatheter from the venous side and one microcatheter from the arterial side. (D) Nonsubtracted lateral view showing the placement of coils from the microcatheter in the vein. (E) Nonsubtracted lateral view showing the cast of ethylene vinyl alcohol (EVOH) copolymer and coils. Note that the coils with n-butyl-2-cyanoacrylate prevented distal migration of EVOH copolymer and allowed retrograde embolization of the AVM. (F) Lateral view of vertebral angiography showed complete obliteration of the AVM.
Outcome assessments
To ascertain the long-term post-operative benefit and account for transient post-operative deficits due to edematous changes, the neurological status at 30 days and 12 months (modified Rankin Scale (mRS) score) were compared. Treatment-related major complications were defined as neurological deterioration resulting in a permanent worsening of more than one point of mRS score at 1 year. Complete occlusion was assessed on follow-up digital subtraction angiography (DSA) at 3–6 months.
Results
Fifty-one patients (20 women) with brain AVMs embolized with the RPCT were identified (online supplemental tables 1 and 2). Median age was 47 years (range 15–74). Most patients (82%) presented with hemorrhage before treatment. Forty-one (80%) were neurologically independent (mRS 0–2) pre-embolization. AVMs were deep-seated or cortical in 30 and 21 patients, respectively. Thirty-six (71%) were high grade and two-thirds had been previously embolized.
Supplemental material
Supplemental material
Complete obliteration was observed in 49/51 patients (96%) after a single session, including one AVM with two outflow veins where a double RPCT was used through a bilateral internal jugular vein approach (online supplemental table 3). One patient with two deep outflow veins required two separate embolizations to be cured. We failed to catheterize the main outflow vein in one left-sided mesio-temporal AVM draining into the sphenopetrosal vein, which was sent to radiosurgery. We could measure the diffusion time of Onyx in 42 cases (84%) of 50 embolized cases. The median time between venous plug formation and full AVM obliteration was 6 min (IQR: 3.25–8).
Supplemental material
