Article Text

Abstract
Introduction Conventional Onyx embolization of cerebral arteriovenous malformations (AVMs) requires lengthy procedure and fluoroscopy times to form an adequate ‘proximal plug’ which allows forward nidal penetration while preventing reflux and non-targeted embolization. We review our experience with balloon-augmented Onyx embolization of cerebral AVMs using a dual-lumen balloon catheter technique designed to minimize these challenges.
Methods Retrospectively acquired data for all balloon-augmented cerebral AVM embolizations performed between 2011 and 2014 were obtained from four tertiary care centers. For each procedure, at least one Scepter C balloon catheter was advanced into the AVM arterial pedicle of interest and Onyx embolization was performed through the inner lumen after balloon inflation via the outer lumen.
Results Twenty patients underwent embolization with the balloon-augmented technique over 24 discreet treatment episodes. There were 37 total arterial pedicles embolized with the balloon-augmented technique, a mean of 1.9 per patient (range 1–5). The treated AVMs were heterogeneous in their location and size (mean 3.3±1.6 cm). Mean fluoroscopy time for each procedure was 48±26 min (28 min per embolized pedicle). Two Scepter C balloon catheter-related complications (8.3% of embolization sessions, 5.4% of pedicles embolized) were observed: an intraprocedural rupture of a feeding pedicle and fracture and retention of a catheter fragment.
Conclusions This multicenter experience represents the largest reported series of balloon-augmented Onyx embolization of cerebral AVMs. The technique appears safe and effective in the treatment of AVMs, allowing more efficient and controlled injection of Onyx with a decreased risk of reflux and decreased fluoroscopy times.
- Arteriovenous Malformation
Statistics from Altmetric.com
Introduction
With an incidence of approximately 1.2 per 100 000 person years or approximately 4.3% of the population,1 ,2 cerebral arteriovenous malformations (AVMs) are uncommon lesions that pose a unique challenge to the neurointerventional surgeon. While there are many described classification systems for AVMs, these lesions are heterogeneous and therefore treatment and prognosis must be tailored to the individual patient. In general, the risk of bleeding appears to be 2–4% per year per person and appears to be increased if intranidal aneurysms, deep venous drainage, venous stenosis, or venous stasis are present.3 ,4 Those presenting with prior hemorrhage and those with small deep-seated lesions are also at increased risk for hemorrhage.5 ,6 Treatment options include expectant management, open surgery, endovascular embolization, radiosurgery, and any combination of these.7
Endovascular embolization with ethylene vinyl alcohol copolymer, known as Onyx (Covidien/ev3 Neurovascular, Irvine, California, USA), has gained favor as an effective adjuvant treatment for these lesions. However, the traditional approach to Onyx embolization requires a lengthy time under fluoroscopy due to the necessity to create a large Onyx plug proximally to ensure vessel protection and avoid reflux of embolisate. Recent small case series suggest that use of the Scepter C dual-lumen balloon microcatheter (MicroVention, Tustin, California, USA) allows the balloon portion of the microcatheter to act as the proximal plug, summarily resulting in greater protection from reflux of embolisate, greater vessel protection, and shorter time under fluoroscopy.8–10 We describe the results of a multicenter series of 20 patients with cerebral AVMs that were embolized using the balloon-augmented Scepter C microcatheter technique.
Materials and methods
Approval from the Institutional Review Board was obtained to allow data to be retrospectively reviewed from the neuroendovascular case logs of four centers: Medical University of South Carolina, East Carolina University-Vidant Medical Center, Wake Forest University-Baptist Medical Center, and Geisinger Medical Center. From these case logs we identified all patients in whom the Scepter C balloon catheter was used as part of the endovascular treatment regimen for their AVM. All patient demographics, procedural data, and clinical follow-up information were obtained in this retrospective fashion from the medical record. Immediate angiographic outcomes were determined by estimating the percentage of nidus reduction in the immediate post-treatment angiograms per treatment session.
Balloon-augmented Onyx embolization technique
All procedures were performed under general anesthesia in the neuroangiography suite. A 6Fr introducer sheath was introduced into the common femoral artery and a 6Fr guide catheter was introduced into the internal carotid or vertebral artery of interest using standard technique. The choice of arterial pedicle(s) most appropriate for balloon-augmented Scepter C embolization was made by the treating physician on a case-by-case basis. Not every pedicle embolized in a given session was embolized with the Scepter C balloon technique. Traditional techniques were used with some pedicles at the treating physician's discretion. The most common reason for this was difficulty maneuvering the Scepter balloon into position or small size of parent vessel.
