Article Text

Abstract
Background and purpose Variability in response to clopidogrel therapy is increasingly being recognized as an important factor in thromboembolic and hemorrhagic complications encountered after neurointerventional procedures. This study aims to determine the variability in response to clopidogrel therapy and associated complications in patients undergoing endovascular treatment of unruptured cerebral aneurysms.
Methods We recorded baseline patient characteristics, co-administered medications, P2Y12 reaction units (PRU) values with VerifyNow, clopidogrel dosing, and thromboembolic and hemorrhagic complications in patients undergoing endovascular treatment of unruptured cerebral aneurysms at our institution during a 19 month period.
Results 100 patients were included in the study, 76 women and 24 men, mean age 57.3 years. 15 patients exhibited an initial clopidogrel hypo-response (PRU >240) and 21 patients an initial clopidogrel hyper-response (PRU <60). 36 patients had a follow-up VerifyNow test performed without changes to the standard 75 mg daily clopidogrel dose, which demonstrated that 59% of patients who had initially been within the target 60–240 PRU range exhibited a delayed conversion to clopidogrel hyper-response. In our cohort, a clopidogrel hypo-response was associated with a significantly increased risk of thromboembolic complications in patients undergoing cerebral aneurysm treatment with stent assistance or the pipeline embolization device (60%, p=0.003), while a clopidogrel hyper-response was associated with a significantly increased risk of major hemorrhagic complications in all patients undergoing endovascular treatment of cerebral aneurysms (11%, p=0.016).
Conclusions We found wide and dynamic variability in response to clopidogrel therapy in patients undergoing endovascular treatment of unruptured cerebral aneurysms, which was significantly associated with thromboembolic and major hemorrhagic complications in our cohort.
- Aneurysm
- Platelets
- Stroke
- Flow Diverter
- Hemorrhage
Statistics from Altmetric.com
Introduction
The increasing number of devices used for the endovascular treatment of cerebral aneurysms requiring implantation within the parent artery's lumen has led to a considerable increase in the use of potent antiplatelet medications by neurointerventionalists in order to prevent parent artery thrombosis as the device endothelializes. However, despite the routine use of dual antiplatelet therapy prior to these neurointerventional procedures, usually consisting of aspirin and clopidogrel, thromboembolic complications continue to be encountered, and major hemorrhagic complications such as intraparenchymal cerebral hemorrhage (ICH) are being reported with increasing frequency, particularly following treatment with flow diverters.
A growing body of neurointerventional literature is indicating that variability in patient response to the standard 75 mg daily clopidogrel dose may be associated with some of the thromboembolic and hemorrhagic complications encountered after neurointerventional procedures, such as stenting for extracranial and intracranial atherosclerosis, stent assisted coil embolization for treatment of cerebral aneurysms, and endovascular treatment of cerebral aneurysms with the pipeline embolization device (PED).1–8
Clopidogrel causes irreversible inhibition of the P2Y12 receptor, which plays a central role in platelet activation and aggregation. VerifyNow (Accumetrics, San Diego, California, USA) is a platelet function test that measures the degree of P2Y12 receptor inhibition after stimulation with adenoside diphosphate, a P2Y12 receptor agonist. This assay has been found to correlate strongly with light transmittance aggregometry, the gold standard for quantification of platelet reactivity, in patients treated with clopidogrel, prasugrel, or ticagrelor.9–12 VerifyNow results are reported in P2Y12 reaction units (PRU), with (1) a lower PRU value corresponding to a higher degree of P2Y12 receptor inhibition and, hence, a decreased likelihood of platelet activation and aggregation, and (2) a higher PRU value corresponding to a lower degree of P2Y12 receptor inhibition and, hence, an increased likelihood of platelet activation and aggregation.