Of the 30 deep-seated AVMs, 29 (97%) drained into the straight sinus. All were accessible via the basal vein of Rosenthal or internal cerebral vein. Of the 21 cortical AVMs, 18 (86%) drained into the superior sagittal sinus. Eight (44%) required balloon assistance to fully access the cortical vein. Two drained into the cavernous sinus, which was accessed via the inferior petrosal sinus to reach the main outflow vein.
Maximal length of reflux in the main outflow vein was 4 cm. No durable symptomatic post-operative venous ischemia was observed. No jugular vein thrombosis was observed.
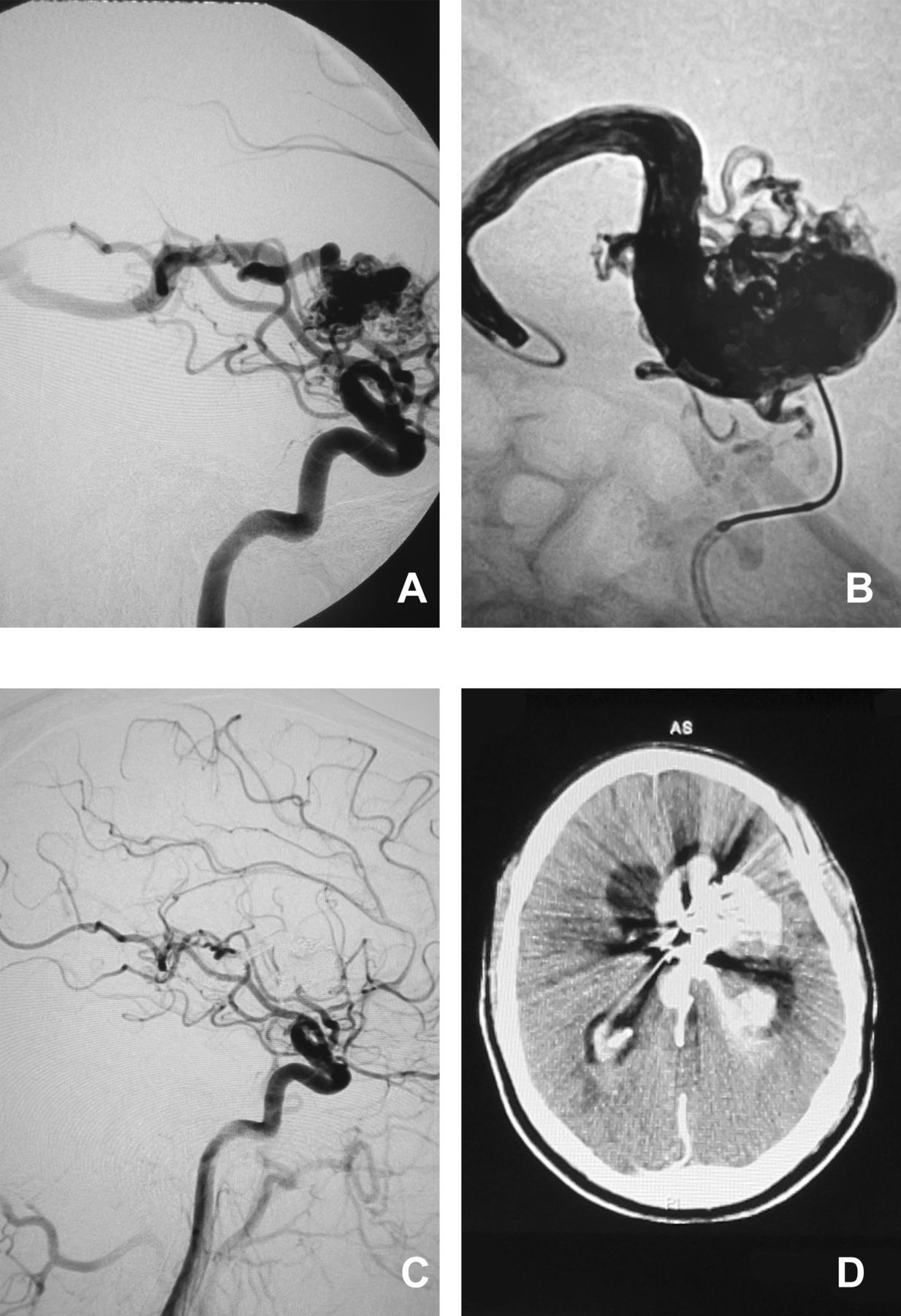
Postoperative intracranial hemorrhage occurred in three patients (5.9%). The first was a patient with a ruptured dorsal midbrain AVM that initially presented with ventricular bleeding. After an uneventful RPCT and complete exclusion, the patient developed pulmonary embolism that was anticoagulated, followed by headaches and somnolence on the following day. A CT revealed an intracerebral hematoma in the left thalamus extending to the corona radiata and ventricular system, possibly precipitated by anticoagulation. The second bleed occurred in a patient with a right-sided basal ganglial AVM who initially presented with putaminal hemorrhage and left hemiparesis. Venous perforation occurred during catheterization of a long and tortuous frontobasal vein. Nonetheless, prompt curative embolization could be achieved, including perforation site. Minimal subarachnoid contrast extravasation was observed on cone-beam CT, which remained clinically uneventful. The third happened in a hemiparetic patient with a four-time ruptured left-sided basal ganglial AVM previously treated twice by stereotactic radiosurgery. Despite an uneventful curative RPCT, a parenchymal hematoma with intraventricular extension requiring surgical evacuation developed 24 hours' later (figure 3). Recovery to his pre-operative status (mRS 4) was observed at 30 days.

A patient with a residual ganglionic arteriovenous malformation (AVM) after four episodes of hemorrhage and stereotactic radiosurgery twice previously. (A) Lateral view of internal carotid angiography demonstrates residual AVM in the left basal ganglia. (B) Nonsubtracted lateral view shows the cast of ethylene-vinyl alcohol copolymer. (C) Complete obliteration of the AVM. (D) Follow-up plain CT showing intracerebral hemorrhage in the left basal ganglia and ventricular system.