The Scepter C balloon catheter was prepared according to the manufacturer’s recommendations. Balloon contrast mix was prepared in either 50/50 or 60/40 (contrast/saline) ratio for visualization of the balloon. A 0.014 inch Synchro-2 microwire (Stryker Neurovascular, Fremont, California, USA), 0.014 inch Transcend microwire (Stryker) or 0.014 inch Traxcess microwire (Mirovention) was placed within the inner lumen of the Scepter C balloon catheter which was then advanced over the microwire into the arterial pedicle of interest. The Scepter balloon comes in three different lengths and the choice of device length was made at the discretion of the treating physician.
Once the balloon catheter was in position within the desired segment of the artery, the balloon was inflated through the catheter's outer lumen hub with the contrast/saline mixture. The goal of the inflation was to completely occlude the arterial pedicle without causing injury. In our experience, both the Scepter C and Scepter XC balloons are extremely compliant, allowing for good conformation of the balloon with regard to vessel geometry. Next, the microwire was removed from the inner lumen of the Scepter C balloon catheter. The inner lumen hub and catheter dead space of the Scepter C balloon catheter is 0.44 mL, and this volume was primed with dimethyl sulfoxide (DMSO). While the balloon remained inflated, embolization was achieved by infusing Onyx through the inner lumen into the AVM nidus. Upon completion of Onyx embolization the balloon was deflated, control was angiography performed through the guide catheter and the Scepter C balloon catheter was subsequently removed from the pedicle. Additional pedicles were embolized at the discretion of the treating physician. If the Scepter C balloon catheter technique was used on an additional arterial pedicle, a new Scepter C balloon catheter was obtained.
Results
Patient and AVM characteristics
The balloon-augmented Scepter C embolization technique was used in 20 patients who underwent a total of 37 endovascular embolization procedures (any technique) during the course of their AVM treatment. Thirteen of these 37 procedures did not involve the Scepter C device technique and data from those sessions were not reviewed or reported. The balloon-augmented Scepter C embolization technique was used during the remaining 24 procedures; 23 of these procedures used the Scepter C technique exclusively. There were 37 discreet arterial pedicles embolized using the balloon-augmented Scepter C technique in this patient cohort during the 24 Scepter C embolization sessions. The results are summarized in table 1.
Patient and AVM characteristics and results of balloon-augmented Scepter embolization technique
The location of the treated AVMs included frontal (n=4), temporal (n=1), parietal (n=1), frontoparietal (n=3), temporoparietal (n=1), parieto-occipital (n=1), occipital/pineal (n=3), cerebellar (n=5), and one AVM located throughout multiple eloquent areas. The mean±SD size of the AVMs was 3.3±1.61 cm, with the largest malformation measuring 6.2 cm and the smallest 1.1 cm. Ten AVMs (50%) were treated in the setting of hemorrhage and the remaining 10 were unruptured.
Procedures
In all patients the Scepter C balloon microcatheter was maneuvered into position without significant difficulty. The balloon was inflated without difficulty in 36 of 37 pedicles and embolization with Onyx proceeded accordingly. Of the 24 individual treatment procedures where the Scepter device was used, we noted a time under fluoroscopy of 48±26 min per procedure (there were two procedures for which time under fluoroscopy was not available). The mean number of pedicles embolized per patient was 2 (range 1–5). In four patients radiosurgery was undertaken following embolization. In 12 patients, resection followed embolization, one patient had resection prior to embolization, and the remaining three patients had no adjuvant treatment following embolization.
Angiographic outcomes
We categorized our immediate angiographic outcomes by percentage of total nidus reduction in the immediate angiographic follow-up per embolization session compared with the size of the untreated AVM. There were 24 total sessions in the 20 patients treated in which the Scepter device was used. We achieved complete angiographic obliteration of the nidus in three patients (15%) after the initial session with the Scepter microcatheter. In seven treatment sessions we achieved a 90–99% reduction of the nidus, we achieved a 70–89% reduction in six sessions, a 50–70% reduction in four sessions, a 25–49% reduction in three sessions, and a <25% reduction in the remaining session. It should be noted that cure or maximal percentage of nidal reduction was not the goal of every treatment session. In larger AVMs, planned staging of embolization took place for some patients (eg, patient 17). In other patients the goal was embolization of arterial feeders that were felt to be difficult to access surgically prior to planned resection.
