Article Text

Abstract
Background/purpose Various aneurysm animal models have been utilized to study the histological reaction post coil embolization. Our aim was to evaluate the imaging findings at day 14 of a rat external carotid artery side wall aneurysm treated with coil embolization using a gradient echo sequence on 7 T MRI and to correlate this with the histological findings.
Materials and methods Male Sprague Drawley rats were utilized to create a sidewall external carotid artery blind pouch aneurysm. A 5 mm segment of hydrocoil or bare platinum coil was inserted into the created aneurysm. Five sham operated rats were used as controls. The arterial construct was harvested on day 14. The block of tissue was evaluated with histopathology and immunohistochemistry. Prior to sacrifice, the animal underwent 7 T MRI. Statistical analysis was then performed to assess the correlation of signal abnormality with intra-aneurysmal thrombus formation on histology.
Results 10 rats were used for the experiment. Five rats had implantation of hydrocoils and five of bare platinum coils. There was a statistically significant linear correlation between the intra-aneurysmal thrombus on histology and gradient echo 7 T MRI sequences. There was no correlation demonstrated in the hydrocoil implanted group. No thrombus or abnormal signal was seen in the sham group.
Conclusions In our experiment, thrombus formation in aneurysms treated with bare platinum coils is well correlated with the presence of abnormal signal on 7 T MRI at 14 days. No correlation was appreciated in the hydrocoil implanted group due to the presence of intra-aneurysmal reactive tissue instead of thrombus.
- Aneurysm
- Coil
- MRI
Statistics from Altmetric.com
Introduction
Subarachnoid hemorrhage from a ruptured cerebral aneurysm is a significant cause of morbidity and mortality. Cerebral aneurysms have traditionally been treated with surgical clip placement but over the past two decades, endovascular techniques have gained acceptance. The Guglielmi Detachable Coil was approved by the Food and Drugs Association in 1995.1 Coil technology has been subsequently refined, and based on the International Subarachnoid Aneurysm Trial is the preferred method of treatment for ruptured aneurysms.1 In spite of this, endovascular therapy continues to be plagued with a high incidence of aneurysm recurrence following treatment.2 ,3 In order to reduce the incidence of recurrence, traditional bare platinum coils have been modified with bioactive/expansile gel material coating. The two most common materials tried in clinical practice have been poly-glycolic acid (PGLA) and hydrogel. While PGLA has not been shown to offer any added value in preventing aneurysm recurrence following embolization, the hydrogel coated coils do demonstrate some benefit in medium sized aneurysms.4 ,5
New bioactive coatings continue to be placed on traditional platinum based coil platforms. These have been tested in various animal models.6–10 Typically the assessment of new coated coil technology is based on histological tissue examination; however, this requires sacrifice of the animal. MRI with higher magnet strength is evolving at a rapid pace, with some recent human applications in the evaluation of cerebral aneurysms treated with coil embolization.11–13 In contrast, application of high field strength MRI in the evaluation of aneurysms treated with coil embolization is limited in animal models.14 Based on this, we examined the hypothesis that there is a correlation between the MRI findings of thrombus formation within an aneurysm and histology. Potentially, this would allow study of aneurysm healing without sacrifice of the animal.
The purpose of this study was to evaluate the imaging findings at day 14 of a rat external carotid artery (ECA) side wall aneurysm treated with coil embolization using a gradient echo sequence on 7 T MRI and to correlate this with the histological findings.
Materials and methods
Animal preparation and coil placement
The protocols for animal use were approved by the University of Michigan Committee on the Use and Care of Animals. A total of 15 adult male Sprague Drawley rats weighing between 350 and 400 g were used. Access to food and water was ad libitum. General anesthesia was induced by intraperitoneal injection of 60 mg/kg sodium pentobarbital (Nembutal; Ovation Pharmaceuticals Inc, Deerfield, Illinois, USA). Body temperature was maintained at 37°C by use of a feedback controlled heating pad. Under sterile conditions, bare platinum coils (Microplex 18; MicroVention Inc, Tustin, California, USA) and hydrogel coated coils (HydroCoil 14 or 18; MicroVention Inc) were cut into 5 mm long segments.