Median duration of DSA follow-up was 3 months (IQR: 3–5.3) in 40/51 (82%) patients, confirming cure in all controlled cases. Follow-up DSA remains pending in 11 patients (online supplemental table 2).
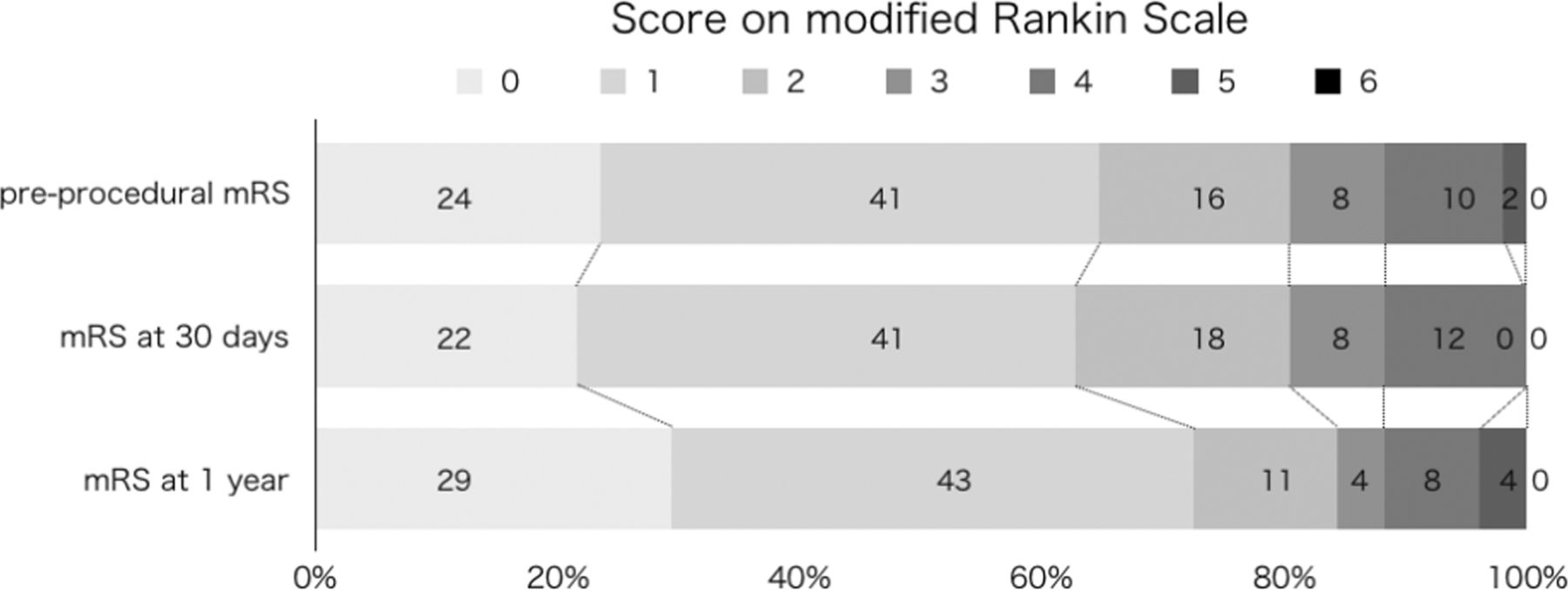
Overall, 41 (80%) patients at 30 days and 43 (84%) at 1 year had a good outcome (mRS 0–2). In 46, the neurological status remained unchanged or improved at 30 days compared with the pre-operative status (figure 4). Five experienced at least 1-point mRS worsening at 30 days. At 1 year, two improved and regained their pre-interventional condition (5.9% transient morbidity). One with a pre-mRS of 3 gradually decreased to 4 at 30 days and 5 at 1 year, despite any treatment-related ischemic or hemorrhagic changes. Clinical worsening was attributed to wasting syndrome. One with a pre-mRS of 1 increased to 2 at 30 days and 1 year and thus categorized as minor permanent morbidity. As a result, one major treatment-related complication (2%) was observed in our series. There were no deaths.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Distribution of modified Rankin Scale (mRS) scores before treatment, at 30 days, and 1 year after transvenous embolization using retrograde pressure cooker technique: 0 indicating no symptoms; 1 no clinically significant disability; 2 slight disability (patient is able to look after own affairs without assistance but is unable to carry out all previous activities); 3 moderate disability (patient requires some help but is able to walk unassisted); 4 moderately severe disability (patient is unable to attend to bodily needs without assistance and unable to walk unassisted); 5 severe disability (patient requires constant nursing care and attention); and 6 death.