Case illustrations
Case 1
The patient presented with an unruptured 2.1 cm left inferior frontal Spetzler–Martin grade II AVM during investigation for headaches. This vascular malformation was fed by parasitized vessels from both the left anterior and middle cerebral arteries and drained primarily through the anterior third of the superior sagittal sinus. The patient had successful balloon-augmented embolization with Onyx via feeding pedicle from the distal left middle cerebral artery (MCA). Total time under fluoroscopy was 40 min and a >90% reduction of nidus was achieved. The patient subsequently underwent surgical resection with complete resection of the nidus seen on postoperative angiography. The patient was discharged on postoperative day 2 with no neurologic deficit (figure 1).

(A) Lateral projection of a left internal carotid artery (ICA) injection demonstrating 2.1 cm Spetzler–Martin grade II arteriovenous malformation (AVM). (B) Superselective angiography of the AVM with superior sagittal sinus drainage. (C) Lateral projection demonstrating post-embolization Onyx case of the AVM. (D) Final control angiogram demonstrating occlusion of flow into the AVM with preservation of the major cerebral vasculature.
Case 2
The patient presented with sudden onset of headache and nausea and on examination was found to have a cerebellar intraparenchymal hemorrhage. Further imaging revealed a left-sided 1.8 cm Spetzler–Martin grade II cerebellar AVM supplied by branches from the left superior cerebellar artery (SCA). The patient had balloon-augmented Onyx embolization of a feeding pedicle from the left SCA, as well as Onyx embolization through a Marathon microcatheter (Covidien) of an additional feeding pedicle from the left SCA. Total time under fluoroscopy was 48 min and a 70–89% reduction of the nidus was achieved. The patient was then medically optimized as an inpatient and underwent subsequent resection of the vascular malformation via craniotomy. The patient was discharged on postoperative day 8 neurologically intact (figure 2).

(A) Lateral projection of pretreatment left-sided 1.9 cm Spetzler–Martin grade II cerebellar arteriovenous malformation (AVM) supplied by branches from the left superior cerebellar artery (SCA). (B) Superselective angiography of the left SCA. (C) Post-Onyx treatment control angiogram demonstrating occlusion of inflow and no outflow from the AVM.
Case 3
The patient presented as an outpatient for an incidental finding of an AVM in the left posterior temporal-parietal region found on CT as part of an investigation for a traumatic concussion with resolution of symptoms. Digital subtraction angiography (DSA) revealed a 2.9 cm maximal diameter Spetzler–Martin grade III AVM. The patient had balloon-augmented Onyx embolization of the nidus via a left MCA feeding artery with a reduction in nidal filling of 70-89%. Total fluoroscopic time was 25 min. There were no procedure-related difficulties or complications. Surgical resection was planned for the following day and the patient was taken to recovery with orders for systolic blood pressure (SBP) goals 90–110 mm Hg. The immediate post-embolization neurological examination showed the patint was non-focal without aphasia or motor weakness. Despite a nicardipine infusion, the patient's blood pressure was not optimally controlled while in recovery with SBP reaching as high as 160 mm Hg. Approximately 2 h after completion of the procedure the patient suffered a sudden onset of severe headache, nausea, vomiting, and her neurological examination rapidly deteriorated with worsening global aphasia and decreased level of consciousness. 20 mg of protamine sulfate was administered intravenously and an emergency head CT revealed a parenchymal hemorrhage. The patient was taken as an emergency to the operating room for evacuation of the hemorrhage and resection of the AVM. There were no intraoperative difficulties and DSA 8 days later showed complete resection of the AVM. One-year follow-up showed that the patient had improved to a modified Rankin Scale (mRS) score of 1 with only mild difficulty with word finding during emotional excitement or stress with otherwise fluent speech. The hemorrhagic complication was not attributed to the Scepter device or the balloon-augmented technique but rather to poor post-embolization blood pressure control and retrospective recognition of partial embolization of the draining vein (figure 3).