Once the rats were effectively anesthetized, they were placed in the supine position and the anterior neck region was prepped and draped under sterile conditions. A paramedian incision was then made, and blunt/sharp dissection was carried out through the fascia and muscle until the carotid sheath was identified. The carotid sheath was then opened, leading to dissection of the internal carotid artery (ICA), ECA, and common carotid artery (CCA). A permanent ligature was placed 5–7 mm distal to the origin of the ECA using 6-0 silk suture. A small arteriotomy was made at the site just proximal to the ligature after proximal blood flow of the ECA was controlled by temporary clipping of the CCA and ICA. A 5 mm coil segment (bare coil or HydroCoil) was then inserted into the ECA lumen until the tip of the coil was positioned at the origin of the ECA. Another ligature was made at the proximal site of the arteriotomy to prevent bleeding and coil migration, and the temporary clips on the CCA and ICA were released to restore blood flow. The operative field was inspected to confirm hemostasis and proper location of the coil in the newly created side wall ECA blind pouch aneurysm. Vasodilation and pulsation of the ECA blind pouch aneurysm were recognized on removal of the temporary clips, and the wound was closed with 4-0 nylon sutures. Sham operated control rats underwent an identical procedure except that no coil was inserted into the ECA lumen. The rats were returned to their cages and given access to food and water ad libitum.
Magnetic resonance imaging
All rats were anesthetized with a 2% isoflurane/air mixture throughout the MRI examination. Rats lay prone, head first in a 7.0 T Agilent MR scanner (183 mm horizontal bore; Agilent, Santa Clara, California, USA) with body temperature maintained at 37°C using forced heated air. A double tuned volume radiofrequency coil was used to scan the neck region of the rats. Axial T2* weighted images