Discussion
According to our findings, the RPCT appears to be highly effective, considering that 96% of AVMs could be fully occluded within a single session. These results concur with a recent systematic review of the venous approach.10 Remarkably, two-thirds were high-grade AVMs (Spetzler–Martin grade 3–5) with a low rate of permanent major neurological morbidity at 1 year (2%), despite hemorrhagic complications in approximately 6%.
The earliest description of transvenous embolization with a precipitating embolic agent dates back to 2003 during the ABC WIN seminar in Val d’Isère (France) by Dr. Houdak, followed in 2005 by Houdart and Chapot at the same meeting. A case report of our “transvenous pressure cooker technique” that we presented orally in several conferences depicts our concept schematically.11 In the past decade, transvenous Onyx embolization has only been occasionally reported.12–14 The largest series published so far in 40 surgically inoperable AVMs by the group of Dr. Mounayer convincingly demonstrated the safety and effectiveness of this technique.15 Recently, the same team reported a 95% cure rate in a series of 73 low-grade AVMs embolized transvenously.16 To explain the absence of significant bleeding and morbidity, they introduced the concept of the “Porcelain Vein”, relating to the circumferential, centripetal deposition of EVOH copolymer along the vessel wall during reflux that progressively reduces the diameter of the main venous drainage, rather than abruptly disrupting its outflow.15 We challenge this concept, however, as we would otherwise have experienced more bleeding in our RPCT series. Moreover, without a plug of coils and glue, it is more difficult to control the length of EVOH reflux in a vein exceeding 4 mm in diameter, which is why we advocate using the RPCT despite the need for multiple microcatheters instead of one. Although Iosif et al6 report that a long reflux of Onyx along the main outflow vein is safe as it only drains AVM, the security margin remains ill-defined. To our knowledge, there is no certainty that normal veins do not drain into the main outflow vein, potentially increasing the risk of venous congestion and infarction if thoroughly occluded.
Onyx-18 was used in the first patients, it was the only viscosity of EVOH that was initially available. We progressively introduced EVOH with a reduced viscosity, Squid-12 after its launch in 2014. In our experience, the lower viscosity allows a higher penetration potential but fails to form a plug. This is another advantage of the RPCT that allows to overcome this drawback by building a plug with coils and glue. The low-viscosity embolic agent can then be used which improves the chances of complete retrograde occlusion.
Our rate of hemorrhagic complications compares favorably to the 8%–11% rate associated with transarterial Onyx embolization,17 18 especially when considering the proportion of high-grade AVMs with exclusive deep drainage that have a higher propensity to bleed and are notoriously challenging to cure with radiosurgery or microsurgical resection.19 Moreover, we have observed significantly less ischemic changes on routine post-interventional magnetic resonance image controls after the RPCT compared with curative transarterial embolization.
Remarkably, no acute intra-operative AVM rupture occurred in the interval between venous occlusion and the subsequent retrograde embolization with EVOH. While rapid retrograde obliteration of the terminal arterial feeders may explain this, we believe prolonged hypotension also plays an essential role by decreasing the risk of hyperperfusion hemorrhage related to the impaired autoregulation of AVM feeders.20 Importantly, no systemic complication from induced hypotension occurred in our series. Alternative methods to reduce the pressure gradient in the AVM during embolization still need to be validated but include balloon inflation in the largest arterial feeder,21 rapid ventricular pacing. or adenosine-induced cardiac arrest.22
Transvenous navigation differs significantly from arterial catheterization, essentially because veins are more fragile, mobile, and elastic. Moreover, a 7F or 8F guiding catheter through a jugular rather than a femoral access is required to pass the tortuous sigmoid sinus junction and obtain sufficient stability to navigate two microcatheters to the main outflow vein.