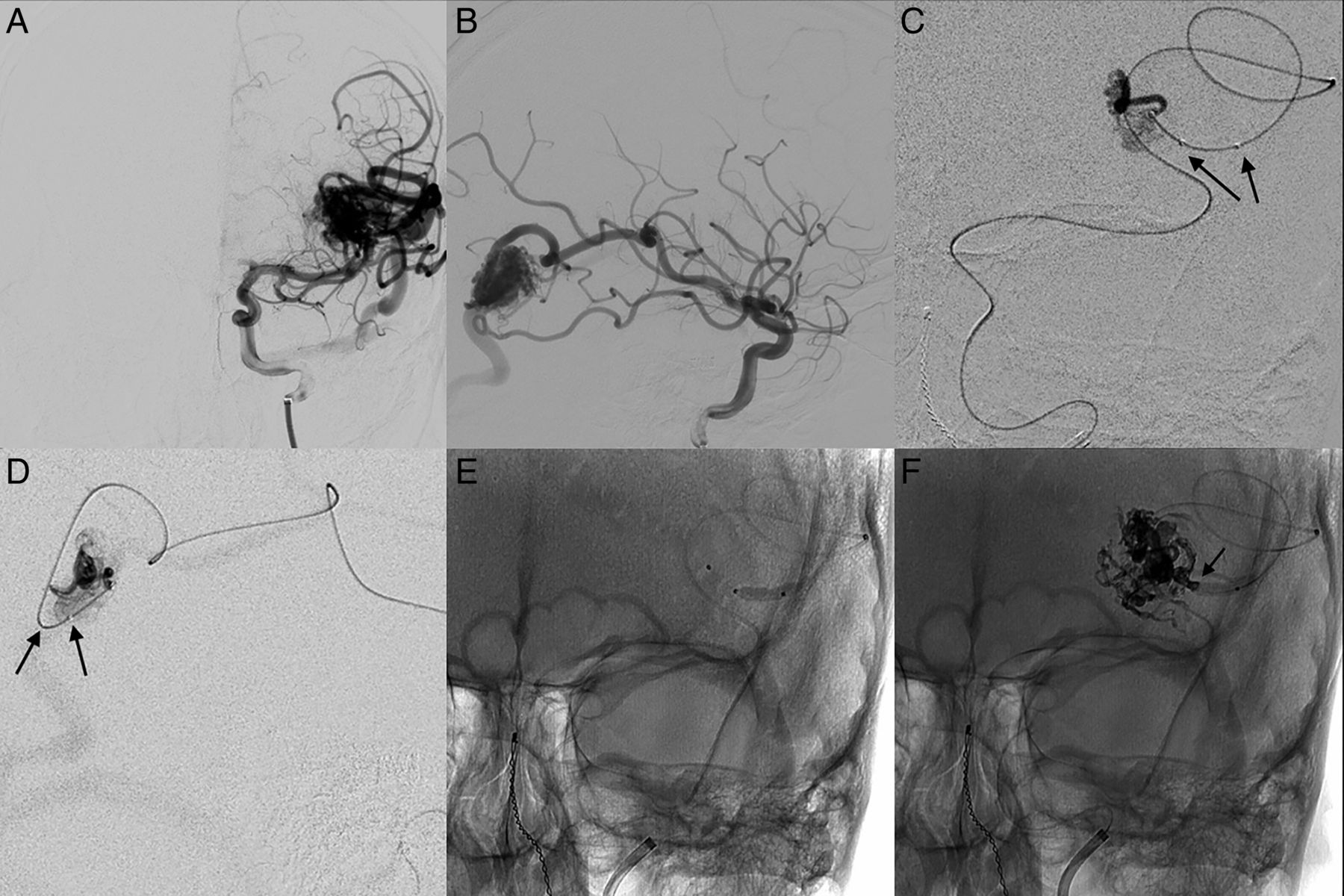
(A) Posterior-anterior (PA) and (B) lateral projection digital subtraction angiography (DSA) demonstrates a Spetzler–Martin grade III unruptured arteriovenous malformation (AVM). (C) PA and (D) lateral superselective angiography via the 4 mm×10 mm Scepter C microcatheter demonstrating distal placement of the balloon catheter tip within the AVM nidus with the balloon portion of the catheter remaining in the feeding arterial pedicle (arrows). Unsubtracted PA fluoroscopic images demonstrating inflation of the balloon catheter prior to (E) and after (F) Onyx embolization. Onyx cast is seen with reflux to the distal nose cone of the balloon (F, arrow). The balloon prevents further Onyx reflux.