were acquired using a gradient echo sequence with the following parameters: repetition time (TR)/effective echo time (TE), 250/6 ms; flip angle of 20; field of view, 20×35 mm; matrix, 256×128; slice thickness, 0.5 mm; slice spacing, 0 mm; and number of slices, 15. Total scan time was ∼ 3.0 min. On day 14 after coil insertion, the carotid bifurcation was imaged under inhalational anesthesia (1.5% isoflurane) in the small bore 7 T MRI according to the specifications described above. Based on the extrapolation of signal characteristics of endovascular thrombus in humans, we determined that gradient echo sequences (T2* weighted images) would be the optimal method to quantify the amount of endoluminal thrombus. The cross sectional image showing the maximum area of blooming artifact was chosen in a blinded fashion. The assessor then measured the area within the region of interest as the surrogate marker of the amount of thrombus. The same area on the contralateral side was used for normalization for the purpose of measurement.
Histological examination
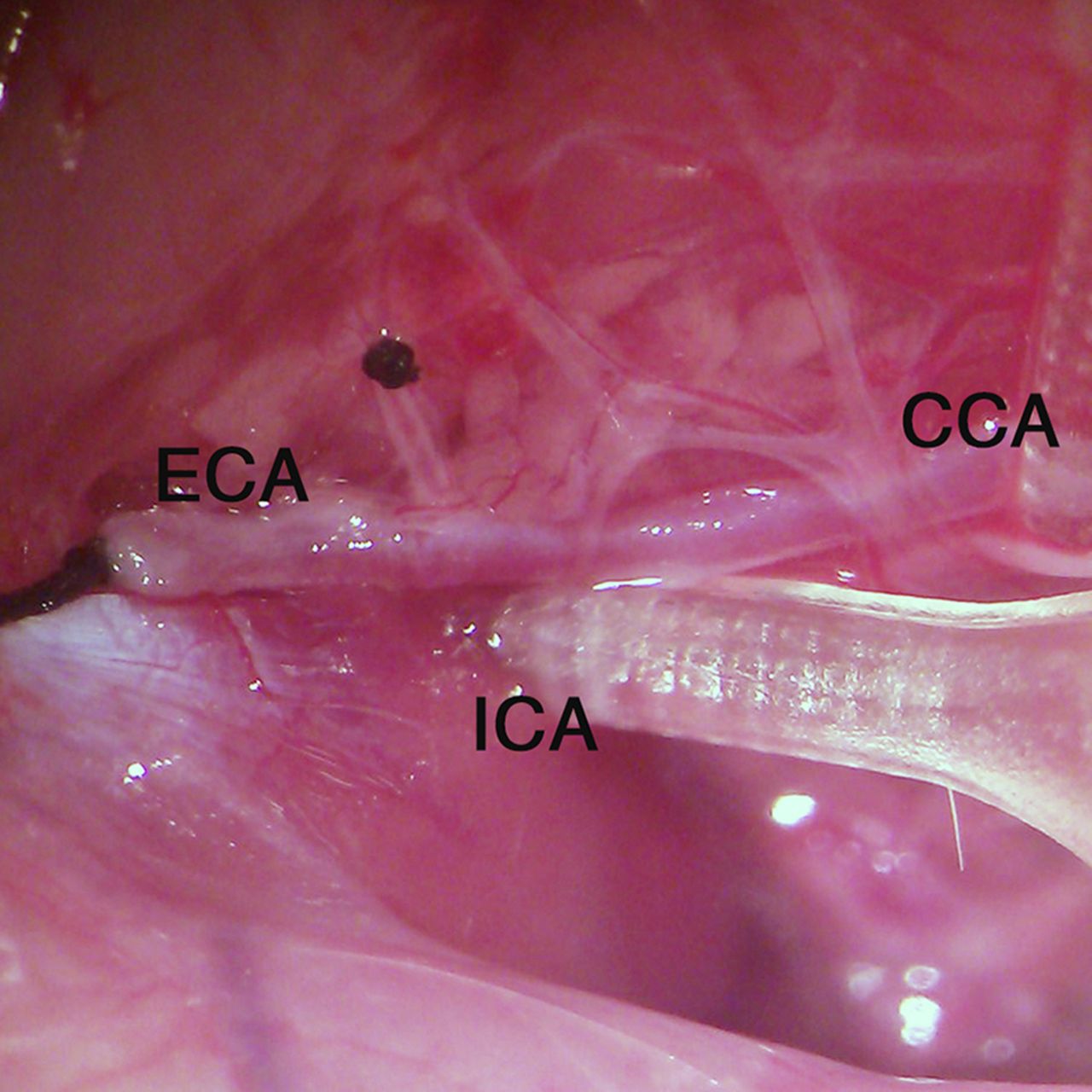
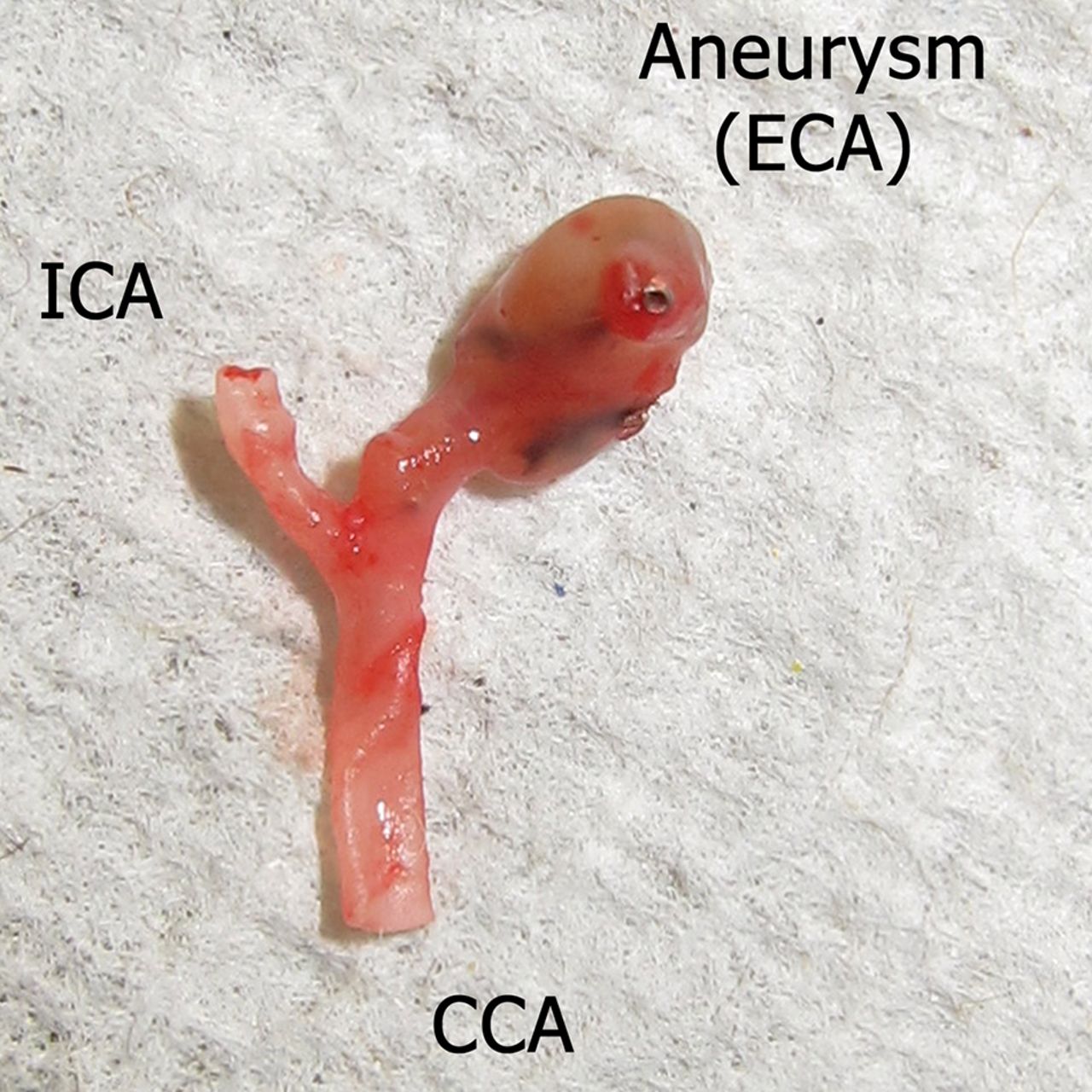
Following 7 T MRI, the animals were euthanized by intraperitoneal injection of 300 mg/kg sodium pentobarbital. The previous incision was reopened and the CCA, ICA, and ECA were exposed (figure 1). The entire bifurcation, including the ECA aneurysmal sac, was harvested for further evaluation (figure 2). The inner lumens of the CCA and ICA were washed with 10 U/mL heparin saline solution and 4% paraformaldehyde in 0.1 mol/L phosphate buffered saline (pH 7.4) and then fixed in 4% paraformaldehyde for 72 h at room temperature. After fixation, the inserted coils were removed from the ECA blind pouch aneurysm under microscopic guidance. The aneurysmal sac was then incised in the center so that the carotid artery bifurcation was separated into the dome side and orifice side. Specimens were then placed in a 70% ethanol–water mixture, and the dome side of the ECA blind pouch aneurysm segments were embedded in paraffin and cut into 4 μm thick slices in cross section.