In summary, the following key points are essential when considering curative transvenous embolization:
As a rule, AVM diameter should not exceed 3 cm to avoid missing terminal feeders that may be masked by a large deposition of EVOH in the primary veins and lead to delayed hemorrhage. In case of doubt, selective microcatheterization and transarterial embolization of a doubtful feeder with a drop of glue of flow coils should be encouraged.
Big AVMs have large outflow veins that tend to be easier to navigate but more challenging to occlude without refluxing excessively. Consequently, curative RPCT should be considered only after having achieved maximal transarterial down-staging in order to progressively reduce the caliber of the main outflow vein.
When multiple main outflow veins are present, betting on the retrograde diffusion of EVOH copolymer to all the shunts from one vein to the other may be hazardous. Consequently, we advise restricting the transvenous approach to AVMs expressing a single main outflow vein, unless distinct compartments with separate feeders and a dedicated draining vein can be identified and successively embolized, as achieved in two of our patients.
The deep venous system is the easiest access for a transvenous approach.6 12 Indeed, catheterization of the straight sinus, internal cerebral, or basal veins is relatively straightforward. While superficial brain AVMs may also be cured transvenously in experienced hands,23 accessing the cortical veins through the superior sagittal sinus is more challenging and often requires adjunctive techniques due to their “S-shaped” caudal angulation at the duro-pial junction. Likewise, the vein of Labbé is delicate to navigate due to its functional nature and the recurrent angulation at the junction with the transverse or sigmoid sinus. According to our experience, a contralateral approach from the opposite jugular vein through the torcular tends to be more successful. Finally, the cavernous sinus may also be considered to reach the main outflow vein of otherwise unattainable superficial AVMs, as done in two of our patients. Given the septated aspect of the cavernous sinus, however, the risk of failure is high.
A post-embolization flat-panel CT is advised to rapidly identify and manage perioperative rupture.
Our study has several limitations. Besides its single institution retrospective nature and inherent biases, we selected patients in whom we considered that complete embolization had a high chance of success, which may not be reproducible in different settings. On the other hand, 36/51 patients (71%) presented with high-grade AVMs that are notoriously challenging to resect or to irradiate. The lack of a control group and self-adjudicated results without core-laboratory evaluation of the clinical and radiological results are probably the main limitation, despite our encouraging results. Additionally, a follow-up DSA still lacks in 11 patients (18%), which may disclose unexpected results and diminish the total cure rate of the RPCT. Likewise, while postoperative recurrence is rare,24 long-term follow-up, especially in young patients, remains essential. Furthermore, while curative transvenous embolization seems possible for selected AVMs, the risk of each prior transarterial embolization needs to be accounted for during patient counseling, despite the absence of morbidity in our cohort.
Conclusion
The transvenous retrograde pressure cooker technique can be curative in a single session in well-selected high-grade brain AVMs. The risk of hemorrhage seems to be acceptable with good odds of a clinically favorable outcome. Longer follow-up and case-controlled studies are required to validate our findings.
Data availability statement
Data are available upon reasonable request. The datasets during and/or analyzed during the current study available from the corresponding author on reasonable request.
Ethics statements
References
Footnotes
MK and PJM contributed equally.
Contributors Study design: MK, PJM, CPS, RC. Data acquisition: MK, PJM, HN, MH, JK, APN, AES, CPS, RC. Data analysis and interpretation: MK, PJM, CPS, RC. Manuscript preparation: MK, PJM, CPS, RC. Revision of manuscript for important intellectual content: MK, PJM, CPS, RC. Approval of the final version of the manuscript: all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.