Complications
In this series we report two complications directly referable to the Scepter device (8.3% of Scepter-related embolization procedure sessions, 5.4% of Scepter embolized pedicles). In the first patient, rupture of a feeding artery was secondary to the inflation of the Scepter balloon catheter itself. This patient had a baseline pre-procedural mRS score of 5 and was discharged with an mRS score of 3. Balloon inflation controlled the bleeding and embolization of the ruptured vessel addressed the complication. In the second patient the Scepter catheter was retained within the Onyx cast, fracturing during the attempt to remove it. This was directly related to reflux of embolisate beyond the proximal marker of the balloon catheter. There was no evidence of thrombosis related to the retained fragment or distal embolization on subsequent diagnostic runs, and a Neuroform 4 mm×15 mm stent was subsequently placed along the length of the fractured fragment, anchoring it against the arterial wall.
In another instance there was an episode of reflux which we did not attribute to failure of the Scepter device; this complication was related to Onyx reflux proximal to the balloon in the arterial pedicle of interest, but the reflux occurred in a retrograde fashion through the nidus of the AVM (distal to the position of the balloon catheter) via a nidal vessel connected to the proximal segment of the arterial pedicle and not around the balloon itself in the traditional sense. The balloon catheter was removed in this instance with some difficulty, and the patient did develop a new ipsilateral third nerve palsy that completely resolved within 30 days. There were no episodes of uninvolved territory infarction.
Clinical outcomes
In our 20 patients we report 10 patients where the mRS score was the same pre- and post-treatment. Five patients were seen with a worsening mRS post-procedurally, four patients with an improved mRS, and one did not have mRS data available. Of the five patients with a worsening mRS, none had complications felt to be referable to the Scepter C device. Three of the five patients worsened minimally from an mRS score of 0 to 1. Only one patient without pre-procedure disability had post-procedure disability (mRS 1–3).
Of the two patients with complications felt to be referable to the device itself, one patient improved from an mRS score of 5 on admission to an mRS score of 3 on discharge, and another was discharged with the same mRS score of 1 as at presentation.
Discussion
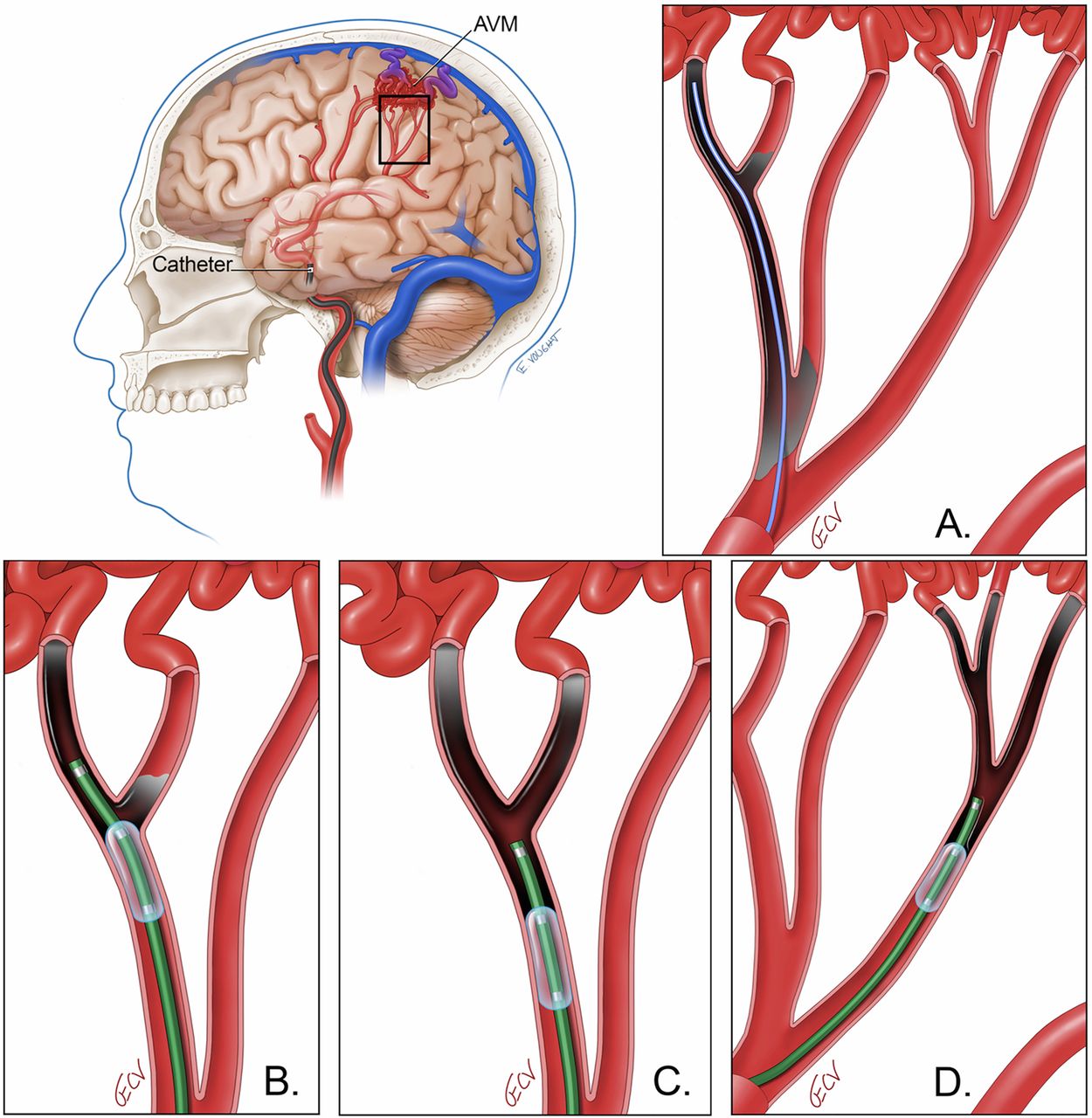