The intraoperative picture shows permanent ligature of the external carotid artery (ECA) and temporary clipping of the common carotid artery (CCA) and the internal carotid artery (ICA).

The entire carotid bifurcation, including the external carotid artery (ECA) aneurysmal sac, was harvested on the 14th day after surgery. CCA, common carotid artery; ICA, internal carotid artery.
Conventional staining
Thin cut tissue sections were stained with hematoxylin–eosin (H&E) and elastic van Gieson according to standard protocols. After conventional staining, the slides were examined microscopically and photographed using a digital camera. The images were analyzed by a single observer who was blinded to the different groups.
Morphometric and statistical analysis
Slides from the dome side of the treated aneurysms were examined for the encircled area lined by internal elastic lamina, which was identified as the vascular lumen. Cellular and fibrotic components in the lumen were defined as organized healing tissue. Using image analysis software (NIH Image J, V.1.43u), the blinded single observer calculated the area of thrombus formation/organized healing tissue as a percentage of the entire cross section area of the histology specimen.
The maximal area (region of interest) of the blooming artifact on MRI was measured independently by a separate observer blinded to the different groups and the measurements on histology. Using image analysis software (NIH Image J, V.1.43u), the blinded single observer calculated the volume of thrombus formation (region of interest×slice (axial) thickness (mm)/matrix (256)) within the aneurysm on MRI.
Data are presented as mean±SD. The measured values on histological sections and MRI were then analyzed using the Pearson correlation coefficient (PCC) by SPSS V.15.0.
