Article Text

Abstract
Objective To understand how three commonly used measures of endovascular therapy correlate with clinical outcome and infarct growth.
Methods Prospectively enrolled patients underwent baseline MRI and started endovascular therapy within 12 h of stroke onset. The final angiogram was given a primary arterial occlusive lesion (AOL) recanalization score (0–3), a Thrombolysis in Myocardial Infarction (TIMI) score (0–3) and a Thrombolysis in Cerebral Infarction (TICI) score (0–3). The scores were dichotomized into poor revascularization (AOL 0–2, TIMI 0–1 and TICI 0–2a) versus good revascularization (AOL 3, TIMI 2–3, TICI 2b–3). Patients were classified according to whether or not they had target mismatch (TMM). Good outcome was defined as a 90-day modified Rankin Scale score of 0–2.
Results Endovascular treatment was attempted in 100. A good outcome was achieved in 57% of patients with a TICI score of 2b–3 and in 24% of patients with a TICI score of 0–2a (p=0.001). Patients with TIMI scores of 2–3 and an AOL score of 3 had lower rates of good outcome (44% and 47%, respectively), which were not significantly better than those with TIMI scores of 0–1 or AOL scores of 0–2. In patients with TMM, these rates of good outcome improved with all the scoring systems and were significantly better for TIMI and TICI scores. Patients with a TICI score of 2a had rates of good functional outcome and lesion growth which were not different from those with TICI scores of 0–1 but were significantly worse than those with TICI scores of 2b–3.
Conclusions TIMI 2–3 and TICI 2b–3 reperfusion scores demonstrated improved outcome in patients with tissue mismatch with a small infarct core and a larger hypoperfused region but AOL scores did not. Patients with a TICI score of 2a had a poorer outcome and more lesion growth than those with TICI scores of 2b–3.
- Angiography
- Intervention
- MRI
- Stroke
Statistics from Altmetric.com
Introduction
Trials evaluating the success of endovascular therapy have relied on a variety of angiographic grading scales to measure how well an ischemic vascular bed responds to treatment. Some of these scales use recanalization of the affected artery and some use reperfusion of the ischemic territory supplied by the artery in question.1–7 The use of multiple scales has resulted in some controversy because the variability in measurements is not easily translated from one study to another.8–11 In addition, studies may define the grades of the same scale in different ways.8 ,11 Ultimately, standardizing the system for reporting results would help to allow more direct comparison between studies and endovascular treatment methods. Understanding how these scales may affect outcome measures would be important to this process.
The DEFUSE 2 study is a prospective study of patients with acute ischemic stroke treated within 12 h of symptom onset with endovascular therapy. The primary clinical results of the study have recently been published.12 In order to be included in the study, patients underwent MRI within 90 min of the start of endovascular treatment and, using predefined MRI parameters, it was hypothesized that patients with a favorable MR pattern would benefit from endovascular therapy. This post hoc analysis of the angiographic data was designed to evaluate how three scales used to measure the success of endovascular treatment correlate with clinical outcome and observed infarct growth following treatment. These three scales, which have been previously described, are the Thrombolysis in Cerebral Infarction (TICI) score, the primary Arterial Occlusive Lesion (AOL) recanalization score and the Thrombolysis in Myocardial Infarction (TIMI) score.
Methods
The DEFUSE 2 study enrolled patients with acute anterior circulation stroke treated with endovascular therapy which was initiated within 12 h of symptom onset. At the outset, patients underwent MRI and were eligible for enrollment if they had a large vessel occlusion. Multicenter enrollment occurred from July 2008 to September 2011.12 Approval for the study enrollment was provided at each center's Institutional Review Board.
Imaging
Head MRI was performed on 1.5 or 3.0 T MR systems using a previously described imaging protocol. Image reconstruction was done offline using a computer system which generated quantitative diffusion-weighted imaging (DWI) and perfusion-weighted imaging (PWI) lesion maps (RAPID).13 Following endovascular therapy, an early follow-up scan with the same sequences as those used in the baseline study was obtained within 12 h of the procedure. An additional MRI study was obtained at discharge or on day 5 and included a fluid-attenuated inversion recovery (FLAIR) sequence which was used to determine infarct volume.
The automated maps generated by the RAPID system included a measure of the ischemic core volume. This volume measured regions of apparent diffusion coefficient thresholds of <600×10−6 mm2/s. A PWI volume map was used to determine the amount of hypoperfused tissue based on the time to the maximum tissue residue function (Tmax) threshold of >6 s. Target mismatch (TMM) was predefined as a ratio between the hypoperfused tissue and ischemic core of ≥1.8, with an absolute difference of ≥15 mL. In addition, patients with a TMM profile also had to have an ischemic core volume of ≤70 mL and the volume of tissue with more severe hypoperfusion (Tmax > 10 s) had to be ≤100 mL.
Endovascular treatment
Intervention was started within 12 h of the onset of ictus and within 90 min of completion of the baseline MRI study. Local sites were encouraged to use FDA-approved devices for thrombectomy which included the Concentric Merci Retriever and the Penumbra Suction Thrombectomy catheter; however, no device or technique was mandated. In addition, sites were encouraged to minimize the use of intra-arterial tissue plasminogen activator (tPA). If no prior tPA had been used, centers were encouraged to use less than a maximum of 25 mg intra-arterial tPA. If patients had received prior intravenous tPA, centers were encouraged to use ≤5 mg intra-arterially.
Imaging evaluation
All MRI and cerebral angiography studies were evaluated by a core imaging laboratory blinded to clinical data. Infarct growth was defined as the difference between the 5-day FLAIR infarct volume and the baseline DWI lesion volume. A single reader (MPM) evaluated the baseline angiogram prior to treatment to identify the primary AOL recanalization score and also assigned a pretreatment TICI score. The final post-treatment angiogram was evaluated by the same reader for reperfusion and recanalization scores using previously described measures for TIMI scores,14 TICI scores15 and AOL recanalization scores.1 The TICI score was modified from the original definition with 2a defined as partial reperfusion of ≤50% of the vascular territory of the occluded artery and 2b as partial reperfusion of >50% of the occluded artery.5 These scores are summarized in tables 1⇓–3. Post-treatment TICI scores and AOL recanalization scores were evaluated at the same time and a subsequent blinded evaluation was performed to assign post-treatment TIMI scores.
Thrombolysis In Myocardial Infarction (TIMI) scale
Thrombolysis In Cerebral Infarction (TICI) scale
Arterial occlusive lesion (AOL) scale
A dichotomous analysis was performed comparing poor revascularization scores (AOL 0–2, TIMI 0–1, TICI 0–2a) with good revascularization scores (AOL 3, TIMI 2–3, TICI 2b–3). TICI 2b–3 reperfusion was chosen as a prespecified endpoint to indicate that there had been successful early reperfusion as it correlated with the MR definition of early reperfusion.12
Statistical analysis
We compared rates of good outcome between groups using the Fisher exact test. The Cohran–Armitage test was used to evaluate trends in the rates of good outcome with increasing recanalization or reperfusion scores. Lesion growth between dichotomized groups was analyzed with the Mann–Whitney U test. All tests were two-tailed and considered significant at the α<0.05 level. Statistical analysis was performed using SAS V.9.3 (SAS Institute, Cary, North Carolina, USA).
Results
One hundred patients (49 men) of mean age 65±16 years attended the catheterization laboratory for endovascular therapy and treatment was attempted. The median time from symptom onset to femoral puncture was 5.8 h (IQR 4.5–7.8). Ten additional patients attended the catheterization laboratory but treatment was not attempted because the interventionalist decided it was not necessary after performing a diagnostic angiogram (four patients with no angiographic lesion and six patients with a more distal lesion (M2, M3 or M4 branches)). Two patients were included in the group of patients with attempted treatment because the interventionalist intended to treat them but it was decided after starting the angiogram that they could not proceed (one patient with a difficult femoral artery access with bleeding and the second patient with a carotid occlusion just distal to the aortic arch which the interventionalist felt could not be opened safely).
Table 4 shows the distribution of primary AOLs and endovascular therapies employed in the 100 patients with attempted treatment. Mismatch profiles were available for 94 patients (in six patients the baseline PWI was technically inadequate), with 75 showing a TMM profile and 19 with no TMM. Eighty-seven patients had a 5-day follow-up MRI to calculate lesion growth.
Vessel occlusion and therapy
The pretreatment angiogram demonstrated TICI 0–1 flow of the primary occlusive lesion in 87 patients (87%) and TICI 2a,b flow in 13 (13%). Following treatment or attempted treatment, 23% remained TICI 0–1, 31% were TICI 2a, 28% TICI 2b and 18% were TICI 3. The distributions of the TIMI scores after treatment were: 22% TIMI 0–1, 58% TIMI 2 and 20% TIMI 3. The AOL recanalization scores after treatment were: 24% AOL 0–1, 17% AOL 2 and 59% AOL 3. The patient with femoral access complications and the patient with very proximal carotid occlusion were scored as TICI 0–1, TIMI 0–1 and AOL 0–1, and the scoring for these two patients relied on MR angiographic studies performed shortly after the attempted procedure.
Figure 1 shows the 90-day modified Rankin scores 0–2 for the individual recanalization and reperfusion scores in the entire group of 100 patients and for the patients in each group. There was a strong trend for higher rates of good outcome with an increase in AOL score (p=0.052). The rate of good outcome was found to increase with a better TIMI score (p=0.023) and TICI score (p=0.008). Of note, patients with TICI 2a reperfusion had outcomes that were similar to those with TICI scores 0–1.

Rates of good functional outcome for individual recanalization and reperfusion scores. AOL, arterial occlusive lesion; mRS, modified Rankin Scale; TICI, Thrombolysis in Cerebral Infarction; TIMI, Thrombolysis in Myocardial Infarction.
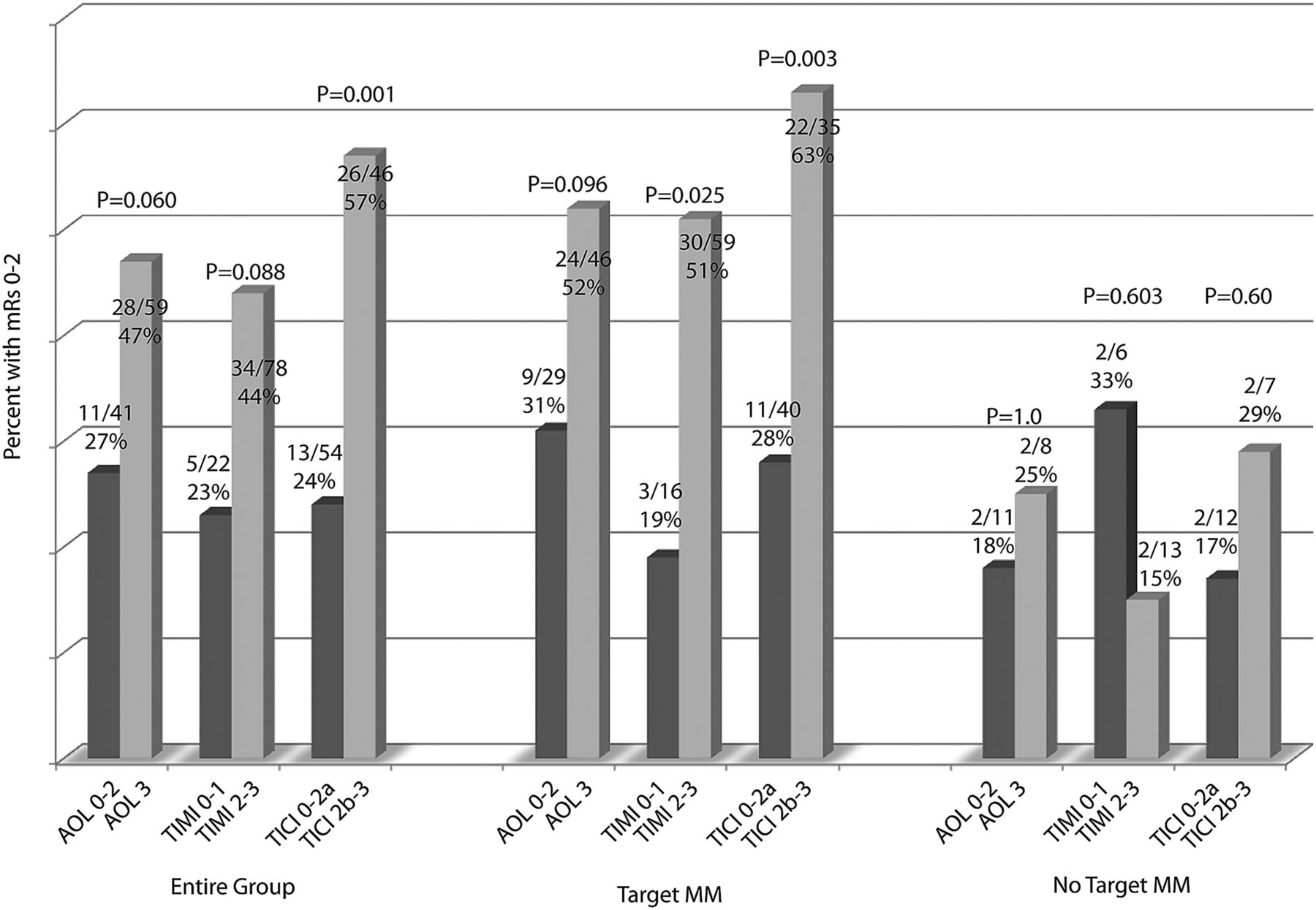
Figure 2 demonstrates the rates of good outcome for patients using a dichotomous analysis for the different scoring systems. It compares the AOL recanalization scores 0–2 with AOL 3, TIMI 0–1 with TIMI 2–3 and TICI 0–2a with TICI 2b–3 scores for the entire group of patients and for those stratified by TMM and no TMM profiles. There was a trend to higher rates of good outcome for patients with AOL 3 scores compared with AOL 0–2 scores in the entire group (p=0.06). In patients with TMM, more patients with AOL 3 had a good outcome those with AOL scores of 0–2, but these differences were not significant (p=0.096). The differences were not significant between patients with TIMI 2–3 and those with TIMI 0–1 scores for the entire group (p=0.088) but, in the TMM group, patients with TIMI 2–3 had a better outcome (p=0.025). Patients with TICI 2b–3 scores did better than those with TICI 0–2a scores in the entire group (p=0.001) and in the TMM group (p=0.003).
{kind=link}
{kind=link}
Rates of good functional outcome in dichotomous analysis of recanalization and reperfusion scores. AOL, arterial occlusive lesion; mRS, modified Rankin Scale; TICI, Thrombolysis in Cerebral Infarction; TIMI, Thrombolysis in Myocardial Infarction.
Table 5 demonstrates the infarct growth seen in patients as it correlated with the scoring systems. All the scoring systems showed that higher scores had lower rates of infarct growth, with significant differences seen in the dichotomous analysis of the AOL, TIMI and TICI scores. A separate analysis comparing median (IQR) lesion growth for TICI 0–1 scores (74 (47–127) mL) and TICI 2a score (89 (21–178 mL) showed no difference (p=0.7), while there was a difference in lesion growth between TICI 2a and TICI 2b–3 scores (23(6–69 mL; p=0.003).
Lesion growth
Discussion
This study evaluated three commonly used measures of revascularization following endovascular therapy for acute ischemic stroke. When the AOL recanalization scores were analyzed in a dichotomous fashion, a difference was seen between good (AOL 3) and poor (AOL 0–2) recanalization (p=0.06) but, in patients with TMM, those with an AOL score of 3 did not differ significantly from patients with AOL scores of 0–2. The dichotomous analysis showed that outcomes were not better for patients with TIMI 2–3 scores in the entire group (p=0.088) but, when patients with TMM were evaluated, the outcome in patients with TIMI scores of 2–3 were improved (p=0.025). Improved 90-day outcome rates were seen in patients with TICI scores of 2b–3 in the entire study group (p=0.001), and patients in the TMM group with TICI 2b–3 reperfusion also did better at 90 days (p=0.003).
These findings show that higher degrees of reperfusion appear to correlate with a greater likelihood of having a good outcome. Using the modified TICI score system, we found that the good outcome rates in patients with TICI 2a and those with TICI 1 were similar (26% and 25%, respectively), and that the good outcome rate in patients with TICI 2b (61%) showed a real improvement. This suggests that there may be a threshold for reperfusion which translates into a higher rate of good functional outcome. The TIMI scoring system does not distinguish these degrees of partial reperfusion, combining partial reperfusion into a single grade.
The AOL recanalization score is a measure of recanalization and is probably correlated to some degree with the reperfusion scores because recanalization of the primary AOL is usually a prerequisite to establishing reperfusion. However, recanalization of the primary arterial lesion does not guarantee that that there will be full reperfusion of the downstream vascular bed because there may be additional downstream occlusion that is not accounted for in the recanalization score.8 This may explain our finding that the recanalization score did not definitely correlate with good functional outcome, particularly in patients with TMM.
Our results for good outcome are similar to the recently reported Interventional Management of Stroke (IMS) III trial.16 In the patients treated with endovascular therapy there was a correlation between TICI scores and good outcome (p<0.001). In the IMS III trial, 27.6% of patients with TICI 1, 34.3% of those with TICI 2a, 47.9% of those with TICI 2b and 71.4% of patients with TICI 3 had a good outcome. Another recently reported randomized trial which did not show a benefit for endovascular therapy (MR RESCUE) used TICI 2a–3 reperfusion as a measure of successful reperfusion.17 In this study, 67% of patients had ‘successful’ reperfusion with at least TICI 2a scores. However, only 27% showed TICI 2b–3 reperfusion, although it should be noted that the definition of TICI 2b used in this trial was more than two-thirds of the territory in question.
There was a wide variation and an overlap in the amount of infarct growth seen with the AOL, TIMI and TICI scoring systems. However, the amount of infarct growth was significantly different between the groups using a dichotomous analysis for all the scores. We also saw that infarct growth was not significantly different between TICI 0–1 and TICI 2a reperfusion but was significantly lower comparing TICI 2b-3 with TICI 2a reperfusion. This decrease in infarct growth with better reperfusion also suggests that there may be a threshold of reperfusion needed to obtain an improvement in clinical outcome.
The initial description of the TICI scoring system defined a score of TICI 2b as more than two-thirds of the territory being reperfused,15 which was subsequently modified to more than one-half.5 This modified definition was used in our evaluation because it most closely matched our prespecified endpoint for reperfusion measured in follow-up perfusion studies where the deficit volume decreased by >50%.12 A recent review of how the TICI score has been defined in various studies points out that there is tremendous variability in the definitions used for the different TICI score categories.18 A recent single-center retrospective comparison of patients undergoing endovascular therapy showed that use of TICI 2b > 50% rather than >66% included about 20% more patients in the TICI 2b category.19 In addition, the study found that using >50% for TICI 2b reperfusion (as opposed to >66%) was more likely to identify patients in the TICI 2b–3 category with a good outcome. A recently reported analysis of 308 patients undergoing endovascular therapy also found that TICI 2b–3 reperfusion where >50% reperfusion was used for the definition of TICI 2b flow had the greatest sensitivity for predicting a good outcome at 90 days.20 These types of results have prompted investigators to call for the use of this threshold for defining adequate reperfusion.21 ,22
In conclusion, we found that patients with TMM with TIMI 2–3 and TICI 2b–3 reperfusion had significantly higher rates of good functional outcome than those with TIMI 0–1 and TICI 0–2a reperfusion, respectively. However, TICI 2a reperfusion was similar to TICI 0–1 in the rates of good functional outcome. Outcome was not significantly improved in patients with TMM with AOL 3 recanalization compared with those with AOL 0–2 recanalization. Median lesion growth was also found to be reduced in patients with good reperfusion or recanalization scores.
References
Footnotes
-
Funding The National Institute for Neurological Disorders and Stroke (NINDS) R01 NS03932505.
-
Competing interests MPM, MGL and MM have received grants from the National Institutes of Health. GZ has received grants from GE Healthcare and the National Institutes of Health. RB has equity interest in iSchemaView and has received grants from the National Institutes of Health. GWA has received grants from NINDS, personal fees from Covidien, Codman and Concentric, has equity interest in iSchemaView and has a patent for the RAPID software pending.
-
Contributors All the named authors contributed to conception and design or analysis and interpretation of data; drafting the article or revising it critically for important intellectual content; and final approval of the version to be published.
-
Ethics approval Ethics approval was obtained from Stanford University Institutional Review Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.