Onyx has gained widespread popularity as an embolisate material for endovascular embolization of intracranial AVMs. Onyx is a cohesive polymer which polymerizes when put in contact with an ionic solution (such as plasma). The cohesive nature (as opposed to adhesive) confers great advantage in terms of ability to start and stop injection and thus control for unsatisfactory flow of embolisate.11 However, the ability to control the direction of Onyx flow remains a challenge. This challenge is traditionally overcome by forming a ‘proximal plug’ of Onyx slowly at the tip of the microcatheter, which is often a time-consuming and unpredictable process (figure 4). This process leads to a long slow push of the Onyx embolisate which, in turn, results in longer procedural times and increased times under fluoroscopy for both the patient and the surgeon.12 ,13 Reflux of Onyx proximally may lead to non-targeted embolization as well as obstruction of another intended arterial feeder, precluding optimal embolization.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Illustration of a cerebral arteriovenous malformation (AVM) from a lateral view with arterial feeders arising from the middle cerebral artery. (B) The conventional method of Onyx embolization employs a microcatheter which is positioned distally within the pedicle. Long procedure and fluoroscopy times may be required to produce a sufficient ‘proximal plug’ before penetration of the nidus is achieved. Despite these efforts, reflux of the embolisate proximally limits the amount of nidal penetration and can block access to other potential arterial feeders. (C) On the other hand, a dual-lumen balloon catheter does not need to be delivered as far distally within the pedicle since balloon inflation greatly minimizes the concern for proximal reflux. In this example the catheter tip is positioned in one pedicle while the balloon is inflated proximal to the bifurcation of a second pedicle. Balloon inflation leads to Onyx penetration in both pedicles simultaneously. (D) Alternatively, the dual-lumen balloon catheter can be positioned so that both the distal tip and the inflated portion (first and second radiopaque markers) remain just proximal to a bifurcating segment of an arterial feeder to achieve simultaneous embolization of the two branches. (E) Lastly, balloon-augmented embolization allows for efficient Onyx penetration across first and second order branches of an arterial pedicle, even from a relatively proximal position, while providing protection from reflux.