Results
H&E stained histopathology of the experimental aneurysms in the sham group and corresponding MRI are featured in figures 3 (A, D) and 4 (A, D). H&E stained images showed the absence of thrombus in the aneurysm of sham animals (figures 3D and 4D), and the corresponding MRI revealed there was no blooming artifact (figures 3A and 4A). In the bare platinum coil group, H&E stained images showed varying thrombus in the lumen of the aneurysm (figure 3E), and the blooming artifact could be found in the corresponding MRI (figure 3B). In the HydroCoil group, H&E stained images revealed large amounts of organized tissue in the aneurysm (figure 4E) but there was no correlative increase in blooming artifact on the corresponding MRI (figure 4B). The elastic van Gieson staining revealed that the internal elastic lamina of the aneurysm was minimally damaged in the bare coil group (figure 3F), but severely damaged within the Hydrocoil group (figure 4F). In some animals in the HydroCoil group, the entire elastic lamina was destroyed.

(A) MRI axial image shows no blooming artifact in the sham group. (B) MRI axial image shows blooming artifact at the site of the coil insertion in the bare coil group. (C) Yellow circle shows the region of interest of the blooming artifact where the measurement was performed. (D) Hematoxylin–eosin (H&E) stain image shows the absence of thrombus in the aneurysm of the sham group. (E) H&E stain image shows thrombus in the lumen of the aneurysm in the bare platinum coil group. (F) The elastic van Gieson stain image shows that the internal elastic lamina is minimally damaged in the bare coil group.

(A) MRI axial image shows no blooming artifact in the sham group. (B) MRI axial image shows a small blooming artifact at the site of coil insertion in the HydroCoil group. (C) Yellow circle shows the region of interest of the blooming artifact where the measurement was performed. (D) Hematoxylin–eosin (H&E) stain image shows the absence of thrombus in the aneurysm of the sham group. (E) H&E stain image shows large amounts of organized tissue in the aneurysm of the HydroCoil group. (F) The elastic van Gieson stain image shows that the internal elastic lamina is severely damaged in the HydroCoil group.
The percentage of the area of organized tissue on histological sections 2 weeks after surgery was greater in the HydroCoil group than in the bare coil group (49.01±24.83% vs 24.46±23.9%, p=0.06), although this did not reach statistical significance. There was no statistically significant difference in the volume of thrombus formation in the aneurysm on MRI between the HydroCoil group and the bare coil group (0.37±0.04 mm3 vs 0.69±0.51 mm3, p=0.25).
Data on the correlation between the area of organized tissue on histological sections and the volume of thrombus formation in the aneurysm on T2* gradient recalled echo MRI sequences are listed in table 1. In the bare coil group, a significant correlation was found (PCC=0.987 (p=0.002)), but no correlation was demonstrated in the HydroCoil group (PCC=0.344 (p=0.571)). The scatter diagram demonstrated a linear correlation in the bare coil group and no correlation in the HydroCoil group (figure 5).
Data correlation between the area of organized tissue on histological sections and the volume of thrombus formation in the aneurysm on T2* gradient recalled echo MRI sequences

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The scatter diagram demonstrates a linear correlation in the bare coil group with no correlation in the HydroCoil group.
Discussion
In this study, we investigated whether the imaging findings on day 14 of a rat ECA side wall aneurysm treated with coil embolization on 7 T MRI using a T2* gradient echo sequence correlated with histological findings. Our results showed that for aneurysms treated with bare platinum coils there was a correlation with the amount of thrombus formation identified histologically with the imaging findings on a T2* gradient echo sequence of a 7 T MRI. In the group of aneurysms treated with hydrogel coated coils, the correlation disappeared. This phenomenon in our opinion can be explained by the exuberant tissue proliferation demonstrated on histology in the coated coil group of rats. The presence of altered blood products in the form of intra-aneurysmal thrombus creates the signal aberration on MR. The tissue proliferation secondary to endothelial lining disruption caused by the gel coating on the surface of the coil and the lack of luminal thrombus within the aneurysm explains the lack of correlation with the MR signal aberration. This phenomenon, in our opinion, adds credibility to our hypothesis that when there is thrombus formation within the aneurysm, there is a robust correlation on unenhanced 7 T MR T2* sequences.