Based on the results of the Assessment of Dual Anti-Platelet Therapy with Drug Eluting Stents (ADAPT-DES) registry,13 an ‘optimal’ clopidogrel therapeutic window of 95–207 PRU that minimizes both ischemic and hemorrhagic complications after coronary artery stenting has been proposed, and this therapeutic window has recently received the CE marking of approval in Europe. In addition, a recent retrospective cohort study of 44 patients undergoing treatment of cerebral aneurysms with the PED has proposed an ‘acceptable’ clopidogrel therapeutic window of 60–240 PRU that could potentially minimize both thromboembolic and hemorrhagic complications after PED procedures.7 ,8 However, the existence of an ‘optimal’ or ‘acceptable’ clopidogrel therapeutic window in patients undergoing neurointerventional procedures has not been validated.
The aim of this study was to determine the extent of variability in initial patient response to the standard 75 mg daily clopidogrel dose, the frequency of ‘delayed conversion’ to clopidogrel hyper-response, and associated thromboembolic and hemorrhagic complications in a cohort of patients undergoing endovascular treatment of unruptured cerebral aneurysms.
Methods
Our study was approved by our hospital's institutional review board and conducted in compliance with the Health Insurance Portability and Accountability Act. We conducted a retrospective analysis to examine the response to clopidogrel therapy, and associated thromboembolic and hemorrhagic complications in patients who were started on clopidogrel for endovascular treatment of unruptured cerebral aneurysms at our institution from November 15, 2011 until June 13, 2013.
Medical record review
We recorded baseline patient characteristics and laboratory values, clopidogrel dosing schedule, P2Y12 receptor inhibition with the VerifyNow test (in PRUs) in the initial and follow-up tests, co-administration of medications that could interfere with the metabolism of clopidogrel, as well as thromboembolic and hemorrhagic complications occurring after the procedure.
Thromboembolic complications were considered major if they led to a permanent disabling neurological deficit or death. Hemorrhagic complications were considered major if they consisted of any type of intracranial hemorrhage or if the bleeding led to the patient's death.
Clopidogrel dosing protocol
Clopidogrel therapy was started 7–10 days before the procedure with the standard 75 mg daily clopidogrel dose, and the initial clopidogrel response was assessed the day before the procedure with the VerifyNow assay. For the majority of the study period, the target P2Y12 receptor inhibition was 60–240 PRUs, with PRU <60 considered a clopidogrel hyper-response and PRU >240 considered a clopidogrel hypo-response. During the initial part of the study period, clopidogrel hypo-responders were switched to prasugrel, while for the latter part of the study period, the clopidogrel dose was increased to 150 mg daily for clopidogrel hypo-responders. Clopidogrel hyper-responders were placed on every other day, every third day, every Monday and Friday, every fourth day, every fifth day, or every seventh day dosing regimens as needed to reach the target 60–240 PRU range.
Patients who underwent simple or balloon assisted coil embolization of the target aneurysm were maintained on clopidogrel therapy for 1 month after the procedure without performing routine follow-up VerifyNow testing. Patients who underwent stent assisted coil embolization of the target aneurysm were maintained on clopidogrel therapy for 2–3 months after the procedure. Patients who underwent treatment of the target aneurysm with the PED were maintained on clopidogrel therapy for 5–9 months after the procedure. The latter two patient groups underwent a routine follow-up VerifyNow test 30–40 days after initiation of clopidogrel therapy if no changes to the standard clopidogrel dose had been made. In addition, follow-up VerifyNow testing was performed 7–10 days and 30–40 days after any clopidogrel dose adjustment or after changes to medications that could affect clopidogrel metabolism. Follow-up VerifyNow testing was also performed at any time if the patient became symptomatic with abnormal bruising/bleeding or new focal neurological deficits. Of note, no specific timing between the time of the VerifyNow test and the time of the last clopidogrel dose was pursued.
Statistical analysis
Statistical analysis was performed utilizing the MedCalc V.11.1 software package (MedCalc Software, Mariakerke, Belgium). First, we performed univariate analysis with the χ2 or Fisher's exact test for each variable to identify the predictors of a hyper- and hypo-response to clopidogrel therapy in our cohort. Then we performed multivariate logistic regression analysis to identify the independent predictors of a hyper- and hypo-response to clopidogrel therapy in our cohort. A p value ≤0.05 was considered statistically significant.
Results
From November 15, 2011 until June 13, 2013, 159 patients underwent endovascular treatment of an unruptured cerebral aneurysm at our institution. Of these, 100 patients were started on a standard 75 mg daily clopidogrel dose 7–10 days before the endovascular aneurysm treatment, and the initial response to clopidogrel therapy was assessed with the VerifyNow assay (62.9%), comprising this study's cohort.
Seventy-six patients were women and 24 were men. Mean age was 57.1 years (median 59 years, range 25–82 years). Forty-three patients underwent cerebral aneurysm treatment with the PED, 40 patients underwent simple or balloon assisted aneurysm coiling, and 18 patients underwent stent assisted aneurysm coiling (one patient underwent both stent assisted aneurysm coiling and a PED procedure). Thirty-three patients were active smokers, 61 had a history of hypertension, and eight had a history of diabetes mellitus. Thirty-two patients were taking a statin, 22 a proton pump inhibitor, and 17 a selective serotonin reuptake inhibitor.
Initial response to the standard 75 mg daily clopidogrel dose
Figure 1 illustrates the distribution of the initial response to the standard 75 mg daily clopidogrel dose in our cohort. Mean number of daily 75 mg clopidogrel doses before the initial VerifyNow test was 8.5 (median 9 doses, range 5–15 doses). Mean PRU value in the initial VerifyNow test was 136.5 (median 126.5 PRU, range 0–399 PRU). Utilizing 95–207 PRU as an ‘optimal’ target PRU range, 40 patients would have been considered clopidogrel hyper-responders (PRU <95) and 26 would have been considered clopidogrel hypo-responders (PRU >207). Utilizing 60–240 PRU as an ‘acceptable’ target PRU range, 21 patients were considered clopidogrel hyper-responders (PRU <60) and 15 were considered clopidogrel hypo-responders (PRU >240).

Patient response to the standard 75 mg daily clopidogrel dose in the initial VerifyNow test (mean 8.5 doses).
Overall, in the initial VerifyNow test, a significantly higher proportion of patients were outside the ‘optimal’ target range of 95–207 PRU (66%) compared with the ‘acceptable’ target range of 60–240 PRU (36%, p <0.0001). Using a PRU <60 cut-off, there was a trend towards a higher likelihood of an initial clopidogrel hyper-response in women (25%) compared with men (8.3%, p=0.08). Nevertheless, using a PRU >240 cut-off, there was no significant difference in the likelihood of a clopidogrel hypo-response between women (14.5%) and men (16.7%, p=0.5).
Delayed conversion to hyper-response to the standard 75 mg daily clopidogrel dose
Among the 60 patients who underwent aneurysm treatment with the PED and/or stent assistance, 32 remained on the standard 75 mg daily clopidogrel dose after the procedure and had a follow-up VerifyNow test performed 30–40 days after initiation of clopidogrel administration (53.3%), 17 underwent changes to the standard 75 mg clopidogrel dose after the first VerifyNow test (28.3%), seven were switched to prasugrel after the first VerifyNow test (11.7%), and four remained on the standard 75 mg daily clopidogrel dose after the procedure but did not have a follow-up VerifyNow test performed (6.7%). In addition, four of the 40 patients who underwent simple or balloon assisted aneurysm coiling remained on the standard 75 mg daily clopidogrel dose after the procedure and had a follow-up VerifyNow test performed (10%).
Hence a total of 36 patients in our cohort had a follow-up VerifyNow test performed after the procedure without having undergone changes to the standard 75 mg daily clopidogrel dose, comprising 47.4% of patients who remained on the standard 75 mg daily clopidogrel dose in the perioperative period. In these patients, the mean number of daily 75 mg clopidogrel doses before the first VerifyNow test was 8.8 (median 9 doses, range 5–13 doses). Mean PRU value in the initial VerifyNow test was 137.5 (median 140 PRU, range 32–239 PRU). The mean number of daily 75 mg clopidogrel doses before the follow-up VerifyNow test was 30.2 (median 31 doses, range 14–66 doses). Mean PRU value in the follow-up VerifyNow test was 59.3 (median 48 PRU, range 1–208 PRU). There was a statistically significant decrease in the mean PRU value between the initial (137.5 PRU) and follow-up (59.3 PRU) VerifyNow test in these 36 patients (p<0.0001).
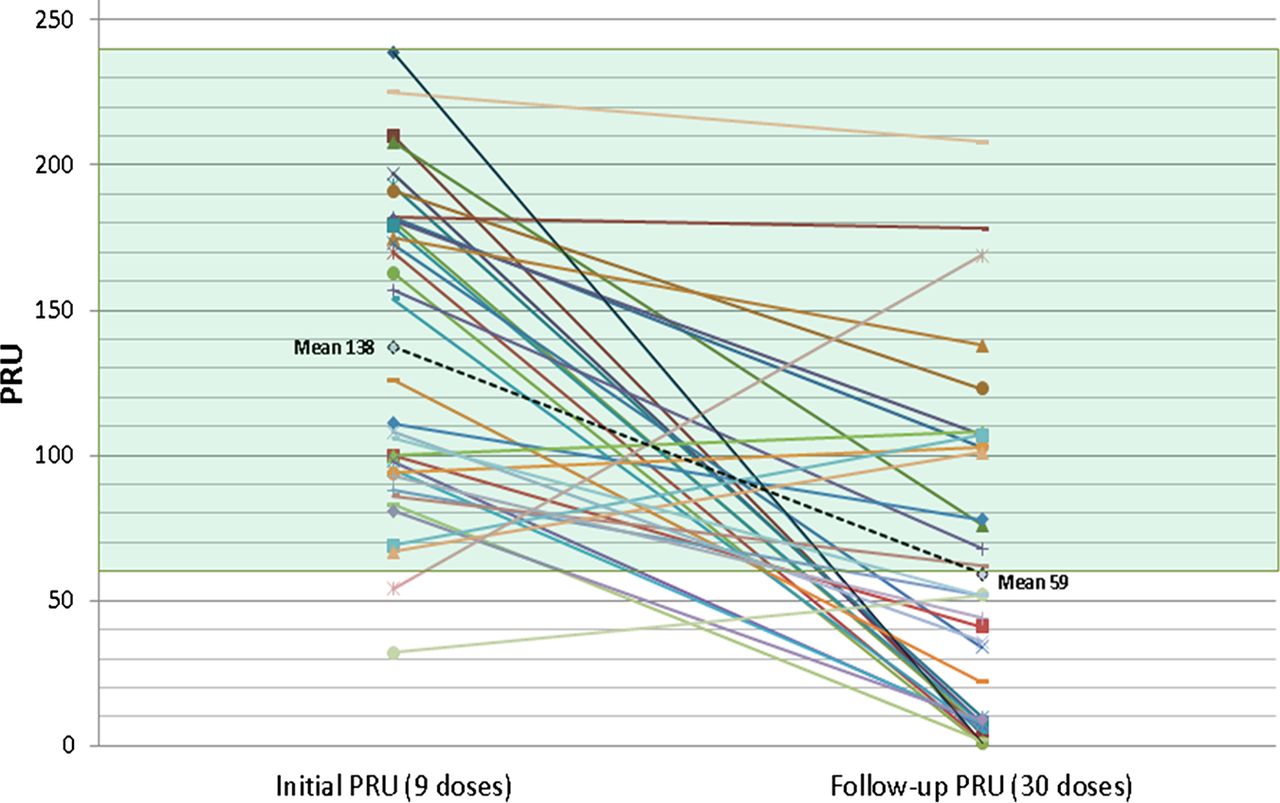
Utilizing a PRU <60 cut-off for a clopidogrel hyper-response, 20 of 34 patients (58.8%) who were not initially considered to be clopidogrel hyper-responders to the standard 75 mg daily clopidogrel dose exhibited a delayed conversion to clopidogrel hyper-response in follow-up testing, with a mean PRU of 17.6 at the time of the follow-up VerifyNow test (median 8 PRU, range 1–52 PRU). Of note, 12 of these 20 patients had markedly decreased PRU values (PRU <10) at the time of the follow-up VerifyNow test (60%). Furthermore, eight of these 20 patients were symptomatic at the time of the delayed clopidogrel hyper-response (40%): seven with abnormal bruising/bleeding and one with ICH. None of the 36 patients who underwent a follow-up VerifyNow test in our cohort exhibited a delayed conversion to hypo-response to the standard 75 mg daily clopidogrel dose. Figure 2 illustrates the change in patient response to the standard 75 mg daily clopidogrel dose in follow-up VerifyNow testing in our cohort.

Change in patient response to the standard 75 mg daily clopidogrel dose between the initial and follow-up VerifyNow tests. PRU, P2Y12 reaction units.
Predictors of a hyper- and hypo-response to clopidogrel therapy
Table 1 summarizes the predictors of a clopidogrel hyper- and hypo-response in our cohort. In univariate analysis, there were no predictors of an initial hypo- or hyper-response to clopidogrel therapy, while a lower weight (p=0.04) and a lower serum creatinine concentration (p=0.01) were predictors of a hyper-response at any time during clopidogrel administration in our cohort. Of note, co-administration of a proton pump inhibitor was not associated with a higher likelihood of a clopidogrel hypo-response in our cohort.
Patient characteristics associated with a hyper- and hypo-response to clopidogrel therapy in patients undergoing endovascular treatment of unruptured cerebral aneurysms
In multivariate logistic regression analysis, a lower body mass index (p=0.01, OR 0.046, 95% CI 0.0045 to 0.48), diabetes mellitus (p=0.02, OR 39.8, 95% CI 2 to 780), co-administration of a selective serotonin reuptake inhibitor (p=0.003, OR 85.5, 95% CI 4.4 to 1649), a lower serum hemoglobin (p=0.02, OR 0.05, 95% CI 0.0039 to 0.68), and a lower platelet count (p=0.02, OR 0.1, 95% CI 0.017 to 0.64) were independent predictors of an initial hypo-response to clopidogrel therapy in our cohort. A lower serum creatinine level (p=0.04, OR 0.33, 95% CI 0.11 to 0.95) was the only independent predictor of a hyper-response at any time during clopidogrel administration in our cohort. There were no independent predictors of an initial hyper-response to clopidogrel therapy in our cohort.
Thromboembolic and hemorrhagic complications and associated hypo- and hyper-response to clopidogrel therapy
Five of the 60 patients who underwent cerebral aneurysm treatment with stent assistance or the PED had a documented clopidogrel hypo-response either shortly before the procedure or at some point during the course of its administration (PRU >240, 8.3%), with a mean PRU of 275 (median PRU 280, range 246–292 PRU), and a mean time from initiation of clopidogrel therapy to the clopidogrel hypo-response of 30 days (median 9 days, range 6–87 days). Among these, two patients experienced a thromboembolic complication at the time of the clopidogrel hypo-response (40%), one causing transient aphasia and one causing permanent disabling contralateral hemiparesis (major). In addition, one patient experienced delayed stent thrombosis causing non-disabling short term memory deficits identified at the time of the first follow-up angiogram (20%). These thromboembolic complications occurred on postoperative days 0, 2, and 183 in patients with pre-procedure PRU values of 275, 262, and 234, and last recorded PRU values of 275, 292, and 280, respectively. Conversely, among the 55 patients who underwent cerebral aneurysm treatment with stent assistance or the PED and did not have a documented clopidogrel hypo-response in our cohort, two experienced thromboembolic complications (3.6%), none of which was major. These thromboembolic complications were an asymptomatic delayed PED thrombosis and a delayed perforator infarction after PED aneurysm treatment causing non-disabling short term memory deficits, both of which were identified at the time of the first follow-up angiogram on postoperative days 170 and 185 in patients with pre-procedure PRU values of 197 and 88 and last-recorded PRU values of 193 and 205, respectively. Overall, among the 60 patients who underwent cerebral aneurysm treatment with stent assistance or the PED in our cohort, there was a statistically significant difference in the likelihood of a thromboembolic complication between patients who had a documented clopidogrel hypo-response (60%) and those who did not (3.6%, p=0.003).
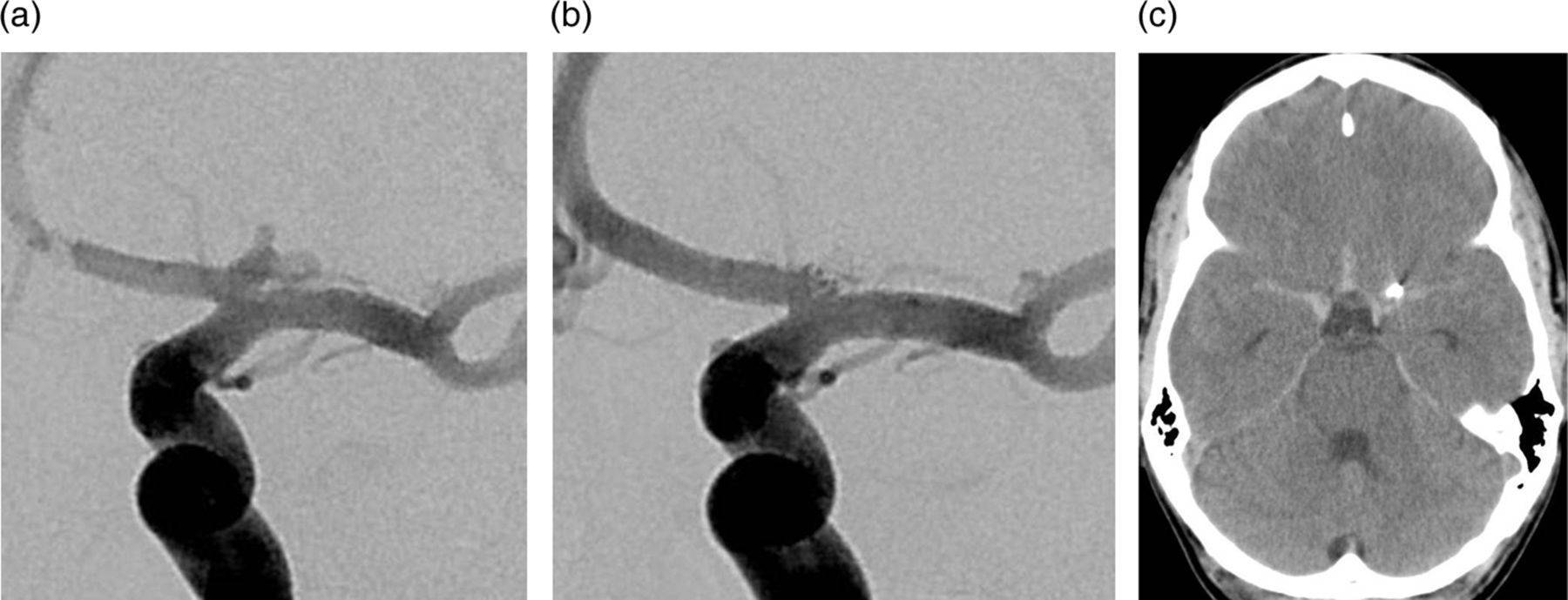
Forty-five patients in our cohort had a documented hyper-response to clopidogrel therapy either shortly before the procedure or at some point during the course of its administration (PRU <60, 45%), with a mean PRU of 20.8 (median PRU 10, range 0–59 PRU), and a mean time from initiation of clopidogrel therapy to the clopidogrel hyper-response of 19.6 days (median 15 days, range 5–76 days). Among these, 18 patients were symptomatic at the time of the clopidogrel hyper-response (40%): 13 with abnormal bruising/bleeding (28.9%), one with a small amount of subarachnoid hemorrhage 2 days after balloon assisted aneurysm coiling without intraoperative aneurysm rupture (2.2%, figure 3), and four with ICH (8.9%, three after PED procedures and one after stent assisted coiling). Thus, five of the 45 patients with a documented clopidogrel hyper-response in our cohort experienced a major hemorrhagic complication at the time of the hyper-response (11.1%). These major hemorrhagic complications occurred on postoperative days 2, 4, 7, 8, and 50 in patients with pre-procedure PRU values of 5, 246, 72, 170, and 34, and last recorded PRU values of 5, 10, 59, 2, and 58, respectively. Conversely, five of the 55 patients who did not have a documented clopidogrel hyper-response in our cohort experienced abnormal bruising/bleeding during the course of clopidogrel administration (9.1%), but none had a major hemorrhagic complication. Overall, in our cohort, there was a statistically significant difference in the likelihood of a major hemorrhagic complication between patients who had a documented clopidogrel hyper-response (11.1%) and those who did not (0%, p=0.016).
{kind=link}
{kind=link}
{kind=link}
A patient in their late thirties with a family history of brain aneurysms presented for endovascular treatment of a multi-lobulated left A1 segment aneurysm identified at screening. Pre-procedure P2Y12 reaction units (PRU) value after five 75 mg clopidogrel doses was 5. Clopidogrel administration was discontinued but the procedure was undertaken. (A) Frontal left internal carotid angiogram demonstrates a multi-lobulated left A1 segment aneurysm measuring 5 mm in maximum dimension. (B) Frontal left internal carotid angiogram demonstrates near complete obliteration of the aneurysm sac after balloon assisted coil embolization. There was no angiographic evidence of contrast extravasation or changes in blood pressure intraoperatively to suggest intraoperative aneurysm rupture. The patient was discharged home on postoperative day 1, neurologically intact with a mild to moderate headache, controlled with oral pain medications. On postoperative day 2, the patient was woken up by the sudden onset of a severe headache. (C) Non-contrast head CT demonstrated a small amount of subarachnoid hemorrhage, predominantly in the anterior aspect of the suprasellar cistern. The patient was discharged home 7 days after hospital readmission, neurologically intact.
Discussion
We found wide variability in the initial patient response to the standard 75 mg daily clopidogrel dose in our cohort, which is similar to that described by Lee et al3 in a cohort of patients undergoing different types of neurointerventional procedures. Assuming that our patient cohort is representative of the general cerebral aneurysm patient population, it is plausible that the variability in initial patient response to the standard 75 mg daily clopidogrel dose could explain some of the thromboembolic and hemorrhagic complications encountered shortly after endovascular treatment of cerebral aneurysms with stent assistance or flow diversion. Namely, patients with a pre-procedure clopidogrel hypo-response (high PRU value) may be at an increased risk of thromboembolic complications in the immediate perioperative period, while patients with a pre-procedure clopidogrel hyper-response (low PRU value) may be at an increased risk of major hemorrhagic complications in the immediate perioperative period.
Further, we evidenced a significant decrease in PRU values after continued administration of the standard 75 mg daily clopidogrel dose in our cohort, with a mean of 137 PRU after the first 8–9 doses and a mean of 59 PRU after 30 doses (p <0.0001). In addition, 59% of patients who were not initially considered hyper-responders to the standard 75 mg daily clopidogrel dose experienced a delayed conversion to hyper-response in follow-up testing. Hence, it is plausible that a delayed conversion to clopidogrel hyper-response could explain some of the delayed hemorrhagic complications encountered after stent assisted coiling and PED procedures, even if the initial pre-procedure PRU value is within the target PRU range.
A significantly higher proportion of patients in our cohort were outside the proposed ‘optimal’ target range of 95–207 PRU (66%) compared with the proposed ‘acceptable’ target range of 60–240 PRU (36%) in pre-procedure VerifyNow testing after 8–9 clopidogrel doses. Hence, if neurointerventional procedures requiring clopidogrel therapy were to be rescheduled until patients are within a target PRU range in pre-procedure testing, then using the ‘acceptable’ PRU range may lead to less cancellations and schedule disruptions than using the ‘optimal’ PRU range. While in our cohort we encountered no major thromboembolic or hemorrhagic complications in patients who were between the proposed ‘optimal’ and ‘acceptable’ PRU ranges (208–240 PRU and 60–94 PRU, respectively), further studies are needed to ensure that using the ‘acceptable’ 60–240 PRU range would not lead to increased thromboembolic or hemorrhagic complications in a larger patient population.
In our cohort, a lower serum creatinine concentration was an independent predictor of a clopidogrel hyper-response at any time during its administration, while there were several independent predictors of an initial clopidogrel hypo-response: lower body mass index, presence of diabetes mellitus, lower serum hemoglobin, lower platelet count, and co-administration of a selective serotonin reuptake inhibitor. Although the clinical significance of these findings is not presently clear and could certainly be related to a ‘statistical fluke,’ the association of a lower platelet count with an increased likelihood of identifying a clopidogrel hypo-response may be intrinsically related to the VerifyNow assay. Interestingly, women patients were more likely to experience an initial (25%) or any (49%) clopidogrel hyper-response than male patients (8%, 33%) in our cohort, although this finding did not reach statistical significance. Notably, administration of a selective serotonin reuptake inhibitor did not significantly increase the likelihood of a clopidogrel hyper-response, and administration of a proton pump inhibitor or statin did not significantly increase the likelihood of a clopidogrel hypo-response in our cohort.
A clopidogrel hyper-response was associated with an 11% risk of a major hemorrhagic complication in our cohort, which was significantly higher than the risk in patients who did not exhibit a clopidogrel hyper-response (0%). Furthermore, a clopidogrel hypo-response was associated with an increased risk of thromboembolic complications in patients undergoing cerebral aneurysm treatment with stent assistance or the PED in our cohort (60%), which was significantly higher than the risk in patients who did not have a documented clopidogrel hypo-response (3.6%). Overall, these findings provide evidence that a clopidogrel hypo- or hyper-response may explain some of the thromboembolic and hemorrhagic complications encountered after endovascular treatment of cerebral aneurysms. Nevertheless, future prospective studies are needed to determine if active management of clopidogrel dosing to maintain patients undergoing endovascular treatment of unruptured cerebral aneurysms within a target PRU range (proposed 60–240 PRU) may minimize the risk of thromboembolic and hemorrhagic complications.
Our study's limitations are the modest sample size, retrospective design, and lack of follow-up VerifyNow testing in all patients who did not undergo changes to the standard 75 mg daily clopidogrel dose. The latter may have led to an overestimation of the proportion of patients who experienced a delayed conversion to clopidogrel hyper-response in this study.
Conclusion
We found wide and dynamic variability in response to clopidogrel therapy in patients undergoing endovascular treatment of unruptured cerebral aneurysms, with 59% of patients demonstrating a delayed conversion to a hyper-response to the standard 75 mg clopidogrel dose in follow-up testing. In our cohort, a clopidogrel hypo-response was associated with a significantly increased risk of thromboembolic complications in patients undergoing cerebral aneurysm treatment with stent assistance or the PED, while a clopidogrel hyper-response was associated with a significantly increased risk of major hemorrhagic complications in all patients undergoing endovascular treatment of unruptured cerebral aneurysms.
References
Footnotes
Correction notice This article has been corrected since it was published Online First. Changes have been made to table 1, small text changes on pages 5 and 6 and an additional reference has been added.
Acknowledgements The authors would like to acknowledge Sandee K Verootis, Radiology Department, Abbott Northwestern Hospital, for her contribution in the data collection for this study.
Contributors JEDA: study design, data collection, data analysis, and manuscript preparation. YK: study design, data collection, and manuscript revision. BMC: study design and manuscript revision. JLF: data collection, data analysis, and manuscript revision. JMS: study design and data collection. DET: study design and manuscript revision.
Competing interests JEDA, YK, BMC, and DET have consulting agreements with Covidien/ev3.
Ethics approval The study was approved by Abbott Northwestern Hospital institutional review board.
Provenance and peer review Not commissioned; externally peer reviewed.