It has been demonstrated that an inflated Scepter C balloon microcatheter can act as a surrogate for the ‘proximal plug’ of Onyx,8–10 allowing for a safer, more controlled injection of Onyx into the pedicle of interest. By acting as the proximal plug, the balloon microcatheter theoretically obviates the need for the formation of a de novo plug of Onyx, resulting in a much shorter time under fluoroscopy and a reduced risk of embolisate reflux. Additionally, Crowley et al11 suggest that the Scepter C balloon microcatheter holds promise in the embolization of high-flow AVM pedicles, allowing a mechanism to arrest the proximal flow from the arterial pedicle, thus decreasing the likelihood of inadvertent embolization of draining veins.
In our experience with the Scepter C microcatheter in the treatment of cerebral AVMs, we have observed many of the aforementioned theoretical advantages to be true. In our multicenter series of 20 patients we noted no episodes of reflux directly past the nose cone of the Scepter balloon. We noted a mean time under fluoroscopy of just 48 min per procedure and 28 min per pedicle, which anecdotally is much lower than the times we traditionally observe using traditional microcatheter systems to deliver Onyx embolisate to AVMs. Indeed, in a study comparing n-butyl cyanoacrylate embolization with Onyx embolization of intracranial AVMs, Velat et al13 reported a mean time under fluoroscopy of 135±65 min for Onyx embolization, which is significantly higher than that observed in our experience. However, direct comparison of fluoroscopy times between patients treated both with and without the Scepter C device is challenging, if not impossible, given disparities in angiographic anatomy, complexity, size discrepancies of AVMs as well as operator-related radiation practices. Because of the retrospective nature of our analysis, the actual time of embolization was not routinely documented and thus is not included in our review.
We demonstrate that the Scepter C device can be used safely for the embolization of intracranial AVMs with Onyx. Earlier reports contain only a small number of isolated cases in which the Scepter C catheter is used to deliver Onyx to intracranial AVMs.8 ,10 ,14 Most previously reported cases involved embolization of lesions via the external carotid vasculature, which is considered more robust than the cerebral vasculature. We describe the largest number of patients with cerebral AVMs to date treated with the Scepter C dual-lumen device across four centers by different physicians with only two complications felt to be related to the Scepter C device itself. Additionally, one of these complications—namely, retention of the microcatheter in an Onyx cast—can also seen with other microcatheter devices.12 ,15 While pedicle rupture via balloon inflation is not seen with other microcatheter systems, arterial rupture is still a recognized complication of AVM embolization performed with other devices.16 However, as in balloon-assisted coiling of aneurysms, the Scepter device allows for immediate proximal control in cases of arterial rupture due to balloon overinflation, offering a distinct advantage over other microcatheter systems in cases of this particular complication. The other published experiences by Jagadeesan et al and Paramasivam et al report similar complications.10 ,14 Jagadeesan et al reported one instance of pericallosal artery rupture from overinflation of the Scepter C balloon which they then addressed in future patients by using strict matching of balloon inflation diameter to the diameter of the arterial pedicle seen on roadmap.
Conclusion
This multicenter experience with AVM embolization demonstrates that using a dual-lumen balloon catheter as an adjunct for Onyx embolization is safe and effective, resulting in satisfactory reduction of the AVM nidus with an acceptable complication rate. This technique may allow for shorter procedure times and lower doses of radiation, but further work is needed to validate this.
References
Footnotes
Contributors All authors made a material contribution to this article, the revision of the article, and the final approval of the article for submission to this journal.
Competing interests A. Spiotta: Consultant/Advisory Board; Modest; Microvention, Stryker, Penumbra, Pulsar. R. Turner: Speakers' Bureau; Modest; Microvention, Stryker, Siemens, Penumbra. A. Turk: Research Grant; Modest; Microvention. Speakers' Bureau; Modest; Microvention, Penumbra, Siemens. Honoraria; Modest; Microvention, Stryker. Consultant/Advisory Board; Modest; Stryker. M. Chaudry: Consultant/Advisory Board; Modest; Microvention, Stryker, Penumbra. R. James: Research Funding; Modest; Microvention, Penumbra. Stock Interest; Modest; Remedy Pharmaceuticals, Inc. Janjua: Consultant; Covidien.
Ethics approval Ethics approval was obtained from Medical University of South Carolina Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.