Marjamaa et al14 demonstrated in their experiment the appearances on MRI of the aneurysms created in the rat abdominal aorta. They demonstrated better neck exclusion in the PGLA coated coil group in comparison with bare platinum coils. They compared the two groups with histology and MRI time of flight sequences utilizing a 4.7 T magnet. They demonstrated good correlation with dog ear filling of coiled aneurysms on MR with endoscopic evaluation of the parent vessel and aneurysm neck interface. Other studies have applied 3 T MR imaging but they were in large animal groups.15 ,16 The choice of 7 T MR by us was based on the hypothesis that higher magnet field strength translates to better resolution, which should allow for improved spatial resolution for MR image analysis in a small animal aneurysm model like ours. More recently, 7 T MRI has been applied in human subjects to validate images with improved spatial resolution.11–13 T2* is an ideal sequence for evaluating treated aneurysms as it has been specifically helpful in identifying altered blood products/thrombus within aneurysms, calcium, and iron within tissues.17 ,18 Our goal was to utilize this MRI sequence for assessing the degree of thrombosis within a treated experimental rat aneurysm.
The rat carotid artery ECA blind pouch aneurysm model is widely used for assessment of coil related tissue reaction within the aneurysm.19 Hence we elected to design our experiment utilizing the blind pouch ECA aneurysm model in rats. Previous animal aneurysm models demonstrated healing mainly on histology following sacrifice of the animal.6 ,7 This method does not allow for chronological assessment of aneurysm healing following coil embolization. Only some animal aneurysm models have applied MRI to non-invasively evaluate aneurysm healing.14 At the time of preparation of this manuscript, there was no published literature demonstrating the feasibility of application of 7 T MRI in the assessment of aneurysm healing initiated by endosaccular coils in a rat aneurysm model.
Aneurysmal recurrence following endovascular coil embolization continues to cloud the durability of endovascular treatment for cerebral aneurysms.20 ,21 To design better coils for permanent healing of cerebral aneurysms, animal models have been developed to evaluate the efficacy and durability of such coils. The rat cervical carotid side wall aneurysm represents an arterial aneurysm model for coil evaluation. We insert coil segments within this experimental aneurysm to evaluate histological reaction over time. Such analysis requires the experimental aneurysm to be harvested in continuity with the parent vessel, requiring sacrifice of the animal. Evaluation of coiled experimental aneurysms over a prolonged duration requires numerous animals, thus increasing the costs associated with such analyses. To allow for longer survival analyses as well as cost reduction, experimental aneurysmal healing post coiling could be evaluated with non-invasive imaging technologies, such as MRI.
There are several limitations to our experiment. The carotid bifurcation model still does not precisely imitate the cerebral aneurysm environment in the human population. The groups of rats utilized in the bare platinum group and the coated coil group were small, which makes statistical analysis less robust. However, we believe that the study demonstrates the feasibility of using MR with higher magnet strength (7 T) in a small animal aneurysm model. It also demonstrates that MR based imaging with T2* gradient echo sequence is a reliable method to evaluate the nature of aneurysmal healing by thrombus formation. In the current climate, there is an unmet need for better evaluation of aneurysm healing chronology before sacrifice of the animal for histological assessment. The technique we describe, once further validated in a larger animal sample, will allow for a more robust surrogate indicator of aneurysm healing. However, it is important to bear in mind that if the primary healing is via exuberant tissue reaction to the coil, then MRI may not be the best non-invasive imaging modality.
Conclusion
There is a reliable correlation of the extent of thrombus formation in a rat ECA side wall aneurysm model treated with bare platinum coil on 7 T MRI gradient echo sequence with histology. The correlation needs further validation in a large animal aneurysm model with a larger sample size. The 7 T MRI correlation with histology can be potentially exploited in future experiments to assess the temporal progression of aneurysmal healing with thrombus formation without sacrificing the animal.
References
Footnotes
-
Contributors CZ: aneurysm model creation, surgery, histology slide staining, measurements on histology, data analysis, and manuscript creation. NC: design of the study, MRI protocol generation, data analysis, and manuscript creation. JJG: manuscript editing. AE: MRI data collection, region of interest measurements, and manuscript editing. JS: data analysis and manuscript creation. BGT: manuscript editing. CG: MRI protocol verification and manuscript editing. GX: study design and manuscript editing. ASP: study design, aneurysm model creation, and manuscript editing.
-
Competing interests None.
-
Ethics approval The protocols for animal use were approved by the University of Michigan Committee on the Use and Care of Animals.
-
Provenance and peer review Not commissioned; externally peer